Cannabis Withdrawal: The Complete Science-Based Guide

What the Research Says
47%
of frequent cannabis users experience clinically significant withdrawal when they stop
JAMA Network Open, 2020 — 23 studies, 27,000+ participants
Day 4–6
symptom peak
2–4 weeks
most symptoms resolve
Day 28
full receptor recovery
If you only read one thing
If you quit weed and feel awful right now — can't sleep, can't eat, snapping at everyone — that's withdrawal, and it's completely normal. About half of regular users go through this. The worst part hits around days 3 to 6, then it starts getting better. Most symptoms clear up within 2 to 4 weeks, though sleep can take up to 6 weeks to fully bounce back. It's real, it's temporary, and your brain is actively repairing itself the whole time.
If you stopped smoking and now you cannot sleep, cannot eat, and feel like you are losing your mind, you are not broken. You are in withdrawal. Cannabis withdrawal is a clinically recognized medical condition that affects nearly half of frequent users, and the fact that you feel terrible right now is actually your brain doing exactly what it is supposed to do. Here is what is happening, why it is happening, and when it stops.
Key Takeaways
- Cannabis withdrawal is a real medical condition — it has been in the DSM-5 since 2013
- Nearly half of frequent cannabis users (about 47%) get withdrawal symptoms when they stop
- Symptoms usually peak around days 3 to 7, and most clear up within 2 to 4 weeks
- Sleep problems hang on the longest, sometimes lasting up to 45 days
- Unlike alcohol or benzodiazepine withdrawal, cannabis withdrawal is uncomfortable but never medically dangerous
- Your CB1 receptors start rebuilding within 2 days and get back to normal by about day 28
What You Are Going Through Is Real
For years, people were told cannabis was not addictive and that quitting had no physical effects. If you believed that and then tried to stop, the experience probably felt confusing and isolating. You might have wondered if something else was wrong with you.
In 2013, cannabis withdrawal was officially added to the DSM-5. That is the Diagnostic and Statistical Manual of Mental Disorders, the book that every psychiatrist and therapist in the country uses to diagnose conditions. (For a closer look at what the diagnostic criteria actually say, see our DSM-5 deep dive.) It is the same manual that contains depression, anxiety, PTSD, and every other recognized mental health condition. Cannabis withdrawal is in there because the evidence became impossible to ignore.
