How to Quit Weed: A No-Judgment Step by Step Guide
Withdrawal & Recovery
72 Hours
The first 72 hours are the hardest part of quitting, and individual cravings peak at about 15 to 20 minutes then pass on their own.
Budney et al., Journal of Abnormal Psychology, 2003
Budney et al., Journal of Abnormal Psychology, 2003
View as imageIf you only read one thing
Pick a quit date, tell one person, throw out your stash, and plan how you'll spend the first three days. That's the formula. The first 72 hours are the worst part — cravings hit hard but each one only lasts about 15 to 20 minutes, then passes on its own. Most physical symptoms clear up within two to four weeks, and your brain fully recovers. If you slip up, it doesn't erase your progress. Just stop again and keep going.
You have decided to quit. Maybe you have been thinking about it for a while, maybe something happened today that made you say "enough." Either way, you are not looking for someone to convince you. You want to know how to actually do it. If you are still on the fence, the should I quit weed decision framework can help you work through that first.
This is the practical guide. No lectures about why weed is bad. No scare tactics. Just the specific steps, in order, that give you the best chance of quitting and staying quit. Everything here is based on behavioral research and what consistently works for people who have done this before you.
Key Takeaways
- Planning ahead before your quit date dramatically raises your chances of success
- The first 72 hours are the hardest part — and individual cravings peak at about 15 to 20 minutes then pass on their own
- Cold turkey and tapering both work, so neither approach is wrong
- Most acute withdrawal symptoms clear up within two to four weeks
- Slipping up does not erase your progress or mean you failed
- Research shows that pairing behavioral strategies with structured support significantly improves your odds of quitting for good
Before You Quit: The Preparation That Most People Skip
The biggest mistake people make is deciding to quit and then just stopping that same day with no plan. That can work, but it is like driving to a city you have never been to without checking the route first. A 2006 study by Dr. Alan Budney and colleagues in the Journal of Consulting and Clinical Psychology[1] found that combining behavioral strategies with structured support significantly improved outcomes in cannabis cessation. People who planned their quit had better results than people who just winged it.
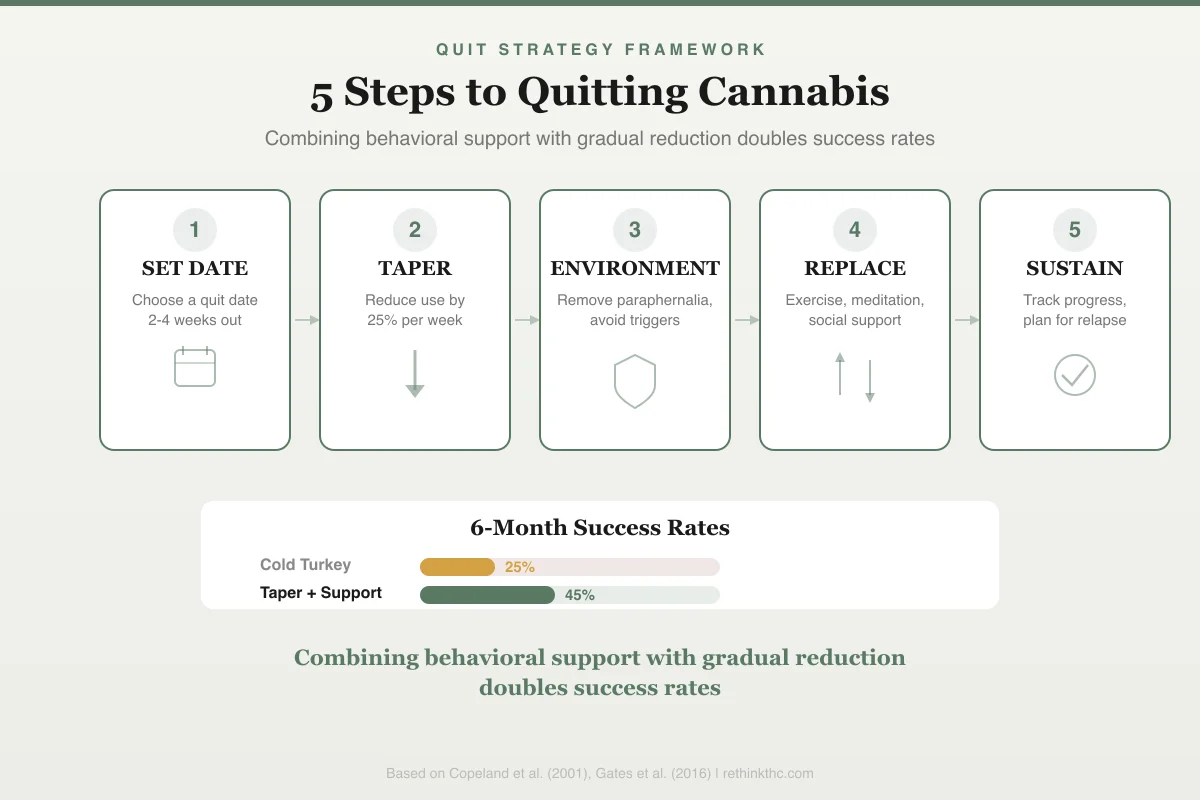
The framework below maps the five-step process that research supports, from setting a date through sustaining your quit long-term.
Quit Strategy Framework
5 Steps to Quitting Cannabis
Combining behavioral support with gradual reduction doubles success rates
SET DATE
Choose a quit date 2-4 weeks out
TAPER
Reduce use by 25% per week
ENVIRONMENT
