Is Weed Addictive? What the Research Actually Shows
Withdrawal & Recovery
47%
of daily cannabis users experience clinically significant withdrawal when they stop — confirmed by a meta-analysis of 23 studies with over 27,000 participants.
Bahji et al., JAMA Network Open, 2020
Bahji et al., JAMA Network Open, 2020
View as imageIf you only read one thing
Yes, weed can be addictive — but not for everyone. About 9 out of 100 people who try it develop a real problem. If you use it every day, the odds go up a lot: roughly half of daily users get withdrawal symptoms when they stop. The risk depends on how often you use, how strong the product is, how old you were when you started, and your genetics. It's less addictive than cigarettes or alcohol, but 'less' doesn't mean 'zero.'
You have probably heard two completely opposite answers to this question. One side says weed is totally harmless, not addictive at all, just a plant. The other side lumps it in with heroin and calls it a gateway drug. If you are asking because your own relationship with cannabis has started to feel like something you cannot easily control, both of those answers are failing you. The real answer is more complicated, more honest, and ultimately more useful than either extreme.
Key Takeaways
- Cannabis dependence is real, but the "addictive vs. not addictive" framing misses the point — it exists on a spectrum
- About 9% of everyone who tries cannabis develops Cannabis Use Disorder, and that number jumps to roughly 30% among regular users
- Physical dependence (tolerance, withdrawal) and psychological dependence (cravings, compulsive use) are both real and often overlap
- Most people who use cannabis never develop a problem — risk depends on frequency, potency, age of first use, genetics, and mental health
- Cannabis carries less dependence risk than tobacco (~32%) or alcohol (~15%), but that does not make the risk zero
- Rising THC potency — from ~4% in the 1990s to 15%+ in flower and 60-90% in concentrates — is likely pushing real-world dependence rates higher than older estimates suggest
The Binary Question Is the Wrong Question
Asking "is weed addictive?" is a bit like asking "is food addictive?" The question assumes a yes-or-no answer when the reality operates on a spectrum. Some people use cannabis occasionally and never think twice about it. Others use it daily for years and walk away without much difficulty. And others find that what started as recreational use has shifted into something that feels compulsive, something they continue despite wanting to stop.
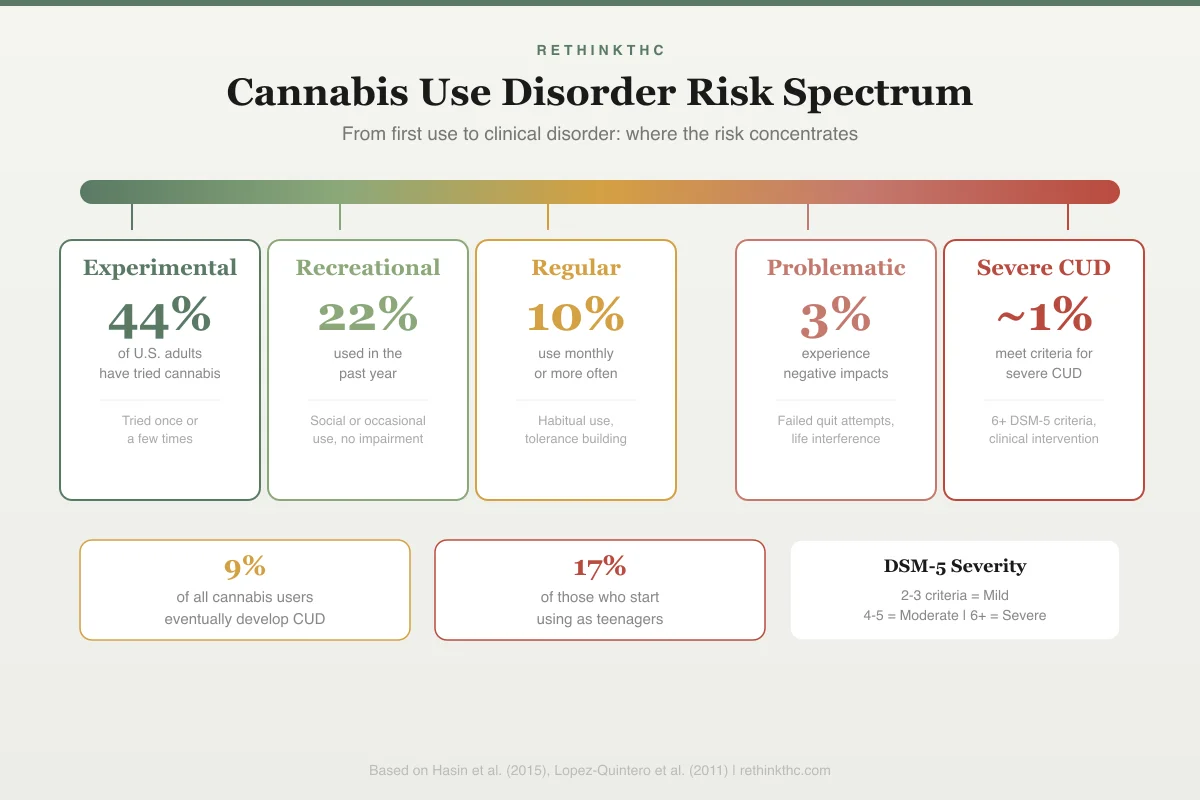
The spectrum below shows where different use patterns fall on the dependence continuum, from no risk through clinical disorder.