A 2020 meta-analysis published in JAMA Network Open analyzed data across 23 studies involving over 27,000 participants and found that 47% of frequent cannabis users experience clinically significant withdrawal symptoms when they stop.[1] That is nearly one in two people. If you are one of them, you are not weak and you are not imagining things. Your brain physically adapted to regular THC, and now it is readjusting.
Here is what that withdrawal process looks like from start to finish.
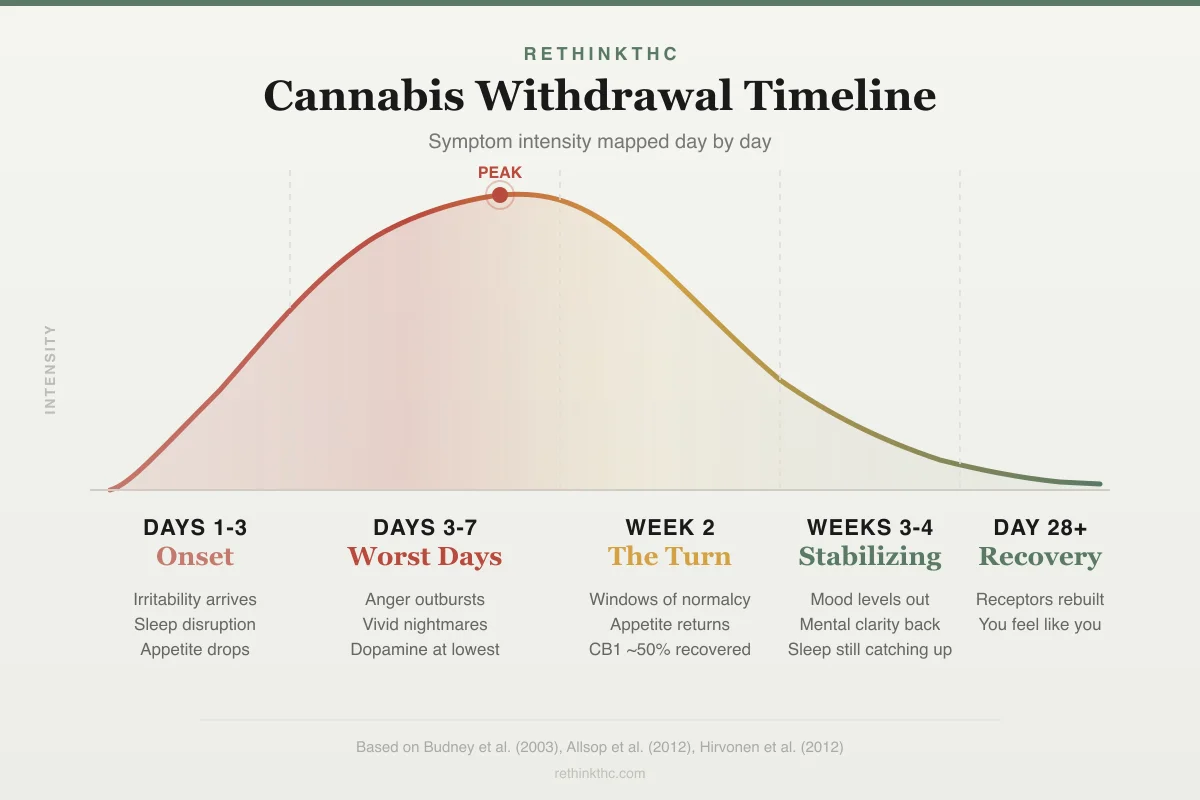
Symptom Intensity by Phase
Cannabis Withdrawal Timeline
Days 1-3
Onset
Days 3-7
Worst Days
Week 2
The Turn
Weeks 3-4
Stabilizing
Day 28+
Recovery
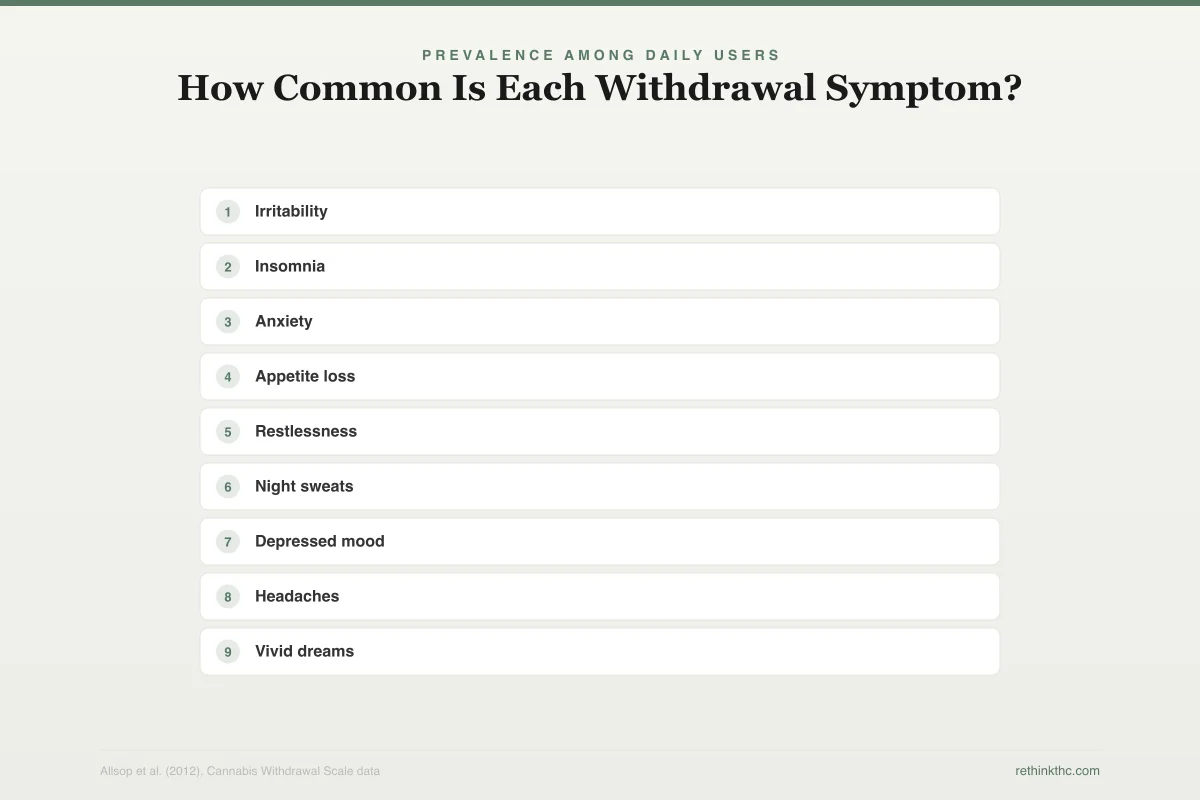
The chart below shows how common each withdrawal symptom actually is among people going through this process.
Prevalence Among Daily Users
How Common Is Each Withdrawal Symptom?
Percentage of daily cannabis users reporting each symptom during withdrawal
Key finding: Nearly 4 in 5 daily users report irritability as their primary withdrawal symptom. Most people experience 3+ symptoms simultaneously.
What Is Actually Happening in Your Brain
Here is the short version: your brain has a built-in cannabis system. It is called the endocannabinoid system, and it was there long before you ever touched weed. It helps regulate mood, sleep, appetite, pain, and stress using chemicals your body produces naturally.
When you use cannabis regularly, THC floods this system from the outside. Your brain responds the way it responds to any surplus: it turns down its own production and reduces the number of receptors available. Specifically, it reduces something called CB1 receptors, which are the docking stations where THC attaches to produce its effects. Think of it like this: if someone is constantly shouting in your ear, you start wearing earplugs. Your brain is doing the same thing with THC.
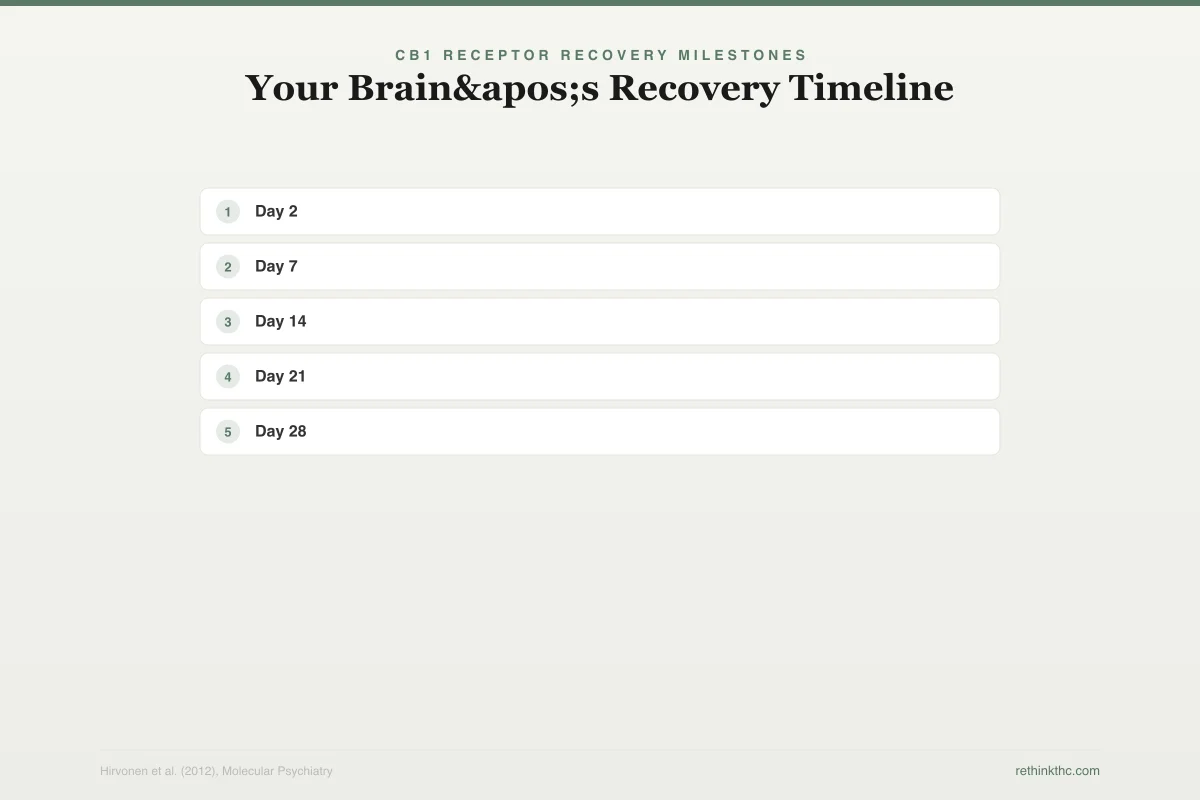
A 2012 study in Molecular Psychiatry used PET brain imaging to confirm that CB1 receptor levels start recovering within just two days of quitting and return to normal levels by about day 28.[2] That is the biological basis for why withdrawal follows a predictable timeline. Your brain is literally rebuilding the hardware that THC wore down.
