Is Cannabis Addictive? What the DSM-5 and Brain Science Say
Balanced Cannabis Science
9%
About 9% of people who try cannabis develop dependence, rising to 17% for those who start as teenagers and 25 to 50% among daily users, with CB1 receptor changes confirmed by brain imaging that reverse within 28 days.
Hasin et al., JAMA Psychiatry, 2015
Hasin et al., JAMA Psychiatry, 2015
View as imageIf you only read one thing
Yes, weed can be addictive — but not for most people. About 9 out of 100 people who try cannabis develop dependence. That number jumps to 17 out of 100 if you started as a teenager, and about half of daily users get real withdrawal symptoms when they stop. Your brain physically changes with heavy use (fewer receptors, less natural calming chemicals), but the changes reverse within about a month of stopping. Cannabis is less addictive than tobacco, alcohol, or opioids — but 'less addictive' isn't the same as 'not addictive.'
The claim that cannabis is not addictive has become so widespread that many people who are clearly dependent on it do not recognize what is happening. They assume that because cannabis is not heroin, what they are experiencing cannot be dependence. Meanwhile, the clinical evidence has been accumulating for decades. Cannabis dependence is not a matter of opinion. It is a diagnosable condition with defined criteria, documented brain changes, and population-level prevalence data.
This article is not an argument for prohibition or a scare piece. It is a look at what the diagnostic criteria, brain imaging research, and epidemiological data actually show. The science is more nuanced and more useful than either the "totally harmless" or "gateway drug" narrative.
Key Takeaways
- The DSM-5 recognizes Cannabis Use Disorder as a diagnosable condition with 11 criteria and three severity levels (mild, moderate, severe)
- About 9% of people who try cannabis develop dependence — but that rate climbs to 17% for those who start as teenagers, and roughly 47% of daily users get withdrawal symptoms
- Cannabis dependence involves measurable brain changes: CB1 receptor downregulation, reduced endocannabinoid production, and altered dopamine signaling
- The rate of Cannabis Use Disorder doubled between 2001 and 2013, right alongside rising THC potency
- Cannabis has a lower dependence rate than tobacco, alcohol, or opioids — but "lower" is not "zero," and the myth that it is not addictive leaves struggling users without support
- Brain imaging shows CB1 receptors start recovering within 2 days of quitting and return to normal by about day 28, so dependence-related brain changes are fully reversible
What the DSM-5 Says
The DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition) is the standard diagnostic reference used by psychiatrists, psychologists, and therapists across the United States. It has included Cannabis Use Disorder (CUD) as a recognized condition since its publication in 2013.