Remove paraphernalia, avoid triggers
REPLACE
Exercise, meditation, social support
SUSTAIN
Track progress, plan for relapse
6-Month Success Rates
Here is what preparation actually looks like.
| Step | What to Do | Why It Matters |
|---|---|---|
| Pick a quit date | Choose a specific day 1–2 weeks out; avoid high-stress periods | Activates implementation intention; shifts from abstract goal to executable plan |
| Tell someone | Share your plan with one trusted person | Provides reality check during peak craving days |
| Remove stash and gear | Get rid of all cannabis, grinders, pipes, papers | Environmental cues trigger cravings independently of conscious desire |
| Stock supplies | Mild snacks, herbal tea, melatonin, journal, fidget items | Prevents the "I feel terrible and have nothing" spiral |
| Learn the timeline | Read the withdrawal timeline before quitting | Removes "something is wrong with me" panic when symptoms hit |
| Plan your first 72 hours | Clear your schedule if possible; have distraction toolkit ready | First 3 days are when most quit attempts fail |
Pick a Quit Date
Choose a specific day within the next one to two weeks. Not "soon." Not "when the time feels right." A date on the calendar. Write it down. Tell your phone to remind you.
Why this works: Research on behavior change has found that setting a specific quit date activates a psychological mechanism called implementation intention. When your brain attaches a behavior change to a concrete time and place, it shifts from abstract goal ("I should quit") to executable plan ("I am quitting on March 3rd"). That shift measurably increases follow-through.
Do not pick a day when you know life will be extra stressful. Do not pick the day before a big presentation or a family event. If you are already in the middle of a major life upheaval, the guide on quitting weed during a crisis like divorce or job loss covers how to handle that overlap. If possible, choose a Friday or a day where you have the next two to three days relatively free. The first 72 hours are the hardest, and having them overlap with high-demand obligations stacks the deck against you.
Tell Someone
You need at least one person who knows what you are doing. Not for accountability in the "check up on me" sense. For reality. When you are on day three and your brain is telling you this was a stupid idea and you should just smoke, having one person who can say "you told me you wanted this, and you are only on day three" is the difference between quitting and not quitting for a lot of people.
Pick someone who will not judge you and who will not try to talk you out of it. A friend, a partner, a sibling, someone in an online community. The format does not matter. The function does. If you are on the other side of this and trying to support someone else through it, the guide on how to help someone quit weed covers what actually helps and what backfires.