When you suddenly stop using cannabis, your brain is caught in a gap. The external THC is gone, but the internal system has not finished repairing itself yet. That gap is withdrawal. Every symptom you feel maps to a specific part of this recovery process. Here is what that receptor recovery looks like over time.
CB1 Receptor Recovery Milestones
Your Brain's Recovery Timeline
CB1 receptor density returns to non-user levels by ~Day 28
The Cannabis Withdrawal Timeline: What to Expect Each Week
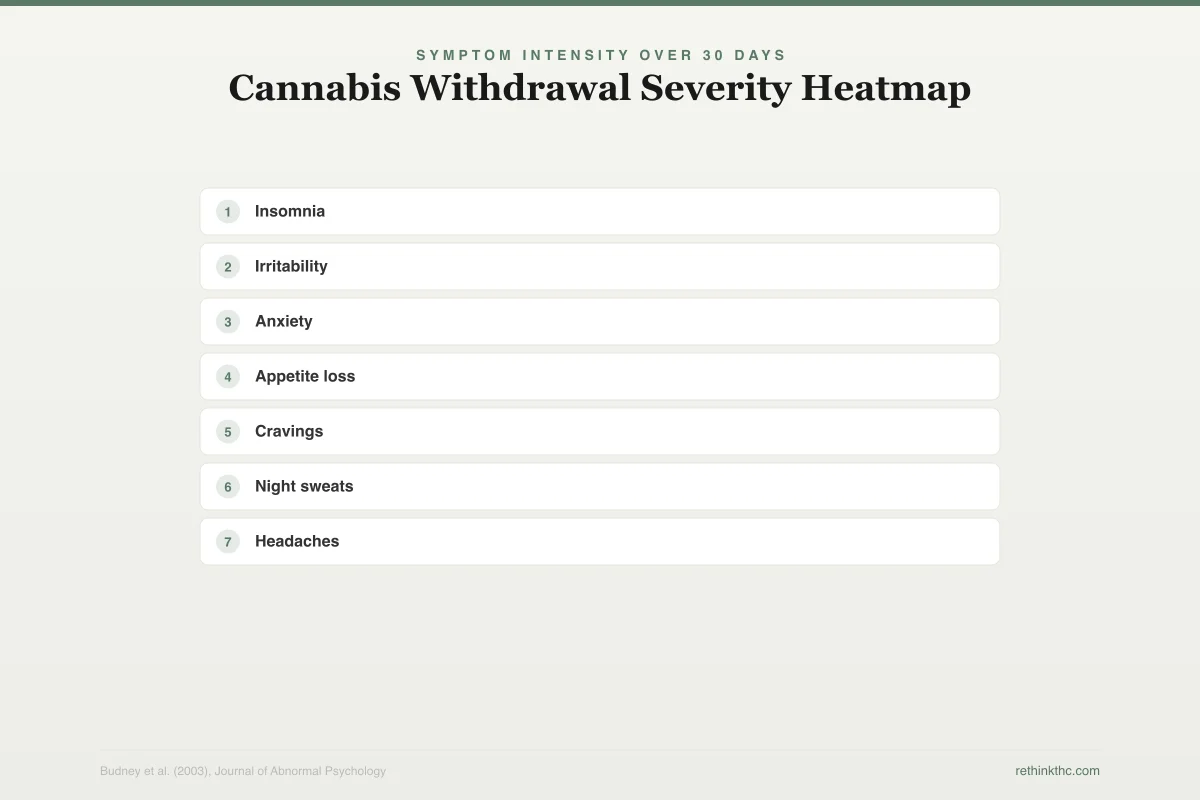
Everyone's experience is slightly different depending on how much you used, how long you used, and the potency of what you were using. But research consistently shows a predictable general pattern.[3] The heatmap below shows how symptom severity shifts across each phase of withdrawal.
Symptom Intensity Over 30 Days
Cannabis Withdrawal Severity Heatmap
Days 1 to 3: It Hits Faster Than You Expect
Most people notice something within the first 24 hours. You might feel restless, irritable, or just "off." Sleep is usually the first thing to go. A 2004 review by Budney and colleagues confirmed that withdrawal onset typically occurs within 24 to 72 hours of cessation, with most users reporting symptoms by the end of the first day.[4][16] We cover every detail of that first week in a separate guide.
People in cannabis recovery communities frequently describe the first few days as feeling like a low-grade flu combined with an emotional short fuse. You might snap at someone over nothing, feel weirdly anxious in situations that never bothered you, or notice that food has no appeal. All of this is normal.
Days 3 to 7: The Peak
This is the hardest part. If you are reading this from the middle of it, know that you are at the worst point and it does get better from here.
A 2003 controlled-abstinence study published in the Journal of Abnormal Psychology confirmed that symptom severity peaks between days two and six.[3] Your brain is in the most active phase of recalibration. The gap between "THC is gone" and "my own system is back online" is at its widest.
During this window, irritability can feel overwhelming. A lot of people describe sudden anger that feels disproportionate to whatever triggered it. Cravings are at their strongest. Sleep may be broken or absent entirely, and when you do sleep, your dreams can be startlingly vivid. Night sweats are common. Some people experience stomach cramps, nausea, or headaches.
One experience that comes up constantly in online recovery communities: the mood swings. You might feel fine for two hours, then suddenly feel crushing sadness or anxiety for no identifiable reason. This is your brain's emotional regulation system coming back online after months or years of THC handling that job. It overshoots before it stabilizes.
Days 7 to 14: The Turn
Somewhere in the second week, most people notice a shift. The irritability starts fading. Appetite creeps back. The cravings are still there, but they lose their urgency. You start having stretches of feeling genuinely okay.
