Should I Quit Weed? A Decision Framework (Not a Lecture)
Withdrawal & Recovery
30-Day Test
A 30-day break is the single most useful experiment you can run because cognitive function sharpens within 72 hours and CB1 receptors reset by day 28, showing you what cannabis is actually doing for you and to you.
Molecular Psychiatry, 2012
Molecular Psychiatry, 2012
View as imageIf you only read one thing
Only about 9% of people who try cannabis develop dependence — so this isn't an automatic yes. The best way to find out if you should quit is a 30-day break. Your thinking sharpens within 72 hours, your brain receptors reset by day 28, and by the end you'll know what cannabis was actually doing for you versus to you. If a 30-day break sounds impossible, that reaction alone is your answer.
You are probably here because you have been going back and forth on this question for a while. Maybe weeks. Maybe months. Maybe years. The fact that you are searching for an answer suggests something has shifted in how you feel about your use, even if you cannot name exactly what.
This is not an article that will tell you what to do. It is a structured way to think about a genuinely complicated question so you can arrive at your own answer with more clarity than you started with.
Key Takeaways
- "Should I quit weed?" deserves a decision framework — not a lecture — because the right answer depends on your specific situation
- Only about 9% of people who try cannabis develop dependence, so most users are not in a spot where quitting is medically necessary
- A structured cost-benefit analysis of your cannabis use beats guilt, fear, or cultural pressure in either direction
- A 30-day break is the single most useful experiment you can run, because it shows you what cannabis is actually doing for you and to you
- Your thinking sharpens within 72 hours and your CB1 receptors reset by about day 28, so a trial break is not a permanent commitment
- If a 30-day break feels impossible or terrifying, that reaction alone tells you how much power cannabis has over your daily life
Why This Question Is Harder Than It Sounds
"Should I quit weed?" seems like it should have a straightforward answer. But it doesn't, because cannabis occupies a strange position in modern life. It is simultaneously normalized and stigmatized, medically useful and recreationally misused, harmless for some people and genuinely harmful for others.
Decision Framework
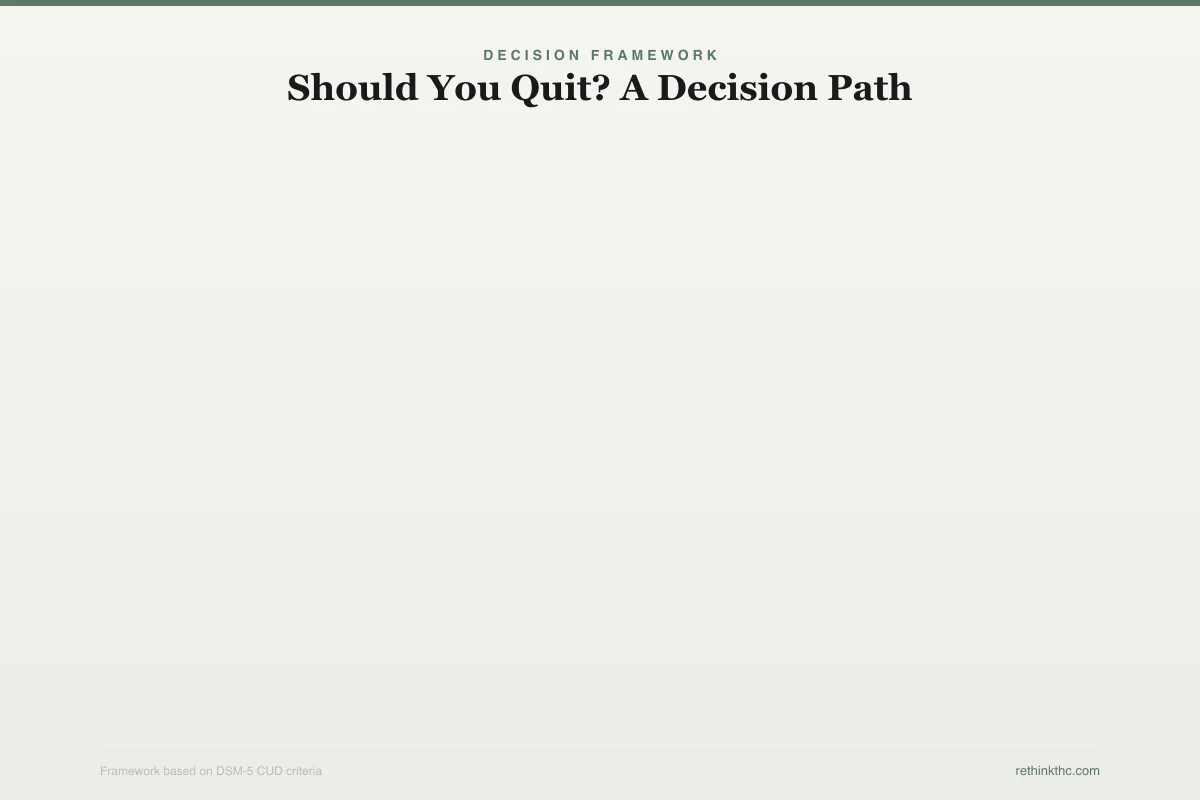
Should You Quit? A Decision Path
Follow the questions to find your starting point — not a verdict, a framework
Has cannabis caused problems in your life?
Work, relationships, finances, health, motivation
Can you control your use?
Set limits and follow them
Try moderation
Set strict rules for 30 days
Consider quitting
Loss of control is a key CUD sign
Current use may be fine
No problems, no dependence signs — re-evaluate periodically
Still worth a 30-day test if you are curious about life without it