Remove Your Stash and Paraphernalia
If there is weed in your house, you will smoke it. This is not a willpower problem. This is how brains work. Research has demonstrated that environmental cues associated with drug use trigger cravings independently of conscious desire. Your grinder sitting on the shelf is a cue. Your pipe in the drawer is a cue. The rolling papers in your nightstand are a cue.
Get rid of it. Give it to someone. Throw it away. If you cannot bring yourself to throw it away, have the person you told in the previous step hold it or dispose of it. Clean the places where you used to store it. Wash the smell out of your smoking spot if you had one indoors.
This is not about trust or willpower. This is about not making yourself fight a craving with the solution sitting three feet away.
Stock Up on What You Will Need
The first week involves specific, predictable physical symptoms. Having the right supplies on hand prevents the "I feel terrible and have nothing to deal with it" spiral that leads to relapse.
Get these before your quit date: healthy snacks you can eat when your appetite is absent (crackers, bananas, toast, broth, anything mild), herbal tea or decaf options for the evenings when you would normally smoke, a journal or notebook for tracking how you feel, and over-the-counter melatonin if you want a mild sleep support option (see the full guide on supplements that may help during withdrawal). Some people find that having something to do with their hands helps, so consider gum, a stress ball, or something tactile.
Know What Is Coming
Read about the cannabis withdrawal timeline before you quit, not during. Understanding what to expect removes the panic of "something is wrong with me" when symptoms hit. Withdrawal is predictable. It peaks around days three to seven, and it ends. Knowing that timeline in advance is one of the most protective things you can do. The complete guide to cannabis withdrawal covers every symptom and why it happens.
Cold Turkey vs. Tapering: Neither Is Wrong
There are two basic approaches and people have strong opinions about both. Here is what the research actually says.
| Factor | Cold Turkey | Tapering |
|---|---|---|
| How it works | Stop completely on quit date | Gradually reduce over 1–3 weeks before quit date |
| Withdrawal intensity | Full force; first 72 hours are intense | Milder; receptor adjustment starts during taper |
| Research support | Most clinical cessation studies use this approach | Less studied for cannabis but well-established for other substances |
| Best for | All-or-nothing personalities; people who want it over with | People anxious about quitting; heavy concentrate users |
| Risk | Acute phase can feel overwhelming | Can become indefinite delay without firm end date |
| Timeline to recovery | Withdrawal clock starts immediately | Slightly delayed but gentler entry |
The honest answer is that both work. Choose the one that matches your personality. If you are an all-or-nothing person, cold turkey is probably better. If you know that jumping off a cliff will make you climb back up, tapering gives you a ramp. The critical piece either way is a non-negotiable quit date. If you are leaning toward stopping abruptly, the cold turkey quit guide walks through exactly what to expect hour by hour. For a deeper comparison of both methods, see cold turkey vs tapering, or if you are not sure whether full abstinence is necessary, read quit or cut back: which is better.
The First 72 Hours: The Part Most People Do Not Survive
Here is the reality. A meta-analysis of over 27,000 cannabis users found that roughly half of regular users experience clinically significant withdrawal, with symptoms peaking in the first week — making the first few days the most vulnerable window for quit attempts.[4] Not because people are weak, but because the first 72 hours are when withdrawal symptoms are ramping up, cravings are at their most aggressive, and you have not yet experienced any of the benefits of quitting. You are paying the cost with no visible return. That is the hardest psychological position to be in.
Here is how to get through it.
Hours 1 to 12: Easier Than You Think
The first half day is usually fine. You might feel some restlessness or mild anxiety, but nothing dramatic. Use this window to set up your environment. Clean your space. Go for a walk. Stock your fridge. You have energy and clarity right now that you will not have tomorrow. Use it.
Hours 12 to 24: The First Test
By the evening of day one, the cravings start. If you normally smoked at a specific time (before bed, after work, after dinner), that is when your brain will start asking for it. This is conditioned behavior, not weakness. Your brain has associated that time and place with THC for months or years.
