The Endocannabinoid System Explained Simply: What It Does and Why It Matters
Balanced Cannabis Science
1992
Your body's own cannabis system was discovered in 1992 when researchers found anandamide, the natural chemical THC mimics to hijack mood, sleep, appetite, and pain regulation.
Devane et al., Science, 1992
Devane et al., Science, 1992
View as imageIf you only read one thing
Your body has its own built-in cannabis system — it makes chemicals that work just like THC to control your mood, sleep, appetite, and pain. Scientists only found it in 1992. When you use cannabis regularly, your brain turns this system down to compensate. When you stop, the system needs about 4 weeks to come back online. That recovery period is what withdrawal actually is.
You keep seeing the phrase "endocannabinoid system" in articles about cannabis, withdrawal, and health. It sounds technical. It sounds like something you need a biology degree to understand. You do not. The endocannabinoid system is one of the most important systems in your body, and it can be explained in plain language without losing any of the science that makes it matter.
This is that explanation.
Key Takeaways
- Your body has a built-in system called the endocannabinoid system (ECS) that controls mood, sleep, appetite, pain, memory, and immune function — and scientists only discovered it in the 1990s
- It runs on two receptors (CB1 in the brain, CB2 in the immune system), two chemicals your body makes (anandamide and 2-AG), and two enzymes that break them down (FAAH and MAGL)
- The ECS works through retrograde signaling — your receiving neurons send messages backward to tell sending neurons "that is enough" — making it a built-in feedback system that THC overrides
- THC works because it copies anandamide and activates CB1 receptors — but far more intensely and for much longer than your body's own chemicals ever would
- Some people may have naturally lower endocannabinoid tone, which could explain why they were drawn to cannabis and why quitting feels harder
- CBD interacts with the ECS differently than THC and does not produce the same high or the same pattern of dependence
- The ECS is larger than originally understood — researchers have identified an expanded "endocannabinoidome" with additional receptors and signaling molecules
- Understanding the ECS is the key to understanding tolerance, withdrawal, and recovery, because all three are direct results of how this system adapts to THC
- Exercise, social connection, omega-3 fatty acids, and stress management all directly support ECS function and recovery
Your Body Built This System First
The word "endocannabinoid" sounds like it comes from cannabis. It does, but only because of the order scientists discovered things. Researchers figured out THC before they figured out why THC works. When they finally identified the biological system THC was targeting, they named it after the plant that led them there. The "endo" prefix means "within," so endocannabinoid literally means "cannabinoid from inside your body."
Here is how the signaling pathway works, from chemical production to receptor activation to cleanup.
Endocannabinoid System
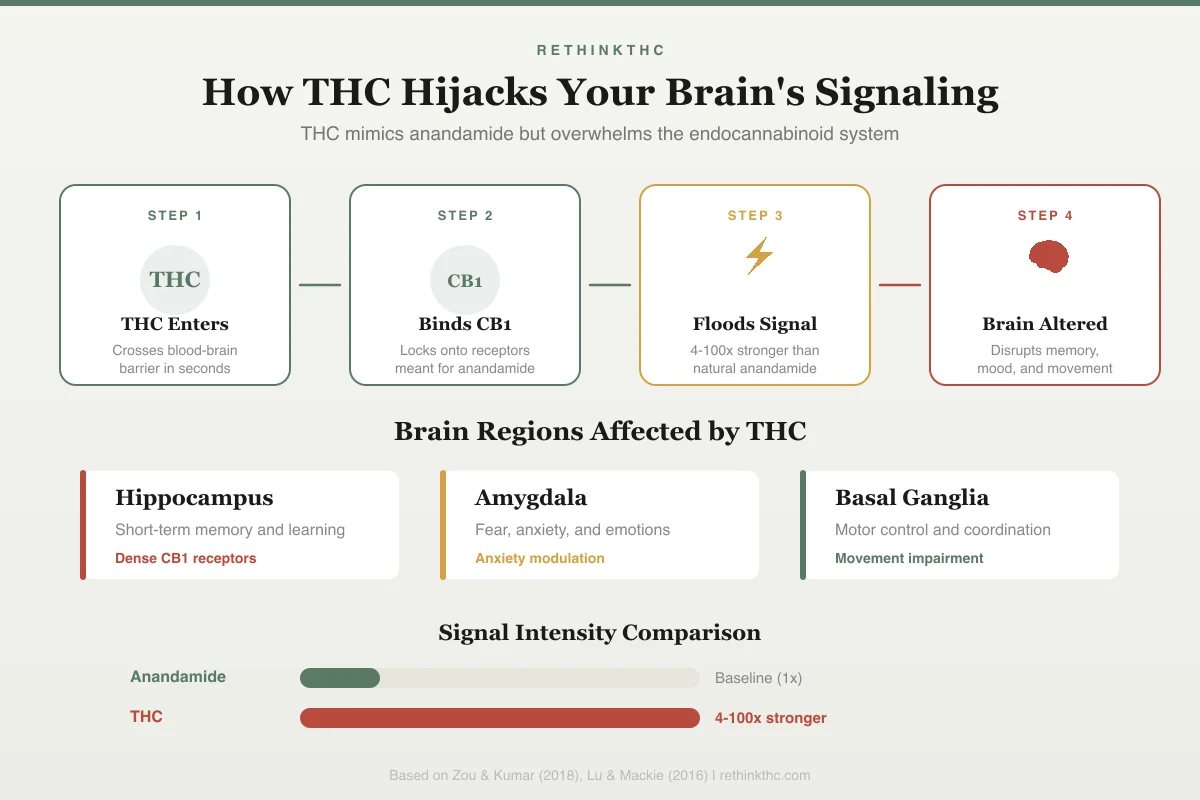
How THC Hijacks Your Brain's Signaling
Step 1
THC Enters
Crosses blood-brain barrier in seconds
Step 2
Binds CB1
Locks onto receptors meant for anandamide
Step 3
Floods Signal
4-100x stronger than natural anandamide
Step 4
Brain Altered
Disrupts memory, mood, and movement
Brain Regions Affected
Hippocampus
Short-term memory and learning
Dense CB1 receptors
Amygdala
Fear, anxiety, and emotions
Anxiety modulation