The difficulty is compounded by the fact that most of the voices weighing in have an agenda. Anti-drug messaging says yes, always quit, cannabis is ruining your life. Cannabis culture says no, never quit, it is a harmless plant that the government demonized for political reasons. Neither of these positions is interested in your specific situation. They are interested in being right.
Your situation is specific. The answer depends on factors that no article can know without you: how much you use, how long you have been using, what it does for you, what it costs you, and what your life looks like with and without it. What follows is a framework for examining those factors honestly.
Signs It Might Be Time
None of these signs in isolation means you must quit. But if several of them resonate, they are worth sitting with.
You are using more than you intend to. You tell yourself "just one hit" and smoke the whole bowl. You plan to use only at night and find yourself starting in the afternoon. You buy a certain amount expecting it to last a week and it is gone in a few days. The gap between what you plan and what you do is one of the earliest indicators of a shift from voluntary to compulsive use.
You have tried to cut back and could not. This is different from never having tried. Many people have never attempted to reduce their use because it has never felt like a problem. But if you have genuinely tried to use less, set rules for yourself, made promises to yourself or others, and repeatedly failed to follow through, that pattern carries information. It may indicate that you have crossed into Cannabis Use Disorder, which is the clinical term for problematic cannabis use.
You cannot imagine socializing, sleeping, or relaxing without it. When cannabis becomes the prerequisite for basic activities, rather than an enhancement to them, the relationship has shifted. If the thought of attending a party sober, falling asleep without a bowl, or unwinding after work without an edible produces genuine anxiety, that suggests psychological dependence. Not moral failure. Dependence.
It is affecting your work, relationships, or finances. Maybe your performance at work has slipped. Maybe your partner has expressed concern. Maybe you are spending more than you can comfortably afford. These are concrete, observable consequences, and they are harder to rationalize away than abstract concerns.
Your tolerance has escalated significantly. If the amount that used to get you high barely registers now, or if you have moved from flower to concentrates because flower stopped working, your brain has adapted to a level of THC exposure that is no longer casual. A 2012 study by Hirvonen and colleagues, published in Molecular Psychiatry, used brain imaging to show[1] that daily cannabis users have significantly fewer available CB1 receptors, the brain structures that THC activates. This downregulation is the biological reality behind tolerance.
