How Weed Rewires Your Reward System (And How to Reset It)
Dopamine / Brain
12 Weeks
THC hijacks the mesolimbic reward pathway, causing measurable changes in the nucleus accumbens and VTA, but neuroplasticity allows most recovery within 4 to 12 weeks of abstinence.
Molecular Psychiatry, 2012
Molecular Psychiatry, 2012
View as imageIf you only read one thing
Weed turns up your brain's pleasure signals way past normal levels. Over time, your brain compensates by turning its own volume down — so without weed, everything feels flat and boring. The good news: this is temporary. Your brain's reward wiring bounces back within about 4 to 12 weeks after you stop, and exercise, new experiences, and social connection speed up the process.
Something shifted and you cannot quite name it. The things that used to light you up, a good meal, your favorite music, an evening with friends, now feel like watching life through a window. You know you are supposed to enjoy them. You remember enjoying them. But the feeling is gone. If you have been using cannabis regularly and this sounds familiar, what you are experiencing is the direct result of how THC interacts with the weed reward system in your brain. Not just dopamine in the abstract, but a specific set of structures and pathways that govern how you experience pleasure, motivation, and meaning.
This article goes deeper than the general dopamine recovery timeline. This is about the reward circuit itself: what it is, how THC takes it over, and what it takes to get it back.
Key Takeaways
- THC hijacks your brain's core reward circuit — the mesolimbic pathway — by mimicking the natural endocannabinoids that regulate pleasure and motivation
- Heavy cannabis use causes measurable changes in the nucleus accumbens and ventral tegmental area (VTA), which are the two structures that drive your sense of reward
- That "nothing feels good anymore" feeling is called anhedonia — it is a direct and temporary result of your reward circuit dialing down after heavy use
- Your reward system can and does rebuild itself after you stop using, because neuroplasticity allows most recovery to happen within four to 12 weeks
- Aerobic exercise, structured novelty, and social engagement directly support reward circuit recovery because they activate the same pathways THC suppressed
- Digital dopamine sources like social media, gaming, and online shopping hit the same mesolimbic pathway — so using them as substitutes during recovery can slow your brain's recalibration
Your Brain's Reward Circuit: The Mesolimbic Pathway
Before you can understand what THC does to your reward system, you need to understand the system itself. Your brain has a dedicated circuit for processing reward. It is called the mesolimbic pathway, and it connects two key structures.
Dopamine
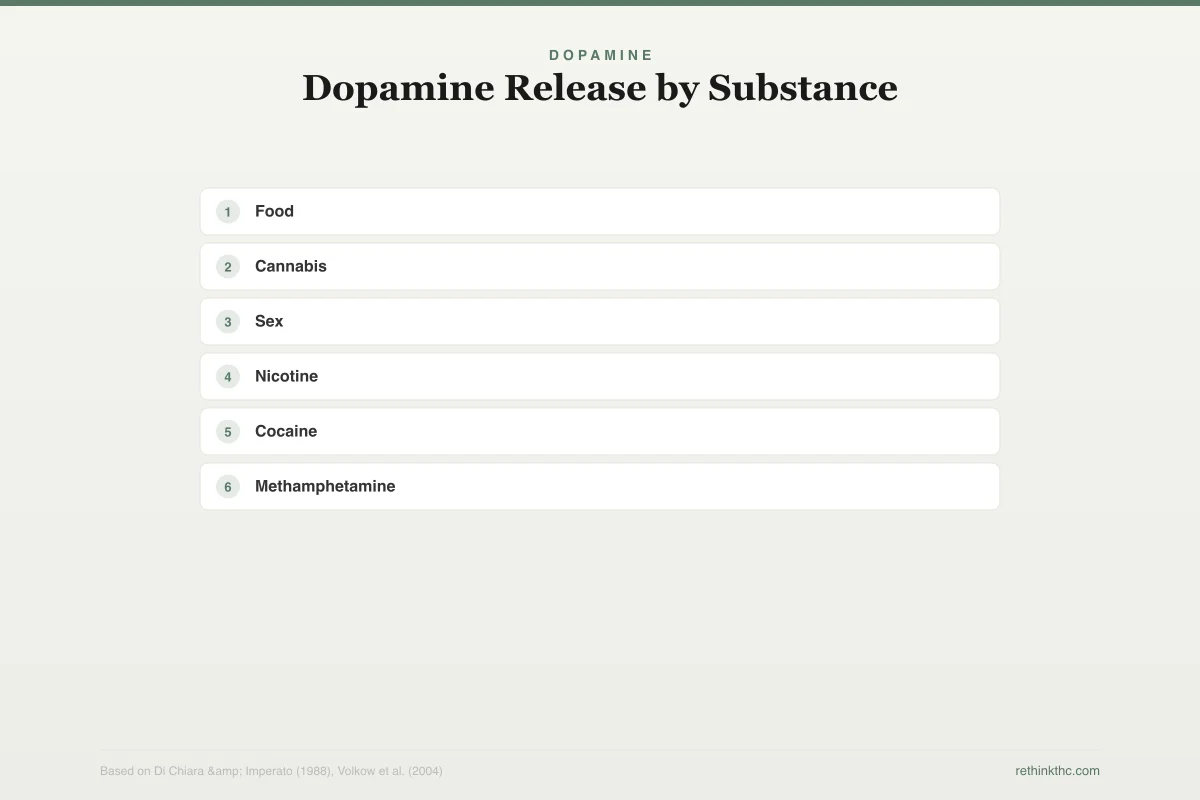
Dopamine Release by Substance
Percentage increase above baseline (100%) in nucleus accumbens dopamine
Cannabis produces a modest dopamine surge comparable to natural rewards — far less than stimulants, but enough to drive habitual use
The first is the ventral tegmental area (VTA), a small cluster of neurons deep in the midbrain. Think of the VTA as the source. It produces dopamine and sends it forward along a bundle of nerve fibers to the second structure.