Basal Ganglia
Motor control and coordination
Movement impairment
Signal Intensity Comparison
The important point is this: cannabis did not invent this system. Your body has been running it for as long as humans have existed. Every mammal has one.[2] It was operating long before anyone ever encountered a cannabis plant.
The Discovery That Changed Everything
In 1992, a team led by Raphael Mechoulam at Hebrew University in Jerusalem made a finding that reshaped neuroscience. They discovered that the human body produces its own cannabis-like chemical. They named it anandamide, from the Sanskrit word "ananda," meaning bliss. The discovery, published in the journal Science,[1] proved that THC does not create a new experience in your brain. It plugs into a system that was already running.
A few years later, researchers identified a second natural cannabinoid called 2-arachidonoylglycerol, or 2-AG for short.[6] While anandamide gets more attention because of its name and history, 2-AG is actually more abundant in the brain and plays a broader role in day-to-day signaling.
These two chemicals, anandamide and 2-AG, are your endocannabinoids. They are the messages your body sends through this system.
The Hardware: CB1 and CB2 Receptors
Messages need somewhere to land. That is what cannabinoid receptors are. Think of them as locks on the surface of your cells. When the right chemical (the key) arrives and binds to the receptor (the lock), the cell responds. There are two main types of cannabinoid receptors, and they sit in very different locations.
CB1 receptors are concentrated in your brain and central nervous system. They are some of the most abundant receptors in the entire human brain[2], found in regions that control mood, memory, appetite, pain perception, movement, and sleep. When anandamide or 2-AG binds to a CB1 receptor, it modulates the activity of that brain region, turning signals up or down to keep things balanced.
CB2 receptors are found primarily in your immune system, gut, and peripheral tissues.[2] They regulate inflammation, immune responses, and digestive function. CB2 receptors do not play a major role in producing the "high" from THC, but they matter for overall health and for the physical symptoms some people experience during withdrawal (gut disruption, inflammation, body aches). CB1's role in movement and motor coordination is especially relevant for understanding impairment.
The table below maps every component of the system, where it lives, and what it does.
| ECS Component | What It Is | Where It Is | What It Does |
|---|---|---|---|
| CB1 receptors | Cannabinoid receptor type 1 | Brain, spinal cord, central nervous system | Modulates mood, memory, appetite, pain, sleep, movement |
| CB2 receptors | Cannabinoid receptor type 2 | Immune cells, gut, peripheral tissues | Regulates inflammation, immune responses, digestion |
| Anandamide | Endogenous cannabinoid | Produced on-demand throughout the body | Brief, targeted signaling for mood, pain, and stress regulation |
| 2-AG | Endogenous cannabinoid (most abundant) | Produced on-demand throughout the body | Broader signaling role; more abundant than anandamide |
| FAAH | Enzyme | Cell membranes | Breaks down anandamide within seconds after use |
| MAGL | Enzyme | Cell membranes | Breaks down 2-AG within seconds after use |
A comprehensive 2016 review by Lu and Mackie in Biological Psychiatry[2] documented the ECS as one of the most widespread modulatory systems in the human body. It is not a minor subsystem. It is a master regulatory network that touches nearly every physiological process you can name.