Is Weed Addictive?
Cannabis Use Disorder Risk Spectrum
44%
Experimental
of U.S. adults have tried cannabis
Tried once or a few times
22%
Recreational
used in the past year
Social or occasional use, no impairment
10%
Regular
use monthly or more often
Habitual use, tolerance building
3%
Problematic
experience negative impacts
Failed quit attempts, life interference
~1%
Severe CUD
meet criteria for severe CUD
6+ DSM-5 criteria, clinical intervention
9%
of all cannabis users eventually develop CUD
17%
of those who start using as teenagers
DSM-5 Severity
2-3 = Mild · 4-5 = Moderate · 6+ = Severe
All three of those experiences are valid. All three are supported by research. The problem is that the public conversation treats them as mutually exclusive, as if one person's experience disproves another's. It does not.
What the science actually shows is that cannabis can produce both physical dependence and psychological dependence in a meaningful percentage of users. For a deeper look at the science behind cannabis addiction, including DSM-5 criteria and brain research, the evidence is substantial. Not everyone. Not even most people. But enough that dismissing the possibility is irresponsible, and enough that you deserve a clear-eyed look at the data if you are questioning your own use.
Physical Dependence vs. Psychological Dependence
These two terms get thrown around a lot, often inaccurately. Here is what they actually mean.
Physical dependence means your body has adapted to the presence of a substance and reacts when it is removed. The hallmarks are tolerance (needing more to get the same effect) and withdrawal (experiencing physical symptoms when you stop). Cannabis produces both. Your brain's CB1 receptors (the primary receptors that THC activates) reduce in number and sensitivity with regular use, a process called downregulation. When you stop, the temporarily impaired endocannabinoid system produces real, measurable withdrawal symptoms: insomnia, irritability, appetite loss, sweating, and anxiety. A 2020 meta-analysis by Bahji and colleagues published in JAMA Network Open found that approximately 47% of daily cannabis users experience clinically significant withdrawal symptoms upon stopping.[1]
Psychological dependence means you feel a strong compulsion to use the substance even when you recognize it is causing problems. You might reorganize your day around it, use it to manage emotions you do not know how to handle otherwise, or find that you cannot relax, sleep, or socialize without it. Psychological dependence does not require physical withdrawal to be real. It involves changes in your brain's reward and motivation pathways, particularly dopamine signaling, that make the substance feel necessary even when intellectually you know it is not.
In practice, these two types of dependence often overlap. Someone who is physically dependent usually experiences psychological dependence as well. The article on physical vs. psychological dependence explores the neuroscience behind both pathways. The distinction matters mainly because it helps explain why "I don't get withdrawal symptoms" does not necessarily mean "I can stop whenever I want."