That second structure is the nucleus accumbens, located in the lower part of the forebrain. The nucleus accumbens is your brain's reward hub. It receives the dopamine signal from the VTA and translates it into the subjective experience of pleasure, satisfaction, and "that was worth doing, do it again." Every naturally rewarding experience you have ever had, food, sex, connection, achievement, laughter, was processed through this circuit.
The mesolimbic pathway does not just register pleasure after the fact. It also generates anticipation. When your brain predicts that something rewarding is about to happen, the VTA fires dopamine into the nucleus accumbens before the reward arrives. This anticipatory signal is what you experience as motivation, excitement, and wanting. It is the reason you feel drawn toward activities that have rewarded you in the past.
A healthy reward system is finely calibrated. Natural rewards produce moderate, proportional dopamine signals. Eating a good meal produces a modest spike. Finishing a meaningful project produces another. The system stays in balance because no natural reward overwhelms it.
How THC Hijacks the Circuit
THC enters this system through a back door. Your brain already has its own version of THC, a class of molecules called endocannabinoids (the most studied being anandamide and 2-AG), which are part of the endocannabinoid system. These endocannabinoids naturally regulate the mesolimbic pathway by fine-tuning how much dopamine the VTA releases. They act as a volume knob, keeping reward signals proportional to actual experiences.
THC mimics these endocannabinoids. It binds to the same CB1 receptors that anandamide targets, but it does so with greater intensity and duration than your brain's own molecules. When THC activates CB1 receptors in the VTA, it removes the braking mechanism on dopamine neurons. A 2004 study by Melis and colleagues, published in the Journal of Neuroscience, demonstrated that THC increases dopamine neuron firing rates in the VTA by suppressing inhibitory signals. In plain terms, THC takes the foot off the brake and the dopamine neurons fire harder and more frequently than they normally would.
The result is a surge of dopamine into the nucleus accumbens that exceeds what any natural reward would produce. Bossong and colleagues confirmed this in humans using PET imaging, publishing their findings in 2009 in NeuroImage. THC administration increased dopamine release in the striatum (the broader region containing the nucleus accumbens) in a measurable, repeatable way.
This is not a catastrophic flood of the kind produced by cocaine or methamphetamine. It is more like turning the volume from five to eight. But when you turn the volume to eight multiple times a day, every day, for months or years, your brain's response is predictable and well-documented.
What Chronic Use Does to the Reward System
Your brain is built to maintain equilibrium. When any signal is artificially elevated for long enough, the system compensates by turning itself down. This adaptation happens at multiple levels within the mesolimbic pathway.
The VTA produces less dopamine. A 2016 study published in Molecular Psychiatry used PET imaging to show that chronic cannabis users have reduced dopamine synthesis capacity in the striatum. Your brain's dopamine factory is literally producing less product.