Sleep is still rough for most people at this stage. You are sleeping more than during the peak, but the quality is poor and the dreams are intense. This is the phase where many people make the mistake of thinking they should be fully better and get discouraged that they are not. The timeline is weeks, not days.
Days 14 to 30: Stabilization
By the end of the third week, most acute symptoms have resolved or significantly diminished.[3] Mood is more stable. Appetite is closer to normal. Many people describe a growing sense of mental clarity during this phase, like a fog lifting that they did not realize was there.
The main holdout is sleep. Sleep disturbances are consistently the longest-lasting withdrawal symptom. Clinical research, including controlled abstinence studies and a systematic review of cannabis withdrawal and sleep, has found that sleep disruption can persist for 40 to 45 days after quitting.[5][15] Understanding this timeline prevents the common trap of relapsing at week three because you think your sleep will never recover. It will. It takes longer than everything else.
Beyond Day 30: The Long Tail
For heavy, long-term users, some symptoms can linger past the one-month mark. Intermittent cravings, occasional sleep disruption, and brief periods of low motivation are the most common. Some researchers refer to this as post-acute withdrawal syndrome (PAWS), though this term is borrowed from alcohol research and is not formally recognized in cannabis-specific literature.
The key distinction: these lingering symptoms are mild compared to the acute phase. They are inconvenient, not debilitating. And they do eventually resolve completely.
Every Symptom Explained
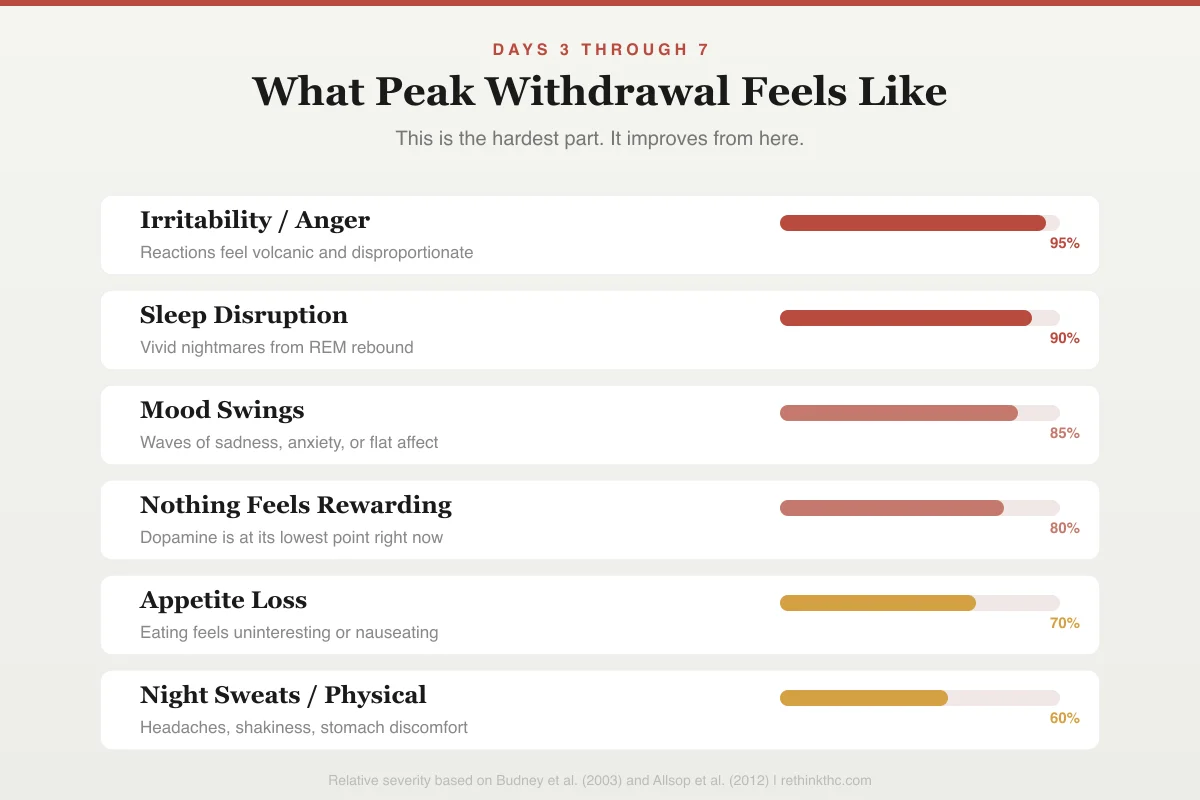
The DSM-5 identifies specific symptoms as diagnostic criteria for cannabis withdrawal. You need to experience at least three of these within a week of stopping or significantly reducing your use. These are the symptoms that hit hardest during the peak window.
Days 3 Through 7
What Peak Withdrawal Feels Like
This is the hardest part. It improves from here.
Irritability / Anger
Reactions feel volcanic and disproportionate
Sleep Disruption
Vivid nightmares from REM rebound
Mood Swings
Waves of sadness, anxiety, or flat affect
Nothing Feels Rewarding
Dopamine is at its lowest point right now
Appetite Loss
Eating feels uninteresting or nauseating
Night Sweats / Physical
Headaches, shakiness, stomach discomfort
| Symptom | How Common | Typical Duration | Mechanism |
|---|---|---|---|
| Irritability / anger | ~70% of cases | 1–2 weeks | Emotional thermostat recalibrating without THC's amygdala dampening |
| Anxiety / nervousness | ~50–60% | 1–3 weeks | Amygdala running at full sensitivity without THC suppression |
| Sleep difficulty | ~45–65% | 2–6 weeks | REM rebound + circadian rhythm disruption |
| Decreased appetite | ~40–50% | 1–2 weeks | Loss of THC-driven CB1 appetite stimulation |
| Depressed mood | ~35–50% | 1–3 weeks | Dopamine system below baseline before natural recovery |
| Restlessness | ~35–45% | 1–2 weeks | Autonomic nervous system recalibration |
| Physical symptoms | ~20–30% | 1–2 weeks | Abdominal pain, sweating, headaches, chills |
Prevalence rates derived from Bahji et al. 2020[1] and Schlienz et al. 2017.[12]
Irritability, anger, or aggression. This is the most commonly reported symptom. Your brain's emotional thermostat has been calibrated to include THC. Without it, emotions run hotter than your baseline. It normalizes, but for the first week or two, people around you may notice before you do.