The Cleanup Crew: FAAH and MAGL
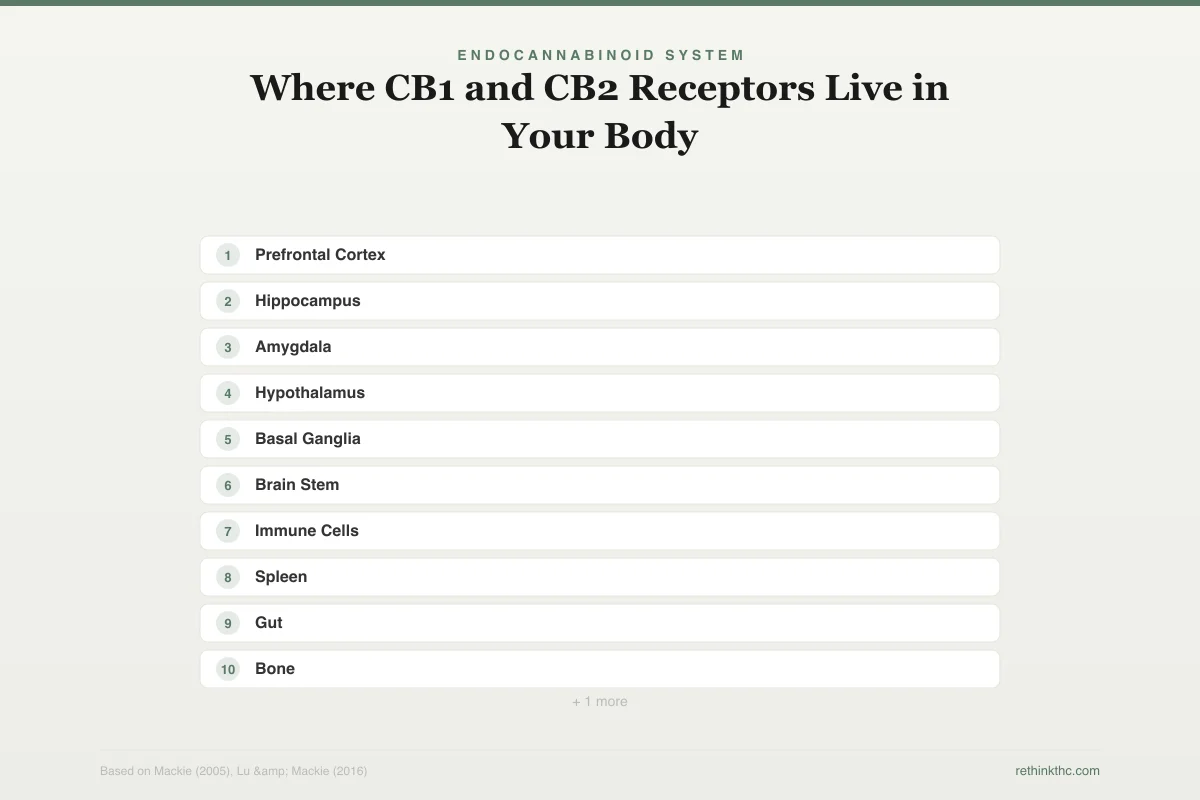
Your endocannabinoids are not meant to stick around. They are built on demand, used immediately, and broken down right after. Two enzymes handle this cleanup. The map below shows where these receptors sit across your brain and body.
Endocannabinoid System
Where CB1 and CB2 Receptors Live in Your Body
Brain & CNS
Neurological effects
Prefrontal Cortex
Decision-making, judgment
Hippocampus
Memory formation
Amygdala
Fear and anxiety
Hypothalamus
Appetite regulation
Basal Ganglia
Movement control
Brain Stem
Nausea, vomiting
Body & Immune
Physical effects
Immune Cells
Inflammation response
Spleen
Immune cell storage
Gut
Digestion, motility
Bone
Bone metabolism
Skin
Barrier function
FAAH (fatty acid amide hydrolase) breaks down anandamide. Once anandamide has delivered its signal and activated a receptor, FAAH degrades it within seconds.[2] This keeps the signaling precise. You get exactly the amount of anandamide activity you need, exactly when you need it, and no more.
MAGL (monoacylglycerol lipase) does the same job for 2-AG. It clears 2-AG from the system after it has done its work.
This on-demand, build-and-destroy cycle is critical to understanding why THC causes problems with chronic use. Your natural system is designed for brief, targeted bursts of cannabinoid activity. THC violates that design.
Why Endocannabinoid Signaling Is Unlike Anything Else in Your Brain
There is one more thing about this system that makes it unusual, and it matters for understanding why THC is so disruptive.