The nucleus accumbens becomes less sensitive. Repeated overstimulation leads to a reduction in dopamine D2 receptors on the receiving end. Fewer receptors means the nucleus accumbens needs a stronger signal to register the same level of reward. This is what tolerance feels like from the inside: the same amount of cannabis produces less effect, so you use more.
CB1 receptors downregulate. The same receptors that THC uses to hijack the system start disappearing. Hirvonen and colleagues demonstrated this directly in a landmark 2012 study in Molecular Psychiatry,[1] showing measurably reduced CB1 receptor density across the brains of chronic daily users. Your brain is pulling the receptors offline because they are being overstimulated.
Neuroscience
How Chronic Use Downregulates the Reward Circuit
Three levels of adaptation in the mesolimbic pathway
Produces less dopamine
PET imaging shows blunted dopamine synthesis in chronic users
Fewer receptors to catch the signal
Chronic overstimulation leads to receptor reduction
Receptors taken offline
Cortical CB1 density significantly reduced in daily users
Hirvonen et al. (2012), Molecular Psychiatry; Bloomfield et al. (2016), Molecular Psychiatry
View as image
The combined effect is a reward system that has been fundamentally recalibrated around the presence of THC. With THC, it functions. Without THC, it is operating below its natural baseline on every level: less dopamine being produced, fewer receptors to catch it, and a nucleus accumbens that has raised its threshold for what counts as rewarding.
Anhedonia: When Nothing Feels Worth Doing
This recalibrated state has a clinical name: anhedonia. It comes from the Greek for "without pleasure," and it describes exactly what heavy cannabis users experience when they stop, or even between sessions. The things that used to generate enough dopamine to register as rewarding, a conversation, a workout, a sunset, now fall below the threshold your nucleus accumbens has set. The signal arrives, but it is too quiet for the turned-down system to hear.
Anhedonia from reward system downregulation is one of the most common reasons people struggle after quitting cannabis. It overlaps with but is distinct from depression. Many people describe it as feeling "flat" or "gray" rather than sad. If this resonates, the article on not being able to enjoy anything without weed covers the lived experience in detail. The article on boredom after quitting weed addresses a closely related phenomenon, the feeling that nothing is fun or interesting enough to hold your attention.
Anhedonia is also a major driver of relapse. Your brain knows exactly one reliable way to restore the reward signal: the substance that caused the problem. The craving is not weakness. It is a depleted reward circuit identifying the fastest available fix. Understanding the mechanism does not make the craving disappear, but it does reframe it as a neurochemical event rather than a personal failure.
Neuroplasticity: Your Brain Can Rebuild
The most important fact about all of these changes is that they reverse. Your brain is not a fixed machine. It is a living system with neuroplasticity, the ability to reorganize, rebuild, and recalibrate its own wiring in response to changed conditions.
When THC is removed from the equation, every level of the reward system begins recovering. CB1 receptor density starts normalizing within days. The Hirvonen 2012 study found that CB1 receptors showed significant recovery by day 28 of abstinence. Dopamine synthesis capacity and D2 receptor availability follow a parallel but slightly longer trajectory, with most users reporting meaningful improvement between weeks four and eight, and full normalization by week 12.
This is not theoretical. It is directly observable on brain imaging. The changes THC produces in the mesolimbic pathway are real, measurable, and temporary.
Recovery
Reward System Recovery Timeline
When each system bounces back after quitting
Begin recovering within days, significant recovery by day 28
Meaningful improvement weeks 4–8
Full normalization by week 12
Key insight: CB1 receptors recover fastest (days to weeks), while full dopamine signaling normalization can take up to 12 weeks — which is why early withdrawal feels so flat.

The dopamine recovery timeline lays out the week-by-week progression. The general cannabis withdrawal guide covers the full picture of what to expect during the adjustment period.
Practical Strategies to Reset Your Reward System
Neuroplasticity means your brain will rebuild on its own with time. But you can actively support and accelerate that process by engaging the mesolimbic pathway through its natural inputs.
Aerobic exercise directly increases dopamine receptor availability. This is the single most evidence-supported intervention for reward system recovery. Research published in Synapse has shown that regular aerobic exercise upregulates D2 receptors in the striatum, directly reversing one of the key changes produced by chronic cannabis use. You do not need to run marathons. Twenty to thirty minutes of movement that raises your heart rate, walking briskly, cycling, swimming, is enough to trigger the neurochemical cascade. The hardest part is starting, because a depleted reward system generates very little motivation to exercise. Push through the first two weeks and it starts reinforcing itself.