Anxiety or nervousness. THC activates calming receptors in your amygdala, the brain region that processes threat and fear. When THC is removed, your amygdala runs at full sensitivity again.[14] Situations that felt manageable while using may temporarily feel overwhelming. For a deep dive, see Weed and Anxiety: The Paradox That Traps People.
Sleep difficulty. This includes trouble falling asleep, waking up throughout the night, and the vivid dream phenomenon known as REM rebound. THC suppresses REM sleep (the dreaming stage), and when you quit, your brain overcompensates with a surge of intense dreaming. This is one of the most distinctive features of cannabis withdrawal.
Decreased appetite or weight loss. THC stimulates appetite through direct receptor activation (this is the mechanism behind "the munchies"). Without it, your hunger signals temporarily drop below normal. Most people see appetite return within the first two weeks.[1]
Depressed mood. This is partly related to dopamine system recalibration. THC artificially boosts dopamine (the brain chemical linked to reward and motivation). When you stop, your dopamine levels dip below your natural baseline before recovering. Things that used to feel enjoyable may temporarily feel flat or pointless.
Restlessness. A physical sense of agitation or inability to sit still. This tends to peak in the first week and resolve by week two.
Physical symptoms. Abdominal pain, sweating, shakiness, headaches, chills, and low-grade fever. These are less common than the psychological symptoms but are well-documented and resolve within the first two weeks for most people.
Symptoms the DSM-5 Does Not List (But You Might Still Experience)
The DSM-5 criteria are a diagnostic minimum, not a complete inventory. Clinical research and large-scale surveys document several additional symptoms that are common, well-studied, and completely consistent with cannabis withdrawal.[12] If you are experiencing any of these, you are not an outlier. The manual is just narrower than your experience.
Night Sweats
You wake up drenched, sometimes multiple times a night. This is your autonomic nervous system (the part of your brain that controls automatic functions like body temperature and heart rate) recalibrating without THC's regulatory input. THC dampens the sympathetic nervous system, which controls your "fight or flight" responses. When it is removed, that system temporarily overreacts, producing excess sweating. Research suggests that cannabis modulates parasympathetic nervous system activity, and withdrawal may trigger a rebound in autonomic signaling.[13] Night sweats are most intense during the first week and typically resolve by week two or three. The Cannabis Withdrawal Scale developed by Allsop and colleagues lists night sweats and strange dreams as among the most diagnostically useful withdrawal symptoms.[6]
Emotional Flooding and Crying Spells
You tear up at a commercial. You feel a wave of sadness that has no cause. You snap at someone, then feel crushing guilt about it ten minutes later. People in cannabis recovery communities describe this as one of the most confusing symptoms because it feels like an emotional disorder, not withdrawal. It is not. THC partially takes over emotional regulation by blunting activity in your amygdala. A 2017 study in Neuropsychopharmacology confirmed that THC directly modulates anxiety responses through amygdalar CB1 receptors, meaning that removing THC leaves the amygdala processing emotions at full volume again.[14] The reversal is not instant. It overshoots, stabilizes, and typically normalizes by weeks two to three.
Brain Fog and Concentration Problems
You cannot focus. You read the same paragraph three times. Tasks that used to be automatic now require conscious effort. THC impairs working memory through CB1 receptor activation in the prefrontal cortex. A 2018 meta-analysis in JAMA Psychiatry found measurable cognitive deficits in heavy cannabis users that largely resolved within 72 hours to three weeks of abstinence.[7] The timeline depends on duration and intensity of use, but the trajectory is consistently toward full recovery.
Vivid Nightmares
This goes beyond the REM rebound discussed in the sleep section. Some people do not just dream vividly — they have nightmares intense enough to wake them in a panic with a racing heart. This happens because REM rebound does not filter for content. Your brain is producing more dreams, longer dreams, and more emotionally charged dreams all at once. A 2016 systematic review of cannabis withdrawal and sleep confirmed that sleep disturbance, including intense dreaming, is among the most persistent and clinically significant withdrawal symptoms.[15] Trauma survivors or people with underlying anxiety may find this particularly distressing. It is the single most commonly cited reason for relapse in the first two weeks. If nightmares are severe enough to prevent you from sleeping at all, a healthcare provider can help.
Derealization and Depersonalization
Things feel unreal, like you are watching your life through a screen. Or you feel disconnected from your own body, like your hands are not quite yours. This is alarming when it happens, but it is a documented feature of cannabis withdrawal, not a psychotic break. THC modulates sensory processing and self-referential thought through CB1 receptors in the default mode network. When those receptors are in flux, your subjective experience of reality can temporarily feel distorted. A 2017 review of cannabis withdrawal syndrome confirmed that perceptual disturbances including derealization are recognized clinical features of withdrawal.[16] It is most common during the peak phase (days three to seven) and typically resolves within two weeks. For more, see our article on weed and depersonalization.
Anhedonia and Boredom
Nothing feels fun. Music sounds flat. Food is boring. Activities you used to enjoy feel pointless. This maps directly to dopamine system recalibration. THC increases dopamine release in the nucleus accumbens (the brain's primary reward center). When you stop, your reward system temporarily drops below its natural baseline. Animal research suggests that THC withdrawal reduces motivation for natural rewards through mesolimbic dopamine dysregulation.[17] The world is not actually less interesting — your brain is temporarily less capable of registering interest. This is one of the slower symptoms to resolve, typically improving between weeks two and four, with full normalization by weeks six to twelve.
Coughing and Lung Clearing (for Smokers)
If you smoked cannabis, you may experience increased coughing, phlegm production, and throat irritation after quitting. This is not withdrawal in the neurological sense — it is your lungs physically clearing accumulated resin and damaged cells. Your respiratory epithelium begins repairing itself within days of stopping smoke inhalation. The coughing can be worse before it gets better as your lungs clear out debris. This typically resolves within two to four weeks. For a detailed breakdown of the lung recovery process, see our lung recovery after quitting guide.
Fatigue and Low Energy
Despite not sleeping well, or sometimes because of it, you feel exhausted in a way that sleep does not fix. This is partly sleep quality related and partly a consequence of your endocannabinoid system being offline. The endocannabinoid system plays a role in energy regulation and alertness. During withdrawal, you lose the stimulating effects of THC-driven dopamine release without yet having your natural system back at capacity. Most people report energy levels normalizing by the end of week two, with continued improvement through week four.