Signs It Might Not Be Necessary
Just as important as recognizing when quitting matters is recognizing when it does not. Not every cannabis user needs to quit, and framing all cannabis use as inherently problematic is not honest or helpful.
Self-Assessment
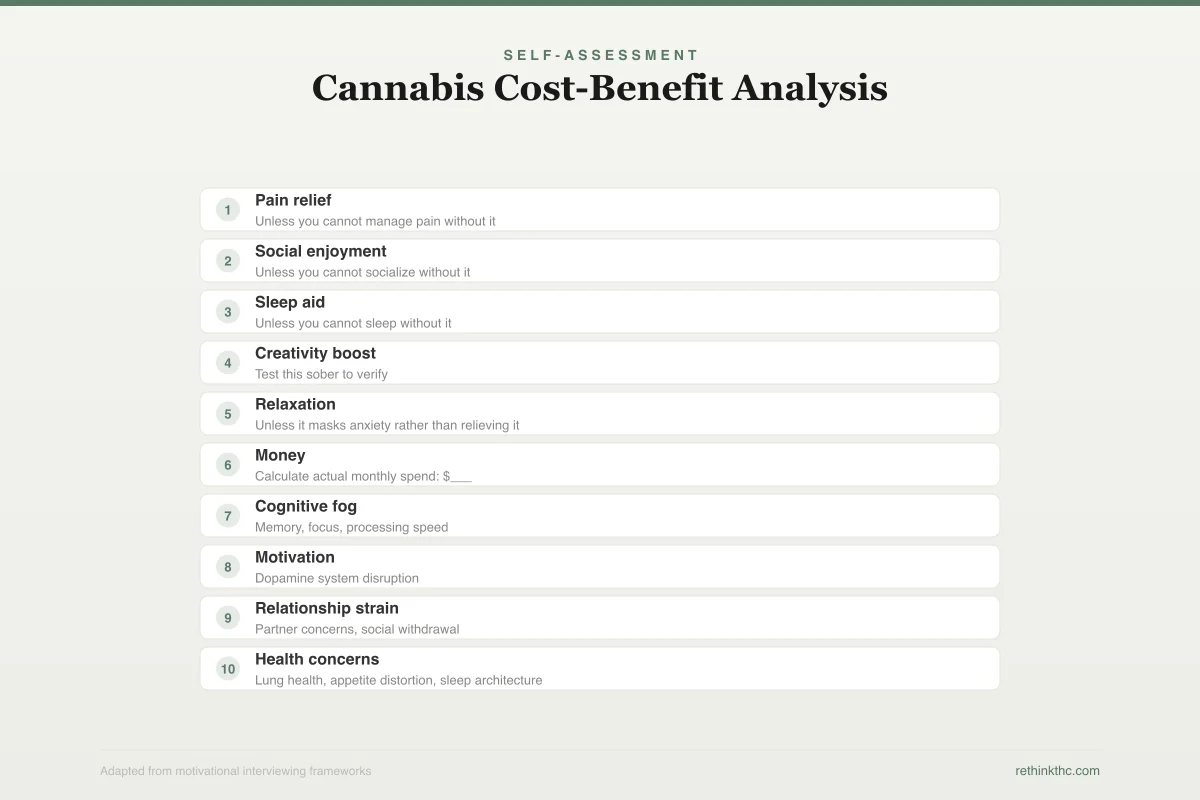
Cannabis Cost-Benefit Analysis
Rate each item 1-5 for personal importance — if costs outweigh benefits, that is data
What Cannabis Gives You
Pain relief
Unless you cannot manage pain without it
Social enjoyment
Unless you cannot socialize without it
Sleep aid
Unless you cannot sleep without it
Creativity boost
Test this sober to verify
Relaxation
Unless it masks anxiety rather than relieving it
What Cannabis Costs You
Money
Calculate actual monthly spend: $___
Cognitive fog
Memory, focus, processing speed
Motivation
Dopamine system disruption
Relationship strain
Partner concerns, social withdrawal
Health concerns
Lung health, appetite distortion, sleep architecture
Key insight: Some “benefits” are dependency in disguise. If you cannot sleep, socialize, or relax without cannabis, that is not a benefit — it is a sign of dependence.