What the DSM-5 Actually Says
The clinical term for problematic cannabis use is Cannabis Use Disorder (CUD), and it has been in the DSM-5 (the Diagnostic and Statistical Manual of Mental Disorders, the standard reference used by psychiatrists and therapists) since 2013. The DSM-5 lists 11 criteria for CUD, including:
- Using more than intended or for longer than intended
- Wanting to cut down but being unable to
- Spending significant time obtaining, using, or recovering from cannabis
- Cravings
- Failing to fulfill major responsibilities because of use
- Continued use despite social or interpersonal problems
- Giving up important activities because of use
- Use in physically hazardous situations
- Continued use despite knowing it causes physical or psychological problems
- Tolerance
- Withdrawal
Meeting two or three criteria within a 12-month period qualifies as mild CUD. Four to five is moderate. Six or more is severe. If you are unsure where you fall, a structured cannabis use disorder self-assessment can help you evaluate your own patterns. You can also review the signs of cannabis use disorder in more practical, everyday terms. This spectrum-based approach replaced the old binary categories of "abuse" and "dependence," and it reflects the reality that problematic cannabis use is not an on-off switch. You can have a mild problem. You can have a severe problem. And you can have no problem at all.
The Numbers: How Common Is It?
Here is where the data gets important, because both sides of the debate cherry-pick statistics.
A widely cited estimate puts the overall rate of cannabis dependence at about 9% of all people who try it. That means roughly 91 out of 100 people who use cannabis will not develop a use disorder. This is the number legalization advocates tend to highlight, and it is broadly consistent with longitudinal data.
But the picture shifts when you narrow the lens. Among current regular users, approximately 30% meet at least some criteria for CUD.[2] Among daily users, that Bahji 2020 meta-analysis in JAMA Network Open found that roughly 47% experience withdrawal symptoms when they stop.[1] These are the numbers that get left out of the "it's just a plant" conversation.
For context, here is how cannabis compares to other substances in terms of dependence rates among people who have ever used them:
| Substance | Dependence Rate (Among Ever-Users) | Withdrawal Severity | Medical Risk of Withdrawal |
|---|---|---|---|
| Tobacco | ~32% | Moderate | Not life-threatening |
| Alcohol | ~15% | Moderate to severe | Can be life-threatening |
| Cannabis | ~9% | Mild to moderate | Not life-threatening |
| Opioids | ~23% | Severe | Can be life-threatening |
| Cocaine | ~17% | Moderate (primarily psychological) | Not life-threatening |
Comparative dependence rates based on longitudinal epidemiological surveys.
A 2015 national epidemiological study by Hasin and colleagues in JAMA Psychiatry found that 30.6% of current cannabis users met criteria for CUD, up from previous estimates, suggesting that increasing potency and changing use patterns may be shifting the prevalence upward.[2] A follow-up analysis using updated DSM-5 criteria confirmed that 2.5% of all U.S. adults and 6.3% met lifetime criteria for cannabis use disorder.[9]
Cannabis carries a lower risk of dependence than tobacco or alcohol. That is a fact. But "lower risk" is not "no risk." Average THC potency has increased dramatically, from roughly 4% in the 1990s to over 15% in flower today[8], with concentrates in legal markets averaging 68.7% THC.[3] These higher potency products drive faster CB1 receptor downregulation, and the real-world dependence numbers may be shifting upward as a result. For more on the gap between public perception and the evidence, see cannabis perception vs. the science gap.
Why Some People Develop Problems and Others Do Not
If the vast majority of people who try cannabis never develop a disorder, what makes some individuals more vulnerable? Research has identified several consistent risk factors.
| Risk Factor | Impact on CUD Risk | Key Finding |
|---|---|---|
| Age of first use | ~3x higher in adolescents vs. young adults | Adolescent brain more vulnerable to lasting neuroadaptation[4] |
| Frequency | Dose-response: daily >> weekly >> monthly | Daily use produces deepest CB1 receptor downregulation |
| Potency | Higher THC = faster tolerance and dependence | Concentrates (60–90% THC) accelerate the cycle |
| Genetics | 40–60% of vulnerability is heritable | Twin studies confirm genetic predisposition[6] |
| Mental health | Significant increase with anxiety, depression, PTSD, ADHD | Self-medication creates reinforcement loop |
| Sex | Males have higher prevalence; females escalate faster | Women may progress from use to disorder more quickly |
Age of first use. This is one of the strongest predictors. A 2025 longitudinal study found that adolescents were over three times more likely to develop Cannabis Use Disorder than young adults, because the developing brain is more vulnerable to lasting neuroadaptation.[4] The adolescent brain is still developing, particularly in the prefrontal cortex (the area responsible for impulse control and decision-making), and THC exposure during this critical window can alter developmental trajectories in ways that adult-onset use does not.