Do something physically different during that window. If you normally smoked on the couch at 9 PM, do not sit on the couch at 9 PM. Go for a walk. Take a shower. Call someone. The craving needs the cue to fire at full strength. Change the cue and the craving weakens.
Hours 24 to 48: It Gets Real
Day two is where most people first think "I cannot do this." You probably slept poorly. You are irritable. Food does not appeal to you. You might feel anxious for no clear reason. You might be sweating more than usual.
The single most important thing to understand about cravings: they are waves, not constants. A craving rises, peaks at about 15 to 20 minutes, and then passes. Every single time. Research by Dr. Alan Marlatt at the University of Washington demonstrated this wave pattern across multiple substances. You do not need to outlast a craving forever. You need to outlast it for 20 minutes.
Build a distraction toolkit for those 20-minute windows: a specific playlist, a walk around the block, a set of pushups, a phone game that requires focus, cold water on your face, calling or texting the person who knows you are quitting. The content of the distraction matters less than its ability to consume your attention for the length of the craving.
Hours 48 to 72: The Peak Begins
By day three, you are entering the peak of acute withdrawal. Symptoms are at or near their worst, and research has found that the degree to which withdrawal disrupts normal daily functioning is one of the strongest predictors of relapse during a quit attempt.[3] Sleep is likely disrupted. Irritability is high. Your brain is actively recalibrating, and the gap between "THC is gone" and "my own system is back online" is at its widest.
This is where knowledge of the timeline saves you. You are at the hardest part. It does not get worse than this. Every hour from here is one hour closer to the other side. If you can get through day three, you can get through anything that follows it.
Week 1 Survival Guide
You made it past 72 hours. The acute peak is either here or just behind you. Here is how to handle the rest of the first week.
Sleep
Insomnia is the most common and most persistent withdrawal symptom. Your brain used THC to initiate sleep for so long that it temporarily does not know how to fall asleep without it. This is not permanent. It is a recalibration.
Practical steps that help: go to bed and wake up at the same time every day regardless of how much you slept. Keep your room cool and dark. No screens for 30 minutes before bed. If you are lying awake for more than 20 minutes, get up and sit in a dimly lit room until you feel drowsy, then go back to bed. Trying to force sleep is counterproductive. For a full breakdown of strategies, read the guide on how to sleep without weed.
Expect vivid, intense dreams when you do sleep. This is called REM rebound and it is your brain catching up on the dreaming stage that THC suppressed. It is temporary.
Appetite
You may have no appetite at all, or food may taste wrong. Eat anyway. Small, bland meals are fine. Your body still needs fuel, and skipping meals makes irritability, headaches, and fatigue worse. Bananas, toast, crackers, soup, and smoothies are standbys. Appetite typically returns within the first two weeks.[4]
Stay hydrated. Dehydration worsens every withdrawal symptom. Keep water within reach at all times.
Exercise
If you do one thing during the first week besides not smoking, exercise. Research has found that aerobic exercise activates endocannabinoid signaling in the brain's reward pathways, the same system that cannabis acts on.[6] Your dopamine system is recalibrating without THC's artificial boost, and exercise directly supports that recovery.
You do not need to run five miles. A 20-minute walk counts. Movement tells your brain to produce the chemicals it is currently short on. Exercise also improves sleep, reduces anxiety, and burns off the restless energy that makes the first week feel unbearable. The guide on exercise as medicine for quitting covers why it works neurologically, and working out during recovery has practical routines for each stage.
Emotional Regulation
You may feel emotions more intensely than you have in a long time. Sudden anger, unexpected sadness, anxiety that arrives from nowhere. This is your brain's emotional processing system running at full volume for the first time since you started using regularly. It overshoots before it stabilizes.
Name what you are feeling when it hits. "This is withdrawal irritability, not actual anger at this person." That small cognitive step creates distance between the emotion and your response to it. You will not do this perfectly. That is fine. The goal is awareness, not control. Journaling through withdrawal gives you a structured way to track and process these emotional shifts day by day.