Dependence Rates
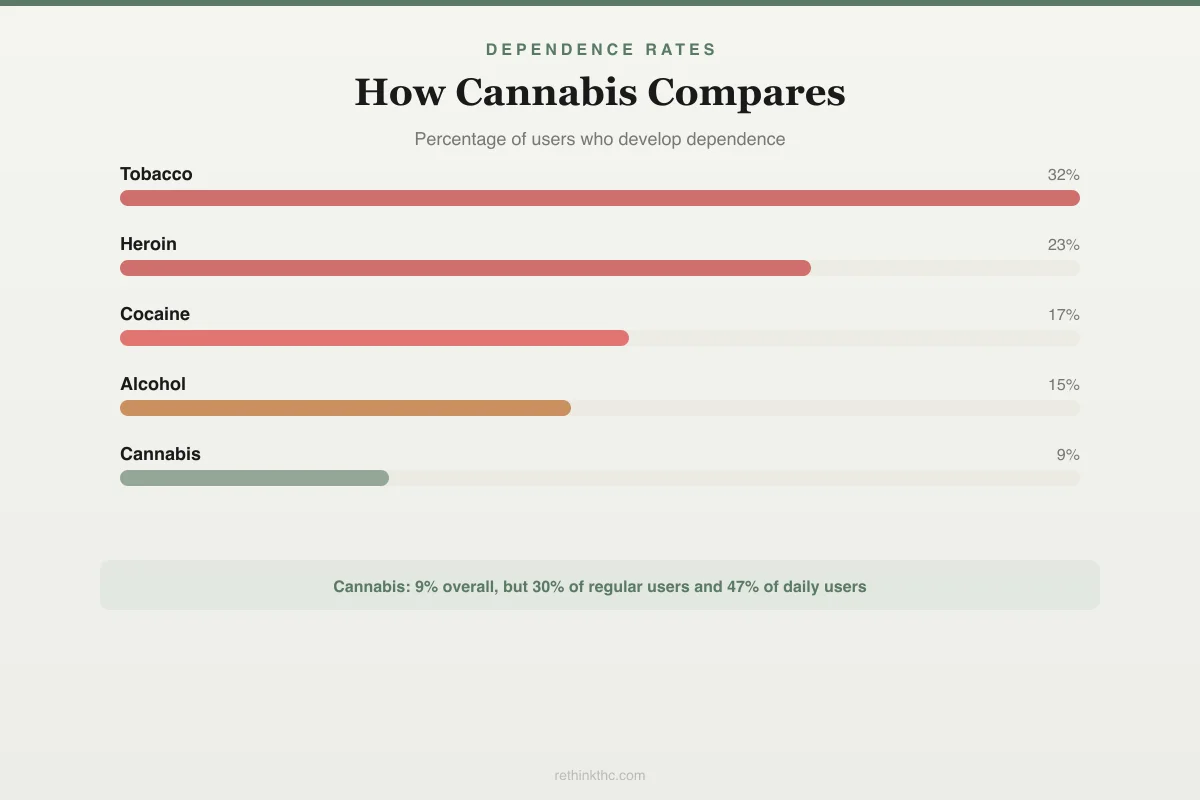
How Cannabis Compares to Other Substances
% of users who develop dependence. Cannabis is lower overall — but risk stratifies dramatically by use pattern.
Cannabis risk by use pattern
9%
All who ever try
30%
Regular users
47%
Daily users w/ withdrawal
17%
Started before 18
The DSM-5 lists 11 diagnostic criteria for CUD:
- Using cannabis in larger amounts or over a longer period than intended
- Persistent desire or unsuccessful efforts to cut down or control use
- Spending a great deal of time obtaining, using, or recovering from cannabis
- Cravings or a strong urge to use
- Recurrent use resulting in failure to fulfill major role obligations
- Continued use despite persistent social or interpersonal problems caused or worsened by use
- Giving up or reducing important social, occupational, or recreational activities because of use
- Recurrent use in physically hazardous situations
- Continued use despite knowledge of a persistent physical or psychological problem caused or worsened by cannabis
- Tolerance (needing more for the same effect, or diminished effect with the same amount)
- Withdrawal (characteristic withdrawal syndrome, or using cannabis to relieve or avoid withdrawal symptoms)
Meeting two or three criteria within a 12-month period qualifies as mild CUD. Four to five is moderate. Six or more is severe. The spectrum-based approach replaced the older binary categories of "abuse" and "dependence," reflecting the clinical reality that problematic cannabis use is not an on-off switch. For a practical guide to evaluating whether these criteria apply to your own use, the signs of cannabis use disorder article walks through each one.
The Neuroscience of Cannabis Dependence
The reason cannabis can produce dependence is not cultural or psychological in some vague sense. It is rooted in specific, measurable changes to brain chemistry that have been documented through imaging studies and molecular research.
Receptor Downregulation
Your brain's CB1 receptors are the primary targets of THC. When these receptors are activated repeatedly by chronic THC exposure, your brain protects itself by reducing the number of available receptors on cell surfaces, a process called downregulation. A 2012 PET imaging study by Hirvonen and colleagues, published in Molecular Psychiatry, provided direct visual evidence[1]: chronic cannabis users had significantly fewer available CB1 receptors across multiple brain regions compared to non-users.
This receptor reduction is what tolerance looks like at a biological level. Your brain literally has fewer receptors for THC to activate, so you need more THC to produce the same effect.