Frequency and duration. Weekly use carries more risk than monthly use. Daily use carries substantially more risk than weekly. Years of daily use produces deeper CB1 receptor downregulation than months. The dose-response relationship is consistent across the research. PET imaging by D'Souza and colleagues showed that daily users have significantly reduced CB1 receptor density compared to non-users.[5]
Potency. Today's cannabis products are not what was available 30 years ago. Average THC concentrations have risen from roughly 4% in the 1990s to over 15% in flower[8] and 60-90% in concentrates.[3] Higher THC exposure means more aggressive receptor downregulation, faster tolerance development, and a steeper withdrawal curve. Concentrated delivery methods like weed vape pens are a particular concern because of how efficiently they deliver high-potency THC.
Genetics. Twin studies estimate that 40-60% of the vulnerability to cannabis dependence is heritable. An Australian twin study by Lynskey and colleagues confirmed significant genetic contributions to cannabis dependence risk.[6] Variations in genes affecting CB1 receptor density, endocannabinoid metabolism, and dopamine signaling all play a role. This is not destiny. It is predisposition.
Mental health. People with anxiety, depression, PTSD, or ADHD are more likely to develop problematic cannabis use, often because cannabis initially provides relief for their symptoms. A meta-analysis by Lev-Ran and colleagues found significant associations between cannabis use and depression[7], and a 2019 meta-analysis linked adolescent cannabis use to significantly increased risk of both anxiety and depression in young adulthood.[10] The short-term relief creates a reinforcement loop that can progress to dependence, particularly when the underlying condition is not being treated through other means.
Safety
ModerateAdolescent use carries outsized risk
Concern
Teens who use cannabis are over 3 times more likely to develop Cannabis Use Disorder than adults who start later. Adolescent use is also linked to nearly 3.5 times higher risk of suicide attempts in young adulthood.
What the research says
The developing brain is more vulnerable to lasting changes from THC. Most of this risk is specific to regular use before the brain finishes maturing (around age 25). Occasional adult use carries far lower risk.
Particularly relevant for: Anyone under 25, parents of teens
What to do
Delay first use as long as possible. If you started young and feel dependent, that context matters — bring it up with a counselor who understands cannabis-specific issues.
Skumlien et al. (2025); Gobbi et al. (2019), JAMA Psychiatry
The Tolerance, Dependence, Disorder Progression
For many people who do develop problems, the path follows a recognizable pattern.
It starts with tolerance. You notice you need more to get the same effect, so you increase your dose or switch to higher-potency products. This is your CB1 receptors downregulating in response to consistent THC exposure.[5]
Tolerance slides into dependence. You start to notice that you feel "off" on days you do not use. Sleep is worse. Appetite drops. Irritability creeps in. You may not identify these as withdrawal symptoms, especially if you have been told withdrawal does not happen with cannabis. So you use again, and the symptoms resolve, reinforcing the pattern.
Dependence can progress to a use disorder when cannabis begins causing clear problems in your life but you continue anyway. Missing commitments. Spending money you do not have. Using when you promised yourself you would not. At this stage, the neurological pull is strong enough that willpower alone often feels insufficient.
Not everyone who develops tolerance will progress to dependence. Not everyone who develops dependence will meet criteria for a use disorder. But understanding the progression helps you recognize where you are on the spectrum before it moves further than you want it to.
Why Both Extremes Are Wrong
Saying "weed is not addictive" is wrong because it ignores the roughly 30% of regular users who meet CUD criteria, the 47% of daily users who experience withdrawal, and the well-documented neuroscience of CB1 receptor downregulation and tolerance. It leaves people who are struggling feeling gaslit by the very communities they thought understood cannabis.
Saying "weed is as bad as heroin" is equally wrong. Cannabis withdrawal is not life-threatening. It does not produce the acute medical danger of opioid, alcohol, or benzodiazepine withdrawal. The dependence rate is lower than tobacco, alcohol, or opioids. And the vast majority of people who use cannabis do so without ever developing a disorder.
The honest position is in the middle: cannabis can produce real dependence in a meaningful minority of users, particularly those who use frequently, start young, use high-potency products, or have pre-existing mental health conditions. If that describes you, you are not broken and you are not weak. Your brain responded to a chemical exposure in the way that brains are designed to respond. For a comprehensive overview of what to expect when you stop and how to navigate the process, the complete guide to cannabis withdrawal covers it in detail. For a step-by-step plan, see how to quit weed.