Your use is occasional and stable. You use a few times a month or on weekends, the amount has not escalated over time, and you do not feel pulled toward using more. This pattern suggests recreational use that has not developed into dependence.
You experience no negative consequences. Your work is fine. Your relationships are fine. Your health is fine. Your finances are fine. If cannabis is genuinely not causing problems in any domain of your life, the case for quitting is less about necessity and more about preference.
You do not experience withdrawal symptoms. A 2020 meta-analysis by Bahji and colleagues, published in JAMA Network Open, found[2] that approximately 47% of regular cannabis users experience withdrawal symptoms when they stop. If you have taken breaks without irritability, sleep disruption, appetite changes, or anxiety, your body is not physically dependent in a way that demands attention.
You are not using cannabis to avoid dealing with something. There is a meaningful difference between using cannabis because you enjoy it and using it because you cannot face your anxiety, boredom, sadness, or stress without it. The first is recreation. The second is self-medication, and even if it "works" in the short term, it tends to prevent you from developing the coping skills that would serve you better long-term.
The Cost-Benefit Analysis
The most useful exercise you can do right now is not reading another article. It is sitting down with a piece of paper (or a blank document) and making two lists.
What cannabis gives you. Be honest and specific. Relaxation. Sleep. Creativity. Social lubrication. Pain management. Stress relief. Entertainment enhancement. A sense of ritual. A community of other users. Whatever it is, write it down without judgment. These benefits are real, and dismissing them does not help you make a clear-eyed decision.
What cannabis costs you. Same rules: honest and specific. Money (calculate the actual monthly number). Motivation. Cognitive sharpness. Physical health (lungs, appetite distortion). Emotional availability. Memory. Time spent high that could have been spent on other things. Career momentum. Relationship quality. Self-respect, if using feels like something you are hiding or ashamed of. Whatever it costs, write it down without minimization.
Now look at both lists. If the benefits column is significantly longer and more meaningful than the costs column, quitting may not be the right call for you right now. If the costs column is longer, heavier, or contains items that genuinely matter to your future, that is data worth respecting.
One important nuance: some of the "benefits" on your list may actually be dependency in disguise. If "sleep" is on the benefits list, but you literally cannot sleep without cannabis, that is not a benefit. It is a sign that cannabis has disrupted your natural sleep architecture and you now rely on it for something your brain should be able to do on its own. Similarly, if "anxiety relief" is on the benefits list, but your anxiety is worse overall since you started using, the "benefit" is actually just temporary relief from a problem that cannabis itself is contributing to.
The 30-Day Test
If you are genuinely unsure whether to quit, the single most useful thing you can do is run an experiment. Take 30 days off and see what happens.