Most neurotransmitters in your brain travel in one direction: from the sending neuron to the receiving neuron. Endocannabinoids do the opposite. They are produced by the receiving neuron and sent backward to the sender.[2] Scientists call this retrograde signaling, and it is the ECS's defining feature.
Think of it as a built-in volume knob. When a receiving neuron is getting too much input — too much excitation, too much inhibition, too much of anything — it manufactures endocannabinoids on the spot and sends them backward to the sender. The message is simple: "That is enough. Dial it back." The sender responds by reducing its output. Balance is restored. The endocannabinoid is immediately broken down by FAAH or MAGL, and the system resets.
This is why the flashlight analogy from the THC section matters. Your endocannabinoids are manufactured at the exact synapse that needs adjustment, travel a few micrometers backward, deliver one precise message, and disappear. THC arrives from outside, floods every CB1 receptor it encounters, and the "that is enough" feedback loop never fires because the signal is not coming from a receiving neuron. It is coming from your bloodstream. The volume knob is broken. The floodlight stays on.
What the ECS Regulates
The reason the ECS matters so much is the sheer range of functions it influences. Scientists describe it as a homeostatic regulator, which is a technical way of saying its primary job is keeping things balanced. When something drifts too far in one direction, the ECS nudges it back.
Mood and emotional regulation. Endocannabinoids modulate the release of serotonin, dopamine, GABA, and other neurotransmitters that determine how you feel.[2] When the ECS is functioning well, it acts as a stress buffer, preventing emotional reactions from spiraling out of proportion. This is the same system that goes haywire during weed and anxiety — when THC artificially dampens the amygdala for months and then disappears, the anxiety regulation overshoots before it stabilizes.
Sleep. The ECS influences your sleep-wake cycle through activity in the hypothalamus and brainstem. Anandamide, in particular, promotes sleep onset and helps maintain sleep stability.
Appetite and digestion. CB1 receptors in the hypothalamus drive hunger signals.[2] CB2 receptors in the gut support digestion and gut motility. This is why cannabis stimulates appetite and why disrupted appetite is one of the most common withdrawal symptoms.
Pain. Endocannabinoids modulate pain signals from the peripheral nerves through the spinal cord to the brain.[2] They do not eliminate pain. They adjust how loudly it registers.
Memory. CB1 receptors in the hippocampus (the brain's memory center) influence how memories are formed and stored. This explains both the short-term memory effects of THC and the cognitive recovery many people notice after quitting. For those wondering specifically about academic performance, the THC and studying article covers the research on learning under the influence.
Immune function. CB2 receptors throughout the immune system regulate inflammation, keeping immune responses effective without letting them cause collateral damage.
Stress response. Hillard's 2018 review in Neuropsychopharmacology[3] documented that circulating endocannabinoid levels are directly responsive to stress. The ECS is part of how your body manages stress at a biochemical level, not just a psychological one.
When the System Runs Low: Clinical Endocannabinoid Deficiency
Not everyone's ECS runs at the same level. Some researchers believe that certain people have naturally lower endocannabinoid tone — fewer endocannabinoids circulating, less responsive receptors, or both — and that this deficit may explain why some conditions cluster together in ways that have puzzled doctors for decades.
The theory is called clinical endocannabinoid deficiency (CECD). A 2016 review by Russo examined the growing evidence and found that three notoriously treatment-resistant conditions — migraine, fibromyalgia, and irritable bowel syndrome — share a pattern that aligns with an underactive ECS.[8] All three involve disruptions to functions the ECS regulates (pain processing, gut motility, sensory sensitivity). All three co-occur more often than chance predicts. And all three have shown some response to cannabinoid-based treatments.
Here is where this connects to your experience. If your ECS was running low before you started using cannabis, you may have been drawn to cannabis precisely because it compensated for a deficit your body was not filling on its own. The relief was real. It was not weakness or a lack of willpower. Your biology was driving the behavior because THC was doing something your system genuinely needed done.
The problem is that external THC does not fix the deficit. It masks it while creating new adaptations — tolerance, receptor downregulation, reduced natural production — that make the underlying situation worse. When you quit, the gap between where your ECS is and where it needs to be is wider than it would be for someone whose baseline tone was normal to begin with. This may explain why withdrawal hits some people much harder than others, and why targeted recovery support (exercise, nutrition, stress management) matters more for some people than "just wait it out."
CECD is still a theory, not a confirmed clinical diagnosis. There is no blood test or brain scan for endocannabinoid tone. But it has real explanatory power for people who found cannabis relief so profound that quitting felt biologically impossible. Understanding that your biology may have been part of the equation changes the story from "I am too weak to quit" to "my system needed support that THC was the wrong long-term answer for."