Weeks 2 to 4: Building the New Normal
The acute phase is winding down. You are sleeping a little better. Your appetite is coming back. The cravings are still there, but they have lost their urgency. Now the challenge shifts from physical survival to psychological adjustment. Some people experience a pink cloud phase around this time, a burst of euphoria and optimism that feels amazing but can set you up for disappointment when it fades. Recognizing it for what it is helps you stay grounded.
Use the checklist below to make sure you have the practical foundations covered before moving into the habit-replacement phase.
Preparation Steps
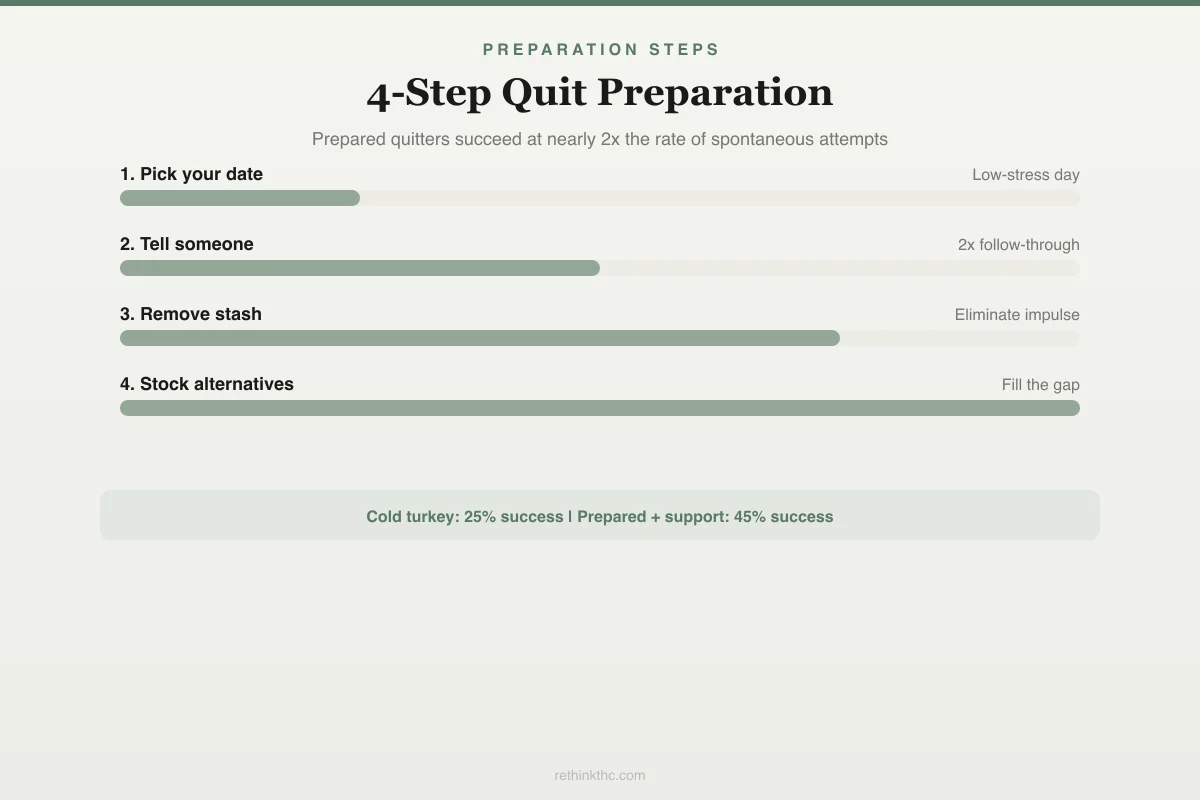
4-Step Quit Preparation
Prepared quitters succeed at nearly 2x the rate of spontaneous attempts.