DSM-5 Criteria
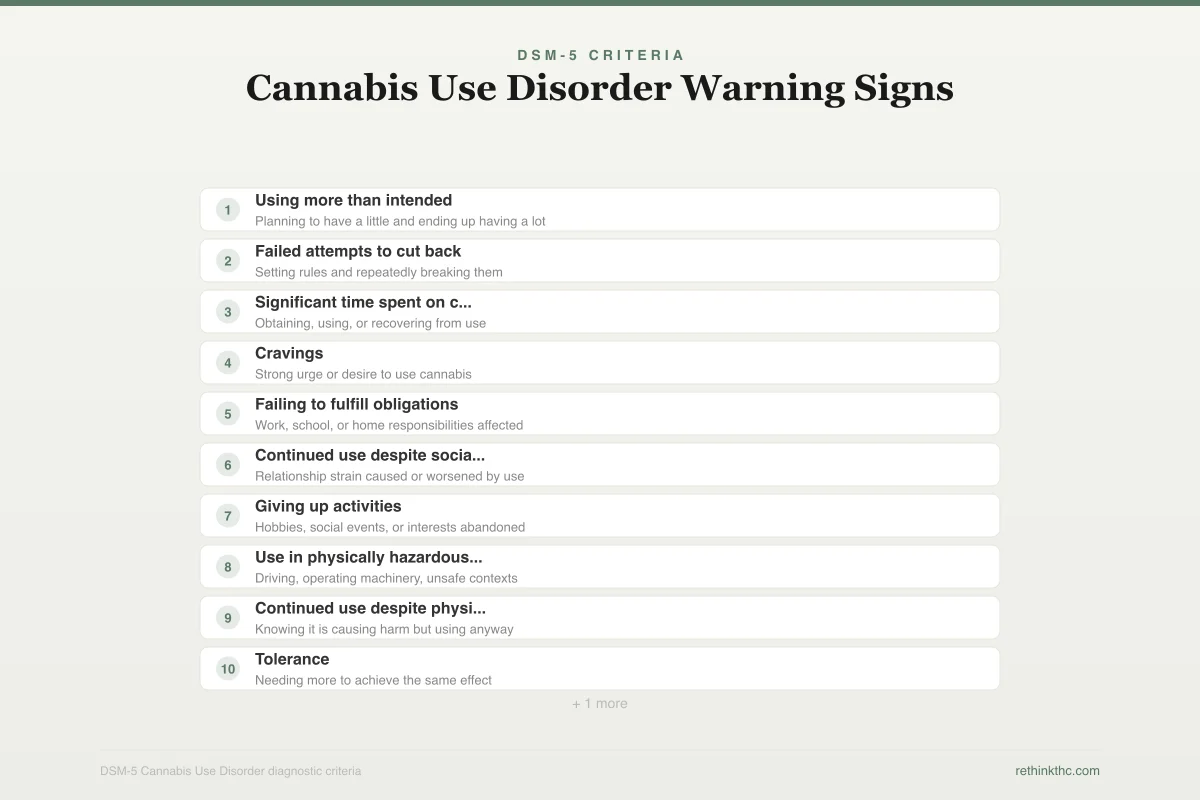
Cannabis Use Disorder Warning Signs
Count how many apply to your situation over the past 12 months
Using more than intended
Planning to have a little and ending up having a lot
Failed attempts to cut back
Setting rules and repeatedly breaking them
Significant time spent on cannabis
Obtaining, using, or recovering from use
Cravings
Strong urge or desire to use cannabis
Failing to fulfill obligations
Work, school, or home responsibilities affected
Continued use despite social problems
Relationship strain caused or worsened by use
Giving up activities
Hobbies, social events, or interests abandoned
Use in physically hazardous situations
Driving, operating machinery, unsafe contexts
Continued use despite physical/psychological problems
Knowing it is causing harm but using anyway
Tolerance
Needing more to achieve the same effect
Withdrawal
Irritability, insomnia, appetite loss when stopping
Your count: ___ / 11 — 0-1 = no CUD, 2-3 = mild, 4-5 = moderate, 6+ = severe
This is not a commitment to quit forever. It is data collection. Here is what 30 days gives you.
Cognitive clarity. A 2018 study by Scott and colleagues, published in JAMA Psychiatry, found[3] that cognitive deficits associated with cannabis use begin to remediate after just 72 hours of abstinence. By day 30, you will have a much clearer sense of how cannabis was affecting your thinking, memory, and mental sharpness.
Receptor recovery. The Hirvonen 2012 research found[1] that CB1 receptors return to approximately normal levels after about 28 days of abstinence. This means that by the end of your 30-day test, your brain's endocannabinoid system will have largely recalibrated. You will be operating at (or near) your neurological baseline for the first time in however long you have been using daily.