Gastrointestinal Issues Beyond Appetite Loss
Nausea, cramping, diarrhea, or general digestive discomfort. Your gut has its own dense network of CB1 receptors. THC directly modulates gut motility, acid secretion, and inflammatory responses.[18] When it is removed, your digestive system recalibrates just like your brain does. These symptoms are most common in the first week and typically resolve by day 10 to 14.
Tinnitus (Ringing in the Ears)
Some people report a new or worsened ringing, buzzing, or hissing sound in their ears during the first week or two. CB1 receptors are present in the auditory cortex and cochlear nucleus. Changes in receptor activity during withdrawal may temporarily alter auditory processing. It typically resolves within two to three weeks.
Why Some People Get Hit Harder Than Others
Not everyone experiences the same severity. Several factors predict how intense your withdrawal will be. Research on withdrawal severity predictors has identified the following key variables:[8][12]
| Risk Factor | Effect on Withdrawal |
|---|---|
| Daily use | More consistent THC exposure → more receptor downregulation → bigger gap when you stop |
| High-potency products (concentrates, dabs) | 80%+ THC concentrates cause greater CB1 changes than 15% flower |
| Longer duration of use | 5 years daily > 3 months daily — neurological adaptation deepens over time |
| Concurrent tobacco use | Nicotine and THC interact in reward circuitry; dual withdrawal compounds symptoms |
| Genetics | Some endocannabinoid systems recover faster — still being quantified by researchers |
| Higher pre-quit use frequency | More sessions per day = higher baseline THC saturation |
| Female sex | Women may experience more severe withdrawal symptoms on average[12] |
A 2012 study using the Cannabis Withdrawal Scale found that withdrawal severity was significantly linked to relapse risk — people whose withdrawal disrupted their daily functioning were more likely to return to cannabis use, making early intervention and symptom management critical.[9]
What You Can Do Right Now
You cannot speed up your brain's receptor recovery. That process runs on its own biological clock. But you can significantly reduce how miserable the process feels. Here is what to focus on during each phase of recovery.
Quick Reference
Where Are You Right Now?
Match your symptoms to your phase
Days 1-3: Onset
If you're feeling...
- ☐Mild restlessness or edginess
- ☐Starting to snap at people
- ☐Trouble falling asleep
- ☐Food sounds unappealing
Peak is coming in 1-3 days. Set up your space now.
Days 3-7: Peak
If you're feeling...
- ☐Anger that feels out of control
- ☐Intense or disturbing dreams
- ☐Nothing feels fun or interesting
- ☐Night sweats, can't eat
This is the worst of it. It starts easing in days.
Week 2: The Turn
If you're feeling...
- ☐Moments where you feel normal
- ☐Actually hungry again
- ☐Cravings feel like suggestions
- ☐Less reactive to frustration
You're past the worst. Brain is 50-60% rebuilt.
Weeks 3-4: Recovery
If you're feeling...
- ☐Stable mood most of the day
- ☐Sharper focus and memory
- ☐Enjoying things again
- ☐Sleep still not perfect
CB1 receptors near normal. Sleep is last to heal.

Exercise is the single most evidence-supported intervention. A 2012 study in Psychoneuroendocrinology demonstrated that aerobic exercise triggers endocannabinoid release in humans — the same system that THC hijacks — providing natural mood elevation through your body's own chemistry.[10] Even a 20-minute walk measurably improves mood during withdrawal. You do not need to run a marathon. Moving your body tells your brain to produce the chemicals it is currently short on. For a detailed guide, see quitting weed and exercise.
Protect your sleep environment. You cannot force good sleep during withdrawal, but you can stop making it worse. Keep your room cool (65–68°F / 18–20°C) and dark. Avoid screens for 30 minutes before bed. Stick to the same sleep and wake times every day, even on weekends. Your circadian rhythm is recalibrating, and consistency helps it find its new baseline faster. For comprehensive strategies, see how to sleep without weed.
Eat even when you are not hungry. Your appetite signals are suppressed, but your body still needs fuel. Small, easy meals (toast, bananas, soup) are better than skipping meals entirely. Dehydration worsens headaches and irritability, so water intake matters more than usual during this phase.
Tell someone what you are going through. Isolation makes every symptom worse. You do not need to announce it publicly, but having one person who understands why you are irritable, not sleeping, and not yourself takes pressure off the process. People in cannabis recovery communities consistently identify social support as the factor that most influenced whether they made it through the first two weeks.
Track your symptoms. A simple daily note of what you are feeling serves two purposes. First, it gives you evidence that you are improving, which is hard to see when you are in it. Second, it prevents the common distortion of thinking today is as bad as day three when it measurably is not. Our withdrawal tracker can help with this.
Medications and Supplements That May Help
No medication is FDA-approved specifically for cannabis withdrawal, but several options have shown promise in clinical research. Always consult a healthcare provider before starting any medication during withdrawal.
| Option | What It Does | Evidence Level |
|---|---|---|
| Gabapentin | Reduces anxiety, improves sleep, may ease irritability | Moderate — shown to reduce withdrawal symptoms in clinical trials |
| N-acetylcysteine (NAC) | Antioxidant that modulates glutamate; may reduce cravings | Mixed — some positive results in adults, but the largest youth trial found no benefit over placebo[11] |
| Melatonin | Supports sleep onset during withdrawal insomnia | Low–moderate — helpful for circadian disruption, limited cannabis-specific data |
| OTC sleep aids (diphenhydramine, doxylamine) | Short-term sleep support | Low — can help acutely but not recommended beyond 1–2 weeks |
| Magnesium glycinate | May reduce anxiety, muscle tension, and improve sleep quality | Low — general evidence, not cannabis-specific |
| CBD | May reduce anxiety without THC's psychoactive effects | Emerging — some concerns about triggering cravings; see our CBD guide |
| CBT-I (Cognitive Behavioral Therapy for Insomnia) | Gold standard for insomnia treatment | Strong — effective for withdrawal-related insomnia specifically |
For a detailed look at supplement options, see supplements for weed withdrawal. For medication interactions, see quitting weed and medication interactions.
Safety
ModerateWhen withdrawal needs professional support
Concern
While cannabis withdrawal is not medically dangerous, severe anxiety, depression, or persistent insomnia can significantly impact daily functioning. In rare cases, withdrawal can worsen pre-existing psychiatric conditions or trigger thoughts of self-harm.
What the research says
Most people get through withdrawal without medical help. But severity varies widely — the 2020 Bahji meta-analysis found that 87% of inpatient populations experienced withdrawal, suggesting a subset of users faces much harder recoveries.