Pick your date
Choose a day with low stress — not during deadlines, travel, or emotional events
Gives your brain a concrete commitment
Tell someone
One person you trust — partner, friend, therapist. Accountability doubles follow-through
2x more likely to follow through
Remove your stash
All of it. Pipes, papers, edibles, vape pens. If it's there at 2am, you'll use it
Eliminates impulsive relapse
Stock alternatives
Herbal tea, melatonin, exercise clothes, a book. Replace the ritual, not just the substance
Fills the behavioral gap
25%
Cold turkey success
45%
Prepared + support
Replacing the Ritual
For most regular users, weed was not just a substance. It was a ritual. The grinding, the packing, the lighting, the inhale. The way it signaled the end of the work day or the beginning of relaxation. Quitting removes the substance, but the ritual-shaped hole remains.
You need to fill it deliberately. If you smoked after work, replace that window with something specific: a walk, a shower, cooking, making tea, stretching. If smoking was your wind-down before bed, build a new wind-down routine that takes roughly the same time and occupies the same psychological space.
The replacement does not need to feel as good as smoking did. It needs to exist. An empty ritual slot is a craving trigger. A filled one is a new habit forming. The replacing the ritual guide has specific substitution strategies for every common smoking context.
Dealing with Boredom
This is bigger than it sounds. THC increases dopamine each time you use, which means everyday activities felt more engaging while you were using. Without that artificial boost, normal life can feel painfully flat. This is temporary. It is called anhedonia, and it resolves as your dopamine system normalizes, typically over weeks two through four with continued improvement for several months.
In the meantime, fight boredom with novelty. Try things you have not done before. New activities create small dopamine spikes without requiring the inflated reward response that THC provided. This is not about finding a "replacement high." It is about giving your reward system new inputs to calibrate around.
Social Situations
At some point someone will smoke around you. Maybe a friend, maybe at a party, maybe a roommate. Having a plan for this before it happens is essential. If you are also navigating the dating world sober, dating after quitting weed covers how to handle the social pressure and identity questions that come with that.
Options that work: leave the room when people light up (you do not need to announce why), bring your own drink or activity so your hands are not empty, have a response ready for when someone offers ("I am good, thanks"), and give yourself permission to leave the event entirely if the craving becomes too strong. Protecting your quit is more important than staying at any particular gathering. If you are wondering whether you can handle a concert or festival sober, the guide on going to a music festival without weed has specific strategies for high-stimulation environments. If you are wondering how to handle the conversation, telling your friends you are quitting covers the practical scripts and common reactions.
Common Pitfalls and How to Avoid Them
These are the patterns that trip up the most people between weeks one and four.
"Just one hit will not hurt." It will. Not because one hit is morally wrong, but because one hit reactivates the craving cycle your brain is working to shut down. Research on marijuana cessation found that a single lapse frequently led back to regular use, particularly when people interpreted the slip as proof they could not quit rather than a recoverable setback.[5] Your brain is in the process of downregulating its response to THC. One hit tells it to stop that process.
Romanticizing past use. Your brain will selectively remember the good parts: the laughs, the relaxation, the food tasting amazing. It will conveniently forget the reasons you decided to quit. Write those reasons down before your quit date and read them when the nostalgia hits.
Isolation. Withdrawal makes you want to be alone. Irritability makes social interaction feel harder. But isolation removes every external check on the "just smoke" voice in your head. You do not need to be social. You need to not be completely alone. Even texting someone counts. Be especially careful with social media, which can be a major trigger during this period through nostalgic posts, stoner content, and friends sharing their sessions.
Damaged relationships. If weed has already strained your relationships, the temptation is to use the guilt as a reason to give up on quitting ("it is already too late"). It is not. But recognizing how weed has affected your relationships can be a powerful motivator to stay the course.
Safety
ModerateDon't replace weed with alcohol
Concern
Many people increase alcohol consumption to fill the gap weed left. This disrupts sleep recovery, impairs dopamine recalibration, lowers inhibitions (making relapse more likely), and introduces a separate dependency risk.