When to Seek Professional Help
If you have tried to quit or cut back multiple times without success, that is not a character flaw. It is a sign that the neurological adaptation is significant enough to benefit from structured support.
Talk to a doctor or therapist if you are experiencing severe withdrawal symptoms that interfere with daily life, if cannabis use is damaging your relationships or work, or if you are using cannabis to manage mental health symptoms that need their own treatment. For those weighing their options, the article on whether rehab is necessary for weed explores the spectrum of support available. If you are experiencing thoughts of self-harm, reach out to a professional immediately.
SAMHSA's National Helpline is free, confidential, and available 24 hours a day, 7 days a week: 1-800-662-4357. They can connect you with local support resources regardless of your insurance or financial situation.
You Deserve an Honest Answer
The fact that you searched "is weed addictive" means you are thinking critically about your own experience rather than accepting someone else's script. That matters. The answer is not a simple yes or no. Cannabis can be addictive for some people, and the risk is influenced by factors both within and outside your control. Knowing where you fall on that spectrum, and understanding the biology behind it, puts you in a much stronger position to make decisions that actually work for your life. Whether that means quitting, cutting back, or simply understanding what is happening in your brain, the knowledge is yours now. Use it on your own terms.
The Bottom Line
Cannabis dependence is real but exists on a spectrum, not as a binary. A widely cited estimate puts Cannabis Use Disorder at about 9% of all people who try cannabis, rising to roughly 30% among regular users, with 47% of daily users experiencing withdrawal. Both physical dependence (tolerance, withdrawal, and measurable brain changes) and psychological dependence (compulsive use, emotional reliance) are documented. Risk factors include early age of first use, daily frequency, high-potency products, genetic predisposition, and co-occurring mental health conditions. Cannabis carries lower dependence risk than tobacco or alcohol, but "lower risk" is not "no risk," and dramatically increased THC potency may be shifting the real-world numbers upward.
Sources & References
- 1RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩
- 2RTHC-00975·Hasin, Deborah S. et al. (2015). “The Largest Study of Cannabis Addiction in America.” JAMA Psychiatry.Study breakdown →PubMed →↩
- 3RTHC-01523·Smart, Rosanna et al. (2017). “Inside Washington State's Legal Cannabis Market: THC Levels, Prices, and the Rise of Concentrates.” Addiction (Abingdon.Study breakdown →PubMed →↩
- 4RTHC-07677·Skumlien, Martine et al. (2025). “Adolescents Were 3x More Likely Than Young Adults to Develop Cannabis Use Disorder Over 12 Months.” Communications medicine.Study breakdown →PubMed →↩
- 5RTHC-01134·D'Souza, Deepak Cyril et al. (2016). “Brain Cannabinoid Receptors Drop With Heavy Use, Then Rebound Within Days of Stopping.” Biological Psychiatry: Cognitive Neuroscience and Neuroimaging.Study breakdown →PubMed →↩
- 6RTHC-00585·Lynskey, Michael T et al. (2012). “Large Australian twin study found cannabis use, abuse, and early onset were all highly heritable.” Twin research and human genetics : the official journal of the International Society for Twin Studies.Study breakdown →PubMed →↩
- 7RTHC-00823·Lev-Ran, Shaul et al. (2014). “Across 22 Longitudinal Studies, Cannabis Use Tracked With Higher Odds of Later Depression.” Psychological Medicine.Study breakdown →PubMed →↩
- 8RTHC-01144·ElSohly, Mahmoud A. et al. (2016). “U.S. Cannabis Potency Tripled Over Two Decades While CBD Nearly Vanished.” Biological Psychiatry.Study breakdown →PubMed →↩
- 9RTHC-01172·Hasin, Deborah S et al. (2016). “National Survey Finds 2.5% of US Adults Had Cannabis Use Disorder in the Past Year, and Most Never Got Treatment.” The American journal of psychiatry.Study breakdown →PubMed →↩
- 10RTHC-02048·Gobbi, Gabriella et al. (2019). “Adolescent cannabis use linked to 37% higher depression risk and 3.5x higher suicide attempt risk in young adulthood.” JAMA psychiatry.Study breakdown →PubMed →↩