Particularly relevant for: Heavy daily users, people with pre-existing anxiety or depression, and those who have failed previous quit attempts
What to do
If insomnia lasts beyond 6 weeks, if anxiety or depression interferes with daily life, or if you experience any thoughts of self-harm, seek help immediately. SAMHSA's helpline (1-800-662-4357) is free and available 24/7.
Bahji et al. (2020), JAMA Network Open; DSM-5 diagnostic criteria
When to Seek Professional Help
Cannabis withdrawal is not medically dangerous. It does not carry the seizure risk of alcohol withdrawal or the life-threatening potential of opioid or benzodiazepine withdrawal. But "not dangerous" does not mean "easy," and some people experience symptoms severe enough to warrant professional support. To put cannabis withdrawal in context, here is how it compares to withdrawal from other substances.
Withdrawal Comparison
Cannabis vs Other Substance Withdrawals
Cannabis withdrawal is uncomfortable but never medically dangerous
Important: Alcohol withdrawal can cause life-threatening seizures. Unlike cannabis, alcohol and benzodiazepine withdrawal may require medical supervision.
Seek help if:
- Insomnia persists beyond six weeks with no improvement
- Anxiety or depression is severe enough to interfere with work, self-care, or relationships
- You experience thoughts of self-harm at any point
- You have a history of psychiatric conditions that are worsening during withdrawal
- Previous quit attempts have failed due to symptom severity
A therapist experienced in substance use can help. Cognitive behavioral therapy has strong evidence for treating both withdrawal-related anxiety and insomnia specifically.
If you experience thoughts of self-harm at any point, reach out immediately. SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day. You can also text HOME to 741741 to reach the Crisis Text Line.
The Bigger Picture
Most people who go through cannabis withdrawal were told it would not happen. They were told cannabis is not addictive, that quitting is effortless, that withdrawal is not a real thing. Then they tried to stop and their body told them a different story. That disconnect between expectation and reality makes the process harder than it needs to be.
Now you know the science. You know your brain adapted to THC, and it is actively repairing itself on a timeline measured in weeks, not months. You know the peak is early and the trajectory is toward recovery. You know the specific symptoms and why each one happens. That understanding does not make withdrawal painless, but it makes it predictable. And predictable is manageable.
The people who get through withdrawal successfully are not the ones who feel nothing. They are the ones who understand what they are feeling, know it has a biological cause, and know it has a biological end date. You now have that information. The next few weeks will be uncomfortable. They will not be permanent. And on the other side of them is a version of your brain that works the way it was designed to, without needing anything from the outside to function. For a step-by-step plan to get through it, see our guide on how to quit weed.
Explore Cannabis Withdrawal
Withdrawal Basics
- Cannabis Withdrawal Syndrome: Why It's Real and What Science Says
- Marijuana Withdrawal Symptoms: Every Symptom Explained
- Cannabis Withdrawal Syndrome: A DSM-5 Deep Dive
- Mild vs Moderate vs Severe Cannabis Withdrawal
- How to Deal with Weed Cravings: Practical Strategies
Physical Symptoms
- Night Sweats After Quitting Weed
- Weed Withdrawal Night Sweats: What's Happening to Your Body
- Weed Withdrawal Headaches: Causes and Relief
- Weed Withdrawal Nausea: Why Your Stomach Is a Wreck
- Weed Withdrawal Appetite Loss: When Food Feels Impossible
- Why You Can't Eat After Quitting Weed
- Weed Withdrawal and Sweating: Why Your Body Is Detoxing
- Weed Withdrawal Chest Tightness and Heart Palpitations
- Weed Withdrawal and Caffeine: Should You Quit Coffee Too?
- Cannabinoid Hyperemesis Syndrome (CHS)
Emotional and Mental Symptoms
- Anger and Irritability During Weed Withdrawal
- Weed Withdrawal Irritability: Why Everything Makes You Angry
- Weed Withdrawal and Anger: Why You're Raging
- Weed Withdrawal Brain Fog: When You Can't Think Straight
- Weed Withdrawal Depression: Why You Feel Empty
- Weed Withdrawal Mood Swings: The Emotional Rollercoaster
- Weed Withdrawal and Crying: Why You Can't Stop
- Emotional Flooding After Quitting Weed
- Weed and Depersonalization: When Reality Feels Unreal
Timeline and Milestones
- Weed Withdrawal Timeline: Day by Day Breakdown
- How Long Does Weed Withdrawal Last? Honest Answer
- What Happens When You Stop Smoking Weed: Week by Week Changes
- How Long to Feel Normal After Quitting Weed: A Realistic Timeline
- The First 7 Days Without Weed: A Day-by-Day Survival Guide
- Cannabis Withdrawal Syndrome Timeline: Day-by-Day Symptom Map
- PAWS: Post-Acute Withdrawal from Cannabis
- Weed PAWS Withdrawal: Why Recovery Takes Months
Demographics
Comparisons
- Cannabis Withdrawal vs Nicotine, Alcohol, and Opioid Withdrawal
- Weed Withdrawal vs Alcohol Withdrawal: How They Compare
The Bottom Line
Cannabis withdrawal is a clinically recognized condition that affects roughly 47% of frequent users. Symptoms typically begin within 24 hours, peak between days 3 and 6, and resolve within 2 to 4 weeks — though sleep disturbances can persist up to 45 days. Withdrawal is uncomfortable but never medically dangerous, and understanding the timeline makes it predictable and manageable.