What the research says
If you didn't drink much before quitting, don't start now. If you did drink, watch honestly whether your intake is creeping up. The goal is to let your brain heal, not swap one substance for another.
Particularly relevant for: Anyone quitting cannabis, especially if you already drink socially
What to do
Track your alcohol intake for the first month after quitting. If it's increasing, that's a signal to address directly — not ignore.
Clinical observations in cannabis cessation literature
Replacing weed with alcohol. This is extremely common and extremely counterproductive. Alcohol disrupts sleep, impairs the dopamine recovery you are in the middle of, lowers inhibitions (making a "just one hit" decision more likely), and introduces its own dependency risk. If you did not drink much before, this is not the time to start. If you did drink, be honest with yourself about whether your consumption is increasing to fill the gap that weed left.
If You Slip Up
You smoked. Maybe once, maybe for a day, maybe for a week.
Here is what that is not: failure. Here is what it is: information.
Research on relapse patterns across substances has found that slips are a normal, expected part of the quitting process. The majority of people who eventually quit successfully experienced at least one slip along the way. A slip becomes a full relapse only when you interpret it as proof that you cannot do this and stop trying.[5]
What to do: stop again as soon as you can. Do not wait for Monday or next month. Examine what triggered the slip. Was it a specific person, place, emotion, or time of day? That trigger is now a known variable you can plan around. Tell the person who knows you are quitting. Reset your timeline mentally without resetting your self-assessment. If you have already gone back and are trying to figure out your next move, the relapse recovery guide walks through exactly what to do. And if part of you regrets going back, that feeling of regret is worth examining because it contains important information about what you actually want.
You did not lose all of your progress. Your brain does not fully revert from one slip. The neural recovery you achieved is still mostly intact. Get back on track and keep going.
If You Are Not Sure About Quitting Completely
Some people reading this are not certain they want to quit permanently. Maybe you want to see what life is like without weed for a while. Maybe you want to reset your tolerance and then make a decision about long-term use from a clearer headspace.
That is a legitimate option. A structured tolerance break uses many of the same strategies in this guide but with a defined return date. It gives you the experience of being sober without the permanence that might feel overwhelming right now.
If a tolerance break is what gets you to actually stop and see what your brain does without THC, it is a better choice than an indefinite "I will quit eventually" that never happens.
When to Seek Professional Help
Everything in this guide covers the normal range of quitting. But some situations warrant professional support.
If you have tried to quit multiple times and consistently cannot get past the first week, or if you recognize the signs of cannabis use disorder in your own patterns, a therapist who specializes in substance use can help you identify what is keeping you stuck. Cognitive behavioral therapy (CBT) has the strongest evidence base for cannabis cessation and is specifically designed to break the thought and behavior cycles that drive relapse. You can also compare MA vs SMART Recovery vs therapy to find the support format that fits your situation.
If you are experiencing severe anxiety or depression during withdrawal that interferes with your ability to work, care for yourself, or maintain relationships, that is worth a professional conversation. Withdrawal can temporarily amplify pre-existing mental health conditions, and a provider can help distinguish between withdrawal symptoms that will resolve and conditions that need separate treatment.
If you experience thoughts of self-harm at any point during this process, reach out immediately. SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day, 365 days a year.
The Part Nobody Tells You
The hardest thing about quitting weed is not the physical withdrawal. It is the two to three weeks after the acute symptoms fade when your life looks the same but feels different. The evenings are longer. The boredom is louder. The things that used to entertain you need more time to feel engaging again.
This is the recalibration period. Your brain is rebuilding its reward system and its emotional regulation and its sleep architecture all at the same time. It is doing exactly what it is supposed to do, and it takes longer than anyone wants it to.
But it works. The data consistently shows full neurological recovery.[2] The people who have been through it consistently say the same thing: it was harder than expected, it was worth it, and the version of their life on the other side was one they could not have imagined from the middle of week one. If you need proof that it is possible, real quitting weed success stories from people who have been exactly where you are can help. And if the process feels like grieving a loss, that is because it is one. The grief is legitimate, and naming it makes it easier to move through.