How THC Hijacks the System
THC (tetrahydrocannabinol) is the primary psychoactive compound in cannabis. It works because its molecular shape is similar enough to anandamide that it fits into CB1 receptors.[2] But the resemblance is only structural. The behavior is very different.
Your endocannabinoids are precise. They are manufactured at the exact location where they are needed, activate receptors briefly, and get broken down within seconds by FAAH or MAGL. They are like a carefully aimed flashlight, illuminating one spot at just the right intensity.
THC is more like a floodlight. When you consume cannabis, THC spreads throughout your brain and activates CB1 receptors broadly, not just at specific locations. It binds more strongly than anandamide. And critically, your enzymes (FAAH and MAGL) are not equipped to break down THC the way they break down your natural endocannabinoids.[2] So THC lingers for hours, producing sustained, elevated activation across the entire CB1 receptor network. When that sustained activation becomes constant through all-day use, the consequences compound, as detailed in what happens when you are high 24/7.
This is the high. It is your ECS being pushed far beyond its normal operating range by a chemical that fits the receptors but ignores the built-in controls that keep signaling precise and temporary. For a closer look at what this means for specific brain regions, the articles on THC and the prefrontal cortex and how THC affects the amygdala break down the regional effects in detail. For a comprehensive look at every common cannabis effect and the neuroscience behind it, see cannabis effects and experience: the science behind your high. These same effects on reaction time, coordination, and judgment are why THC measurably affects driving ability.
How CBD Interacts Differently
CBD (cannabidiol) is the other major compound in cannabis, and it does not work the same way THC does. CBD does not bind directly to CB1 receptors the way THC and anandamide do. Instead, it interacts with the ECS indirectly. The comparison below shows exactly how THC's behavior differs from your body's own chemicals at every step.
Endocannabinoid System
Anandamide vs. THC: Your Body's Chemical vs. the Plant's
Anandamide
Your body's own
THC
From cannabis
Type
Partial agonist
Type
Stronger agonist
Duration
Minutes
Duration
Hours
Production
Made on-demand
Production
Floods system externally
Breakdown
Quickly by FAAH
Breakdown
FAAH cannot clear efficiently
Effect on mood
Subtle regulation
Effect on mood
Intense euphoria
Effect on pain
Gentle modulation
Effect on pain
Strong suppression
Effect on appetite
Normal hunger cues
Effect on appetite
Amplified cravings
Long-term impact
Maintains balance
Long-term impact
Receptor downregulation
THC overrides the system anandamide was designed to regulate — leading to tolerance, dependence, and withdrawal
One of CBD's documented effects is inhibiting FAAH, the enzyme that breaks down anandamide.[7] By slowing down anandamide degradation, CBD may allow your natural endocannabinoids to remain active slightly longer. This is a fundamentally different mechanism than THC flooding receptors from outside. CBD nudges the system from within rather than overriding it.
This difference in mechanism explains why CBD does not produce the intoxicating high that THC does, and why CBD does not cause the same pattern of tolerance and withdrawal. For a deeper comparison of how these two compounds affect your body and brain differently, the CBD vs. THC article covers the distinctions in detail.
Why This Matters for Tolerance
When CB1 receptors get activated by THC repeatedly, your brain adapts. It is not malfunctioning. It is doing exactly what it is designed to do: protect itself from overstimulation.
The first adaptation is downregulation. Your brain physically removes CB1 receptors from cell surfaces or makes them less responsive. A 2012 PET imaging study published in Molecular Psychiatry[4] showed that chronic cannabis users have significantly fewer available CB1 receptors compared to non-users. Fewer receptors means a weaker response to the same dose, which is tolerance at a biological level.
The second adaptation is reduced natural endocannabinoid production. When THC is flooding the system from outside, your brain scales back its own manufacturing of anandamide and 2-AG. Why produce internal cannabinoids when there is already an external surplus?
Over time, these adaptations mean you need more THC to feel the same effect. This is not a willpower issue. It is receptor math. The downstream effects on your brain's reward system and motivation pathways are direct consequences of this receptor-level change. For practical guidance on managing this process intentionally, the tolerance break guide walks through how to reset your sensitivity.
Why This Matters for Withdrawal
When you stop using cannabis after a period of regular use, the THC clears out. But your downregulated receptors and reduced endocannabinoid production do not recover instantly. You are left with an ECS that has fewer receptors, less internal cannabinoid supply, and no external THC to fill the gap.
The system that regulates your mood, sleep, appetite, pain, stress response, and digestion is temporarily running below capacity. Every withdrawal symptom maps directly to an ECS function. Insomnia, mood swings, appetite loss, sweating, anxiety, brain fog: none of it is random. It is a specific, predictable consequence of an impaired endocannabinoid system rebuilding itself.