Sources & References
- 1RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩
- 2RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩
- 3RTHC-00134·Budney, Alan J. et al. (2003). “When Heavy Users Quit Cannabis, Symptoms Show Up Fast and Ease Within Two Weeks.” Journal of Abnormal Psychology.Study breakdown →PubMed →↩
- 4RTHC-00159·Budney, Alan J. et al. (2004). “Yes, Cannabis Withdrawal Is Real. This 2004 Review Mapped What It Looks Like..” American Journal of Psychiatry.Study breakdown →PubMed →↩
- 5RTHC-00301·Bolla, Karen I. et al. (2008). “Stopping Heavy Cannabis Use Was Linked to Poorer Sleep. The Second Night Looked Worse..” Sleep.Study breakdown →PubMed →↩
- 6RTHC-00467·Allsop, David J et al. (2011). “New Cannabis Withdrawal Scale developed: nightmares were most diagnostic, angry outbursts caused the most distress.” Drug and alcohol dependence.Study breakdown →PubMed →↩
- 8RTHC-02471·Claus, Benedikt Bernd et al. (2020). “Urine THC metabolite levels moderately predicted cannabis withdrawal severity during detox.” Frontiers in psychiatry.Study breakdown →PubMed →↩
- 9RTHC-00538·Allsop, David J. et al. (2012). “Withdrawal That Disrupted Daily Life Was Tied to Relapse in a Small Study.” PLOS ONE.Study breakdown →PubMed →↩
- 10RTHC-00608·Raichlen, David A. et al. (2012). “Runner's High Has an Endocannabinoid Signature in Humans. Dogs Show It Too..” Journal of Experimental Biology.Study breakdown →PubMed →↩
- 11RTHC-06584·Gray, Kevin M et al. (2025). “N-Acetylcysteine Did Not Help Youth Quit Cannabis Without Contingency Management.” Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology.Study breakdown →PubMed →↩
- 12RTHC-01513·Schlienz, Nicolas J et al. (2017). “Cannabis Withdrawal Is Real, Driven by CB1 Receptor Changes, and May Be Worse for Women.” Current addiction reports.Study breakdown →PubMed →↩
- 13RTHC-06809·Keen, Larry et al. (2025). “Heart Rate Variability Drops Immediately After Cannabis Smoking in Young Adults with CUD.” International journal of psychophysiology : official journal of the International Organization of Psychophysiology.Study breakdown →PubMed →↩
- 14RTHC-01334·Bhattacharyya, Sagnik et al. (2017). “THC-induced anxiety in humans is linked to CB1 receptor density in the amygdala.” Scientific reports.Study breakdown →PubMed →↩
- 15RTHC-01161·Gates, Peter et al. (2016). “Systematic Review Confirms Cannabis Withdrawal Disrupts Sleep, but Specific Mechanisms Remain Unclear.” Substance abuse.Study breakdown →PubMed →↩
- 16RTHC-01338·Bonnet, Udo et al. (2017). “Comprehensive review of cannabis withdrawal: symptoms, brain mechanisms, gender differences, and treatment options.” Substance abuse and rehabilitation.Study breakdown →PubMed →↩
- 17RTHC-02524·Eckard, M L et al. (2020). “THC withdrawal reduced motivation for sucrose in mice, modeling the anhedonia of cannabis cessation.” Pharmacology.Study breakdown →PubMed →↩
- 18RTHC-02026·Fabisiak, Adam et al. (2019). “CB1 receptor blockers caused diarrhea so consistently they might actually treat constipation-dominant IBS.” Journal of gastrointestinal and liver diseases : JGLD.Study breakdown →PubMed →↩
What the Research Shows
This section synthesizes 166 peer-reviewed studies on Cannabis Withdrawal Syndrome. Stronger evidence means more consistency across study types.
Cannabis withdrawal affects approximately 47% of regular/dependent users — confirmed by the first meta-analysis pooling 23 studies with 27,461 participants
Strong EvidenceThe symptom profile is consistent and reproducible: irritability, anxiety, sleep disturbance, decreased appetite, restlessness, depressed mood, and physical discomfort emerge within 1-3 days and peak in the first week
Strong EvidenceCB1 receptor recovery begins within 2 days of abstinence and normalizes within approximately 4 weeks, providing a neurobiological basis for the clinical symptom timeline
Strong EvidenceNo medication has demonstrated strong evidence for achieving cannabis abstinence — confirmed by the 2025 Cochrane systematic review searching through May 2024
Strong EvidencePsychotherapy, particularly CBT, is the most effective treatment for cannabis dependence, with evidence-level Ia support (the highest) and effect sizes of 0.53-0.9
Strong EvidenceWhere Scientists Disagree
Areas where research shows conflicting results or ongoing scientific debate.
Cannabinoid agonist replacement (nabiximols, dronabinol, nabilone) reduces withdrawal severity but has not translated to better long-term abstinence outcomes
Moderate EvidenceSleep disruption follows a unique withdrawal trajectory — it worsens over the first 1-2 weeks rather than peaking with other symptoms in the first 3 days
Moderate EvidenceCannabis withdrawal can trigger or worsen psychiatric symptoms, with psychiatric intensive care transfers peaking 3-5 days post-admission in hospitalized cannabis users
Moderate EvidenceWhat We Still Don't Know
- No FDA-approved medication exists for cannabis withdrawal or cannabis use disorder — the most significant unmet clinical need in this field.
- Long-term prospective studies tracking withdrawal severity, duration, and predictors across diverse populations are scarce.
- The interaction between withdrawal and co-occurring mental health conditions (anxiety disorders, depression, PTSD) is poorly characterized — most withdrawal studies exclude participants with significant psychiatric comorbidities.
- How withdrawal severity varies by product type (flower vs. concentrates vs. edibles) and potency has not been systematically studied, despite the dramatic increase in THC concentrations over the past two decades.
- Digital therapeutics and app-based interventions for managing withdrawal have shown early promise but lack rigorous RCT evidence.
Evidence Breakdown
Distribution of study types in this research area. Higher-tier evidence (meta-analyses, RCTs) provides stronger conclusions.
Research Timeline
How our understanding of this topic has evolved.
Before 2004
Cannabis withdrawal was controversial. Early case reports and small studies documented symptoms, but many clinicians and researchers questioned whether a true withdrawal syndrome existed. Budney's 2003 time-course study was among the first to rigorously map symptom trajectories.
2004-2012
Evidence accumulated through controlled laboratory studies and clinical observation. Budney's 2004 review proposed diagnostic criteria. The Cannabis Withdrawal Scale was validated (2011). The body of evidence grew strong enough to inform diagnostic classification.
2013
Cannabis Withdrawal Syndrome was added to the DSM-5, marking official recognition. This catalyzed a wave of research into prevalence, mechanisms, and treatment.
2014-2019
The most productive research period. Multiple RCTs tested pharmacotherapies (nabiximols, dronabinol, nabilone, gabapentin). Neuroimaging studies revealed CB1 receptor recovery dynamics. Gender differences were documented. The symptom profile was refined.
2020-present
Meta-analyses quantified withdrawal prevalence at 47%. The 2025 Cochrane Review confirmed no approved pharmacotherapy. Research shifted toward understanding withdrawal in the context of rising THC potency, higher-risk products (concentrates), and psychiatric comorbidities. Digital therapeutics emerged as a new frontier.