Withdrawal data. If you experience significant withdrawal symptoms (insomnia, irritability, appetite loss, anxiety, sweating), that tells you your body was more dependent than you may have realized. If you experience minimal discomfort, that tells you something different. Either way, the information is valuable. You can learn more about what withdrawal involves in our cannabis withdrawal guide.
Emotional data. How do you feel at the end of 30 days? More motivated? Less? More anxious? Less? More bored? More creative? More present in your relationships? The answers to these questions, derived from actual experience rather than speculation, will tell you more about your relationship with cannabis than any article, podcast, or Reddit thread ever could.
Craving data. Pay attention to when and why cravings hit. After work? When stressed? When bored? When socializing? When alone? The pattern of your cravings reveals what cannabis was doing for you psychologically, which is essential information whether you decide to quit, moderate, or return to your previous level of use.
If a 30-day break feels impossible or terrifying, that reaction is itself data. Something you cannot imagine going 30 days without has more power over your life than a recreational choice typically does.
For practical guidance on what the first week looks like, our first week quitting guide covers the timeline and what to expect.
The Dependence Question: Where Do the Numbers Land?
Understanding the research on cannabis dependence can help you calibrate your own risk without catastrophizing or dismissing it.
A foundational study by Anthony and colleagues, published in 1994 in Experimental and Clinical Psychopharmacology, established that approximately 9% of people who have ever used cannabis develop dependence. For context, the comparable rates are roughly 32% for tobacco, 23% for heroin, 17% for cocaine, and 15% for alcohol. Cannabis is not the most addictive substance available, but it is not without addictive potential either.
A 2014 review by Volkow and colleagues in the New England Journal of Medicine noted that the dependence rate rises to about 17% among people who begin using as teenagers. Age of onset matters significantly.
And the picture is changing. A 2015 study by Hasin and colleagues, published in JAMA Psychiatry, found[4] that CUD prevalence among American adults doubled between 2001 and 2013, from 1.5% to 2.9%. Rising potency, greater availability, and shifting cultural norms have all contributed. If you want to understand the science of cannabis addiction more deeply, our article on whether weed is addictive covers the full picture.
The 9% figure means most cannabis users do not develop dependence. But "most people are fine" is not the same as "you are fine." Your individual relationship with cannabis is what matters, and the cost-benefit analysis and 30-day test are better tools for evaluating it than population statistics.
The Moderation Question
Maybe you are reading this thinking: "I do not want to quit entirely. Can I just cut back?"
The 30-Day Test
30-Day Experiment Protocol
Not a commitment to quit forever — a data collection exercise
Set your start date
Tell one trusted person
Remove supplies or lock them away
Stock alternatives: sleep aids, exercise gear, projects
Withdrawal peaks around days 2-3
Use the craving window: wait 20 minutes
Exercise daily, even just a walk
Sleep will be disrupted — expect vivid dreams
Most withdrawal symptoms fading
Track improvements: sleep, appetite, clarity
Notice what cannabis was masking
Cravings less frequent, less intense
CB1 receptors approaching normal levels
Cognitive function largely restored
New routines forming
Clearer picture of costs vs benefits
How do you feel overall?
What improved? What got worse?
Do you want to go back — or keep going?
If returning: start at 25-50% of previous dose
If 30 days feels impossible: that reaction is itself data. Something you cannot imagine going 30 days without has more power over your life than a recreational choice typically does.
Maybe. It depends on where you fall on the dependence spectrum.
If your use is problematic but not yet at the level of Cannabis Use Disorder, moderation is a viable option for many people. Setting specific rules (weekends only, no concentrates, one session per day), sticking to them, and seeing whether your life improves is a reasonable approach. The biological basis for this is solid: even partial reduction in THC exposure allows your CB1 receptors to begin recovering, which means you get more effect from less cannabis over time.