The endocannabinoid system and withdrawal article covers how each symptom connects to specific ECS disruptions in detail.
Why This Matters for Recovery
Here is the part that matters most if you are going through this. The ECS recovers. That same 2012 Molecular Psychiatry study[4] tracked what happened after chronic users stopped. CB1 receptor density began recovering within just two days. By approximately 28 days, receptor availability had returned to levels statistically indistinguishable from people who had never used cannabis.
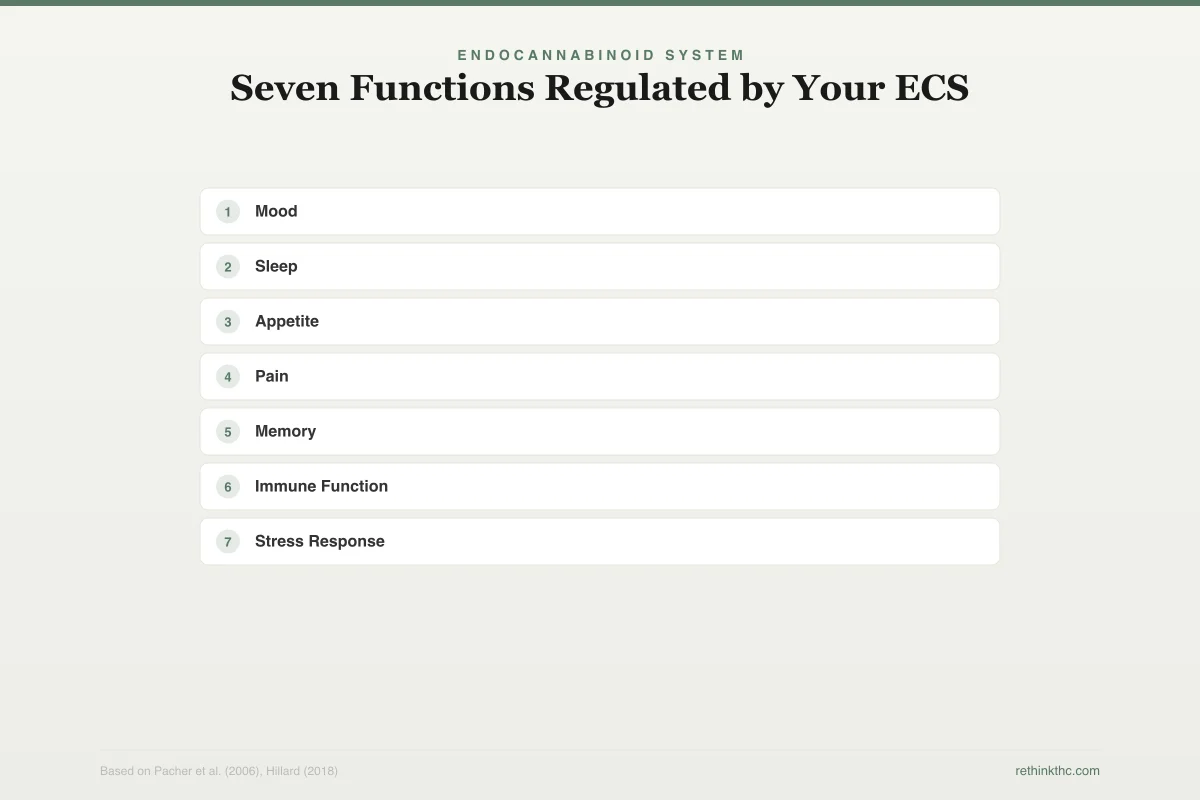
Here is what that recovery looks like mapped across every function the ECS regulates.
Endocannabinoid System
Seven Functions Regulated by Your ECS
Mood
Anandamide
CB1
Sleep
Anandamide
CB1
Appetite
2-AG
CB1
Pain
Anandamide
CB1
Memory
2-AG
CB1
Immune Function
2-AG
CB2
Stress Response
Anandamide
CB1
Natural endocannabinoid production also recovers, though this process is less precisely measured in current research. The general trajectory is clear: the system comes back online. For a detailed look at the receptor recovery timeline and what influences it, see the cannabinoid receptor recovery article. For a step-by-step plan that works with this recovery timeline, see the guide on how to quit weed.
You Can Support Your ECS Naturally
You cannot force the recovery timeline. But you can give your ECS what it needs to rebuild efficiently.