Introduce structured novelty. The VTA responds powerfully to new and unexpected experiences. A different walking route, an unfamiliar genre of music, a conversation with someone outside your usual circle, cooking something you have never attempted. These experiences engage the mesolimbic pathway through different input channels than substance use. Novelty produces dopamine through the brain's salience and curiosity circuits, providing reward system stimulation without reinforcing the old patterns.
Prioritize social connection. Human social interaction is one of the most potent natural activators of the mesolimbic pathway. Oxytocin, released during positive social contact, directly modulates dopamine release in the nucleus accumbens. A 2017 study published in Neuropsychopharmacology demonstrated that social reward and substance reward share overlapping circuitry in the mesolimbic pathway. Rebuilding social engagement is not just emotionally helpful. It is neurochemically restorative.
Use a "reward ladder" approach. Your nucleus accumbens has raised its threshold, so start with small, achievable activities and build up. Do not try to force yourself into activities that require sustained reward engagement (a three-hour hike, an ambitious creative project) during the first week. Start with five-minute walks, one-song listening sessions, brief phone calls. Let each small success generate enough dopamine signal to make the next step feel possible. As your receptors recover, the threshold drops and larger experiences become rewarding again.
Protect sleep aggressively. Dopamine receptor sensitivity is tightly coupled to sleep quality. Research published in the Journal of Neuroscience has shown that sleep deprivation alone reduces D2 receptor availability, compounding the deficit you are already managing. During the early weeks, your sleep is likely disrupted by withdrawal. You cannot fix that entirely, but you can protect it: consistent sleep and wake times, a cool and dark room, no caffeine after noon.
Be cautious with digital dopamine. Social media, video games, online shopping, and other high-frequency digital rewards activate the same mesolimbic pathway you are trying to reset. They are not equivalent to THC, but they can maintain a pattern of frequent, artificial reward stimulation that slows the recalibration process. Awareness is usually sufficient. You do not need to eliminate screens. You need to notice when you are using them as a substitute reward source and create space for the natural ones.
When to Seek Professional Help
The reward system recovery process is uncomfortable but temporary for most people. If anhedonia persists beyond 12 weeks with no improvement, or if you experience persistent feelings of hopelessness, inability to function at work or in relationships, or thoughts of self-harm at any point, reach out to a healthcare provider. Persistent anhedonia beyond the expected recovery window may indicate a pre-existing mood condition, such as depression, that was masked by cannabis use. SAMHSA's National Helpline is available at 1-800-662-4357, free, confidential, and available 24 hours a day.
The Reframe
Your reward system is not broken. It was recalibrated by a chemical that overstimulated it, and now it is in the process of finding its natural set point again. The flatness, the boredom, the inability to feel excited about things you know you care about, these are signs of a brain that is actively rebuilding, not one that is permanently impaired. Neuroplasticity is not a buzzword. It is the documented, observable capacity of your mesolimbic pathway to restore itself. Understanding exactly how THC took over the circuit gives you something most people do not have: a map. And a map makes the territory far less frightening.
The Bottom Line
THC hijacks the mesolimbic pathway, the brain's core reward circuit connecting the ventral tegmental area (VTA) to the nucleus accumbens. Melis et al. (2004, Journal of Neuroscience) demonstrated that THC increases VTA dopamine neuron firing by suppressing inhibitory signals, while Bossong et al. (2009, NeuroImage) confirmed measurable dopamine release increases in humans via PET imaging. Chronic use triggers three-level compensation: reduced VTA dopamine synthesis (2016 Molecular Psychiatry PET study), decreased D2 receptor sensitivity in the nucleus accumbens, and CB1 receptor downregulation confirmed by Hirvonen et al. (2012, Molecular Psychiatry). This produces anhedonia — the inability to enjoy natural rewards because they fall below the nucleus accumbens' raised threshold. CB1 receptors recover by day 28, with dopamine synthesis and D2 sensitivity normalizing between weeks 4 and 12. Evidence-based recovery accelerators include aerobic exercise (upregulates D2 receptors), structured novelty (engages VTA salience circuits), social connection (oxytocin modulates nucleus accumbens dopamine), and a "reward ladder" approach starting with small achievable activities.
Sources & References
- 1RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