If you have tried to moderate and failed repeatedly, that is important information. People who meet criteria for moderate to severe CUD tend to do poorly with moderation strategies. A 2006 study by Budney and colleagues, published in the Journal of Consulting and Clinical Psychology, studied[5] 90 adults in a 14-week treatment program and found that structured abstinence-based approaches, combined with cognitive behavioral therapy and incentives, produced better outcomes than less structured approaches.
The honest test is this: can you set a rule and follow it for 30 days? Not 29 days. Not 30 days with a few exceptions. Thirty consecutive days of following the rule you set. If yes, moderation may work for you. If no, that tells you something about the degree of control you currently have.
Our article on quitting weed versus cutting back explores this choice in detail. And if you decide moderation is worth trying, our tolerance break guide is a good place to start.
What Quitting Actually Involves
If you decide to quit, here is the brief version of what to expect. (For the detailed version, see our guide on how to quit weed.)
The first week is the hardest. Withdrawal symptoms for most people peak between days 2 and 6, and can include irritability, insomnia, decreased appetite, anxiety, and restlessness. These symptoms are uncomfortable but temporary, and they are a sign that your brain is recalibrating, not that something is going wrong.
Cognitive function begins recovering quickly. The Scott 2018 research shows[3] measurable improvement within 72 hours. By two weeks, most people report significantly clearer thinking.
The receptor reset takes about a month. Hirvonen's imaging data shows[1] CB1 receptors approaching normal availability by day 28. This is when the physical adjustment is largely complete.
The psychological adjustment takes longer. Learning to sleep, socialize, manage stress, and experience boredom without cannabis is a process that unfolds over weeks to months. It is not about willpower. It is about building new neural pathways for coping and enjoyment. The benefits of quitting weed often become more apparent during this phase.
Making Your Decision
There is no universal right answer to "should I quit weed?" There is only the answer that is right for your situation, and you are the only person who can determine that.
What you can do is make the decision with better information than you had before. Run the cost-benefit analysis. Consider the 30-day test. Be honest about whether your use pattern has crossed from recreational to compulsive. Look at the concrete evidence in your own life rather than arguing about abstract positions.
If you decide to quit, you are not admitting defeat. You are making a strategic decision about what serves your life best.
If you decide not to quit, you are not in denial (as long as you have genuinely engaged with the questions above). You are making a choice that reflects your honest assessment of the costs and benefits.
And if you decide you are not sure yet, that is fine too. The 30-day test is there whenever you are ready.
When to Seek Professional Help
If you recognize multiple signs of problematic use but feel unable to change your pattern on your own, professional support can make a significant difference. Therapists who specialize in substance use can help you clarify your goals, develop strategies, and work through the psychological dimensions of dependence that self-directed approaches sometimes miss.
If you are experiencing severe anxiety, depression, or other mental health symptoms that are intertwined with your cannabis use, a professional can help you untangle what is caused by cannabis, what is masked by it, and what exists independently.
SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day, 7 days a week. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
The Bottom Line
The question "should I quit weed?" deserves a framework, not a predetermined answer. A structured cost-benefit analysis is more useful than guilt or cultural pressure. About 9% of people who try cannabis develop dependence, meaning most users are not in a situation where quitting is medically necessary. Key warning signs include consistently using more than intended, failed attempts to cut back, inability to imagine basic activities without cannabis, and escalating tolerance. A 30-day break is the single most informative experiment: cognitive function recovers within 72 hours, CB1 receptors normalize by approximately day 28, and the experience reveals what cannabis is actually doing for you and to you. If moderation has failed repeatedly, structured abstinence-based approaches with professional support produce better outcomes.
Sources & References
- 1RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩
- 2RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩
- 4RTHC-00975·Hasin, Deborah S. et al. (2015). “The Largest Study of Cannabis Addiction in America.” JAMA Psychiatry.Study breakdown →PubMed →↩
- 5RTHC-00218·Budney, Alan J. et al. (2006). “Paying for Clean Tests Worked During Treatment. Therapy Helped It Last..” Journal of Consulting and Clinical Psychology.Study breakdown →PubMed →↩