Exercise is the strongest tool available. This is not a generic wellness suggestion. A 2012 study in the Journal of Experimental Biology[5] found that aerobic exercise directly increases circulating endocannabinoid levels. Running and other sustained aerobic activity trigger your body to produce more anandamide. This is what researchers now believe explains the "runner's high," not endorphins, as was previously assumed. When you exercise during withdrawal or recovery, you are literally supplying your ECS with the natural chemicals it is missing.
A 2025 pilot study added specifics: 30 minutes of moderate-intensity aerobic exercise (64 to 76 percent of maximum heart rate) significantly increased anandamide and several other endocannabinoid-like molecules.[10] You do not need to run a marathon. A brisk walk, a steady jog, a bike ride where you are breathing hard but can still talk — 30 minutes at that intensity appears to be the threshold where your body starts producing meaningful endocannabinoid output.
Social connection is an endocannabinoid input. This one surprises people, but the biology is real. Animal research suggests that anandamide mediates some of the social bonding effects of oxytocin, the hormone released during trust, touch, and connection.[11] In those models, boosting anandamide completely reversed social impairment, and the effect ran specifically through CB1 receptors. The research is preclinical, but the implication is significant: your endocannabinoid system and your social bonding system are wired together.
During withdrawal, when your ECS is depleted and social interaction feels harder than usual, this matters. Isolating yourself removes one of the inputs your system needs to rebuild. You do not need to be social in a big way. A phone call, a meal with one person, a walk with a friend — these are endocannabinoid inputs.
Omega-3 fatty acids provide raw materials. Your body builds endocannabinoids from fatty acid precursors. Foods rich in omega-3s (fatty fish, walnuts, flaxseed, chia seeds) give your body the building blocks it needs to manufacture anandamide and 2-AG.
Stress management matters. Chronic stress depletes endocannabinoid tone.[3] The relationship between cannabis, cortisol, and your stress hormones is complex, and during recovery your stress buffer is already weakened. Adding unmanaged stress compounds the deficit. Deep breathing, time outdoors, and mindfulness practices all support healthy ECS function.
Sleep supports recovery, and recovery supports sleep. The relationship is bidirectional. Maintaining consistent sleep and wake times, even during the difficult first two weeks, gives your ECS the best environment to recalibrate.
Some preliminary evidence suggests brief cold exposure may influence endocannabinoid signaling, though the cannabis-specific research is still too early to make definitive recommendations. Chocolate contains anandamide and anandamide-like compounds in small amounts — enjoyable, but not pharmacologically significant. The most reliable tools remain exercise, social connection, omega-3 fatty acids, stress management, and time.
Common Misconceptions
"Cannabis created this system." No. The ECS exists in all mammals and predates any human contact with cannabis by millions of years. Cannabis simply contains chemicals that interact with it. This distinction is especially important when considering cannabis and the developing brain, where the ECS plays a critical role in normal neurodevelopment.
"The ECS only matters if you use cannabis." Not at all. The ECS regulates fundamental functions for everyone, regardless of whether they have ever used cannabis. It matters for understanding stress, sleep, pain, mood, and immune health in any context.
"If my body makes its own cannabinoids, I need cannabis to supplement them." Your body makes endocannabinoids on its own, in the right amounts, at the right times, without any external input. External THC does not supplement the system. It overrides it.
"CBD is basically the same as THC." They interact with the ECS through completely different mechanisms. THC directly activates CB1 receptors. CBD works indirectly, primarily by influencing enzyme activity. The effects, risks, and dependency potential are meaningfully different.
What Scientists Are Still Discovering
The endocannabinoid system described in this article is the simplified version. The full picture is still emerging, and it is bigger than anyone initially expected.
Researchers now use the term endocannabinoidome to describe an expanded network that goes well beyond CB1, CB2, anandamide, and 2-AG. A 2020 review in Nature Reviews Neurology mapped this broader system[9], which includes additional receptors (GPR55, TRPV1, PPARs), dozens of endocannabinoid-like lipid molecules that your body produces alongside anandamide and 2-AG, and connections to the gut microbiome that influence mood, inflammation, and immune function through pathways scientists are only beginning to map.
The gut-brain connection is particularly relevant. CB2 receptors in your gut interact with gut bacteria in ways that influence how you feel emotionally and physically. This is part of why gastrointestinal symptoms during withdrawal (nausea, cramping, disrupted digestion) are not just side effects. They are the ECS recalibrating in your gut at the same time it is recalibrating in your brain.
Why does this matter for you right now? Two reasons. First, it explains why cannabis affects so many different things. It is not that THC is a uniquely powerful drug. It is that the system THC plugs into is extraordinarily far-reaching. Second, it means the current approach to cannabis (flooding CB1 receptors with THC) is like using a sledgehammer on a system designed for scalpels. As researchers understand the full endocannabinoidome, treatments will get more precise — targeting specific parts of the expanded system rather than brute-forcing the whole thing.