The experience of quitting also varies by life stage. If you are quitting in your 20s, the identity and social dynamics are different than if you are quitting in your 30s, when career, family, and health concerns tend to carry more weight.
You are not going to feel like this forever. You just have to get through the part where it feels like you will.
The Bottom Line
Quitting weed is a practical, plannable process with predictable stages. Preparation before your quit date — picking a date, telling someone, removing your stash — dramatically increases success rates. The first 72 hours are the hardest part because withdrawal symptoms are ramping up while benefits have not yet appeared. Individual cravings peak at about 15 to 20 minutes and then pass. Most acute symptoms resolve within two to four weeks, with sleep taking up to 45 days. Both cold turkey and tapering are valid approaches. Slipping up is a normal part of cessation, not a sign of failure.
Sources & References
- 1RTHC-00218·Budney, Alan J. et al. (2006). “Paying for Clean Tests Worked During Treatment. Therapy Helped It Last..” Journal of Consulting and Clinical Psychology.Study breakdown →PubMed →↩
- 2RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩
- 3RTHC-00538·Allsop, David J. et al. (2012). “Withdrawal That Disrupted Daily Life Was Tied to Relapse in a Small Study.” PLOS ONE.Study breakdown →PubMed →↩
- 4RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩
- 5RTHC-00051·Stephens, R S et al. (1994). “How People Explained Their First Marijuana Lapse Predicted Whether They Returned to Regular Use.” Addictive behaviors.Study breakdown →PubMed →↩
- 6RTHC-00608·Raichlen, David A. et al. (2012). “Runner's High Has an Endocannabinoid Signature in Humans. Dogs Show It Too..” Journal of Experimental Biology.Study breakdown →PubMed →↩
What the Research Shows
This section synthesizes 224 peer-reviewed studies on Cannabis Cessation Interventions. Stronger evidence means more consistency across study types.
First meta-analysis of cannabis withdrawal prevalence: 47% of regular/dependent users experienced clinically significant withdrawal across 23 studies and 27,000+ participants
Strong EvidenceMeta-analysis of 4 RCTs found cannabis users with PTSD still benefited from trauma-focused therapy, but attended fewer sessions and showed less improvement in other substance use
Strong EvidenceAnalysis of 920 participants found reducing cannabis use ~50% in frequency and ~75% in amount was associated with clinician-assessed improvement
Strong EvidenceWhere Scientists Disagree
Areas where research shows conflicting results or ongoing scientific debate.
Among 1,481 heavy smokers trying to quit with nicotine patches, marijuana users had half the odds of success
Moderate EvidenceAmong 75 marijuana users who lapsed after treatment, those who blamed themselves and saw the cause as permanent and pervasive were more likely to return to regular use over six months
Moderate EvidenceSelf-efficacy for avoiding marijuana predicted frequency of post-treatment use better than complete abstinence
Moderate EvidenceIn 199 smokers trying to quit, alcohol use predicted failure at all follow-up points
Moderate EvidenceWhat We Still Don't Know
- Long-term prospective studies tracking outcomes over 5+ years are largely absent from the literature.
- Research on diverse populations (different ages, ethnicities, and medical backgrounds) remains limited.
Evidence Breakdown
Distribution of study types in this research area. Higher-tier evidence (meta-analyses, RCTs) provides stronger conclusions.
Research Timeline
How our understanding of this topic has evolved.
Pre-2000
7 studies published. Predominantly observational and review studies.
2000–2009
8 studies published. Includes 2 RCTs.
2010–2014
42 studies published. Includes 11 RCTs, 2 strong-evidence studies.
2015–2019
48 studies published. Includes 13 RCTs, 5 strong-evidence studies.
2020–present
119 studies published. Includes 5 meta-analyses, 33 RCTs, 18 strong-evidence studies.