That is not a reason to wait for better science before addressing your cannabis use. It is context for why the current approach (stopping, letting the system recover, supporting recovery naturally) remains the best available strategy while the research catches up.
When to Seek Professional Help
Understanding the ECS is valuable, but knowledge alone does not replace professional support when it is needed. If you are experiencing withdrawal symptoms that significantly interfere with your ability to function, a healthcare provider can help manage specific symptoms during the transition. If you have been using cannabis to manage a condition like chronic pain, anxiety, PTSD, or insomnia, a clinician can help you develop alternative strategies that work with your ECS rather than overriding it.
If you are experiencing thoughts of self-harm at any point, reach out immediately.
SAMHSA's National Helpline is free, confidential, and available 24 hours a day, 7 days a week: 1-800-662-4357.
The Simple Version
Your body has a signaling system called the endocannabinoid system. It uses chemicals you naturally produce (anandamide and 2-AG) to regulate mood, sleep, appetite, pain, memory, stress, and immune function through two types of receptors (CB1 and CB2). It works by sending signals backward across synapses — a feedback loop that tells your brain "that is enough." THC works because it mimics those natural chemicals, but louder and longer — and because it comes from outside, it bypasses the feedback that keeps the system in check. Chronic THC use causes your brain to turn down its own system. Stopping THC leaves the system temporarily impaired. The system recovers, typically within about four weeks. Exercise, social connection, nutrition, stress management, and time support that recovery. That is the endocannabinoid system, explained simply.
The Bottom Line
The endocannabinoid system (ECS) is a biological signaling network that regulates mood, sleep, appetite, pain, memory, and immune function using chemicals your body naturally produces (anandamide and 2-AG), two receptor types (CB1 in the brain, CB2 in the immune system), and enzymes that break them down (FAAH and MAGL). THC works because it mimics anandamide but activates CB1 receptors more intensely and for much longer. Chronic THC use causes the brain to reduce CB1 receptor availability and scale back natural endocannabinoid production, producing tolerance. When THC is removed, the impaired system produces withdrawal symptoms across every function it regulates. Brain imaging shows CB1 receptors begin recovering within 2 days and return to normal by approximately day 28. Exercise, social connection, omega-3 fatty acids, stress management, and consistent sleep support this recovery.
Sources & References
- 1RTHC-00046·Devane, William A. et al. (1992). “The Discovery of Anandamide — Your Brain's Own Cannabis Molecule.” Science.Study breakdown →PubMed →↩
- 2RTHC-01218·Lu, Hui-Chen et al. (2016). “Your Brain Already Makes Its Own Cannabinoids. Here's How the System Works..” Biological Psychiatry.Study breakdown →PubMed →↩
- 3RTHC-01691·Hillard, Cecilia J. (2018). “Your Blood Carries Endocannabinoids That Track Exercise, Stress, Sleep, and Inflammation.” Neuropsychopharmacology.Study breakdown →PubMed →↩
- 4RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩
- 5RTHC-00608·Raichlen, David A. et al. (2012). “Runner's High Has an Endocannabinoid Signature in Humans. Dogs Show It Too..” Journal of Experimental Biology.Study breakdown →PubMed →↩
- 6RTHC-00072·Mechoulam, R et al. (1998). “The Discovery of the Body's Own Cannabis-Like Molecules: Anandamide and 2-AG.” European journal of pharmacology.Study breakdown →PubMed →↩
- 7RTHC-00924·Blessing, Esther M. et al. (2015). “CBD and Anxiety in 2015: Promising Signals, Mostly From Single Doses.” Neurotherapeutics.Study breakdown →PubMed →↩
- 8RTHC-01255·Russo, Ethan B (2016). “Twelve Years of Evidence: Clinical Endocannabinoid Deficiency Gains Objective Support.” Cannabis and cannabinoid research.Study breakdown →PubMed →↩
- 9RTHC-02484·Cristino, Luigia et al. (2020). “Major review maps the expanded endocannabinoid system and its therapeutic potential across neurological diseases.” Nature reviews. Neurology.Study breakdown →PubMed →↩
- 10RTHC-06191·Cheema, Birinder S et al. (2025). “Cancer Patients Have Lower Endocannabinoid Levels — and Exercise Boosts Them in Both Cancer Patients and Healthy Adults.” Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer.Study breakdown →PubMed →↩
- 11RTHC-01298·Wei, Don et al. (2016). “Boosting the Endocannabinoid Anandamide Completely Reversed Social Impairment in Two Autism Mouse Models.” Cannabis and cannabinoid research.Study breakdown →PubMed →↩