Disrupted Endocannabinoid Production
Alongside receptor downregulation, chronic THC use causes your brain to reduce its natural production of endocannabinoids (anandamide and 2-AG). When external THC is flooding the system, the brain scales back its own manufacturing. This is efficient adaptation, not dysfunction. But it creates a state of dependence: your endocannabinoid system now requires external THC to function at baseline because it has stopped maintaining itself internally.
Withdrawal as Evidence of Dependence
When you remove THC from a brain that has downregulated its receptors and reduced its natural endocannabinoid production, the result is a specific, predictable set of symptoms. Budney's 2004 review in American Journal of Psychiatry was one of the foundational papers establishing the validity[2] of cannabis withdrawal as a clinical syndrome. The documented symptoms include irritability, anxiety, insomnia, decreased appetite, restlessness, depressed mood, and physical discomfort.
A 2020 meta-analysis by Bahji and colleagues in JAMA Network Open analyzed data across multiple studies and found that approximately 47% of regular or dependent cannabis users experience clinically significant withdrawal symptoms upon cessation.[3] For a full breakdown of withdrawal as a clinical syndrome, the cannabis withdrawal syndrome article covers the diagnostic criteria and symptom patterns.
The Population Data
Individual brain changes tell part of the story. Population-level data tells the rest.
Overall Dependence Rate
The foundational epidemiological work by Anthony and colleagues, published in 1994 in Experimental and Clinical Psychopharmacology, established that approximately 9% of people who have ever used cannabis develop dependence at some point in their lives. For context, here is how that compares to other substances:
- Tobacco: approximately 32%
- Heroin: approximately 23%
- Cocaine: approximately 17%
- Alcohol: approximately 15%
- Cannabis: approximately 9%
Cannabis has the lowest dependence rate on this list. That fact is important and should not be ignored. But 9% of an increasingly large user population is a substantial number of people, and it represents roughly one in eleven users developing a clinically significant problem.
Adolescent Vulnerability
The 9% figure is a lifetime average that obscures significant variation by age of onset. Volkow and colleagues' 2014 review in the New England Journal of Medicine documented that the dependence rate rises to approximately 17% for people who begin using cannabis during adolescence. That is nearly double the overall rate.
The adolescent brain is more vulnerable because it is still developing. The prefrontal cortex (responsible for impulse control, planning, and decision-making) does not fully mature until the mid-twenties. Chronic THC exposure during this window appears to produce more persistent neuroadaptations than equivalent exposure during adulthood.
Prevalence Is Rising
The problem is not static. A 2015 study by Hasin and colleagues in JAMA Psychiatry found that the prevalence[4] of Cannabis Use Disorder among American adults had doubled from 1.5% in 2001-2002 to 2.9% in 2012-2013. More people are using cannabis, more are using it frequently, and more are developing diagnosable problems with it.
Potency Is Rising Too
This increase in CUD prevalence has coincided with a dramatic increase in THC potency. ElSohly and colleagues' 2016 analysis in Biological Psychiatry documented[5] that average THC content in confiscated cannabis roughly tripled between 1995 and 2014. Concentrates and extracts, which now make up a growing share of the market, can contain 60-90% THC. Higher potency means more aggressive receptor downregulation, faster tolerance development, and a steeper path to dependence.
The Meier Study and Adolescent Cognitive Risk
A 2012 study by Meier and colleagues, published in PNAS, followed[6] 1,037 individuals from birth to age 38 in Dunedin, New Zealand. It found that participants who began persistent, regular cannabis use during adolescence showed an average decline of 8 IQ points that was not fully recovered after cessation. This study is frequently cited because of its longitudinal design (following the same individuals over decades) and its control for various confounding factors.
The finding is specific to adolescent-onset, persistent use. It does not apply to adult-onset use or occasional use. But it reinforces the point that the developing brain responds differently to chronic THC exposure than the mature brain does.
Psychosis Risk With High-Potency Daily Use
Di Forti and colleagues' 2019 study in The Lancet Psychiatry examined[7] cannabis use patterns across 11 sites in Europe and Brazil. The findings were striking: daily cannabis use was associated with three times the risk of a first episode of psychosis compared to never-use. Daily use of high-potency cannabis (THC content above 10%) was associated with five times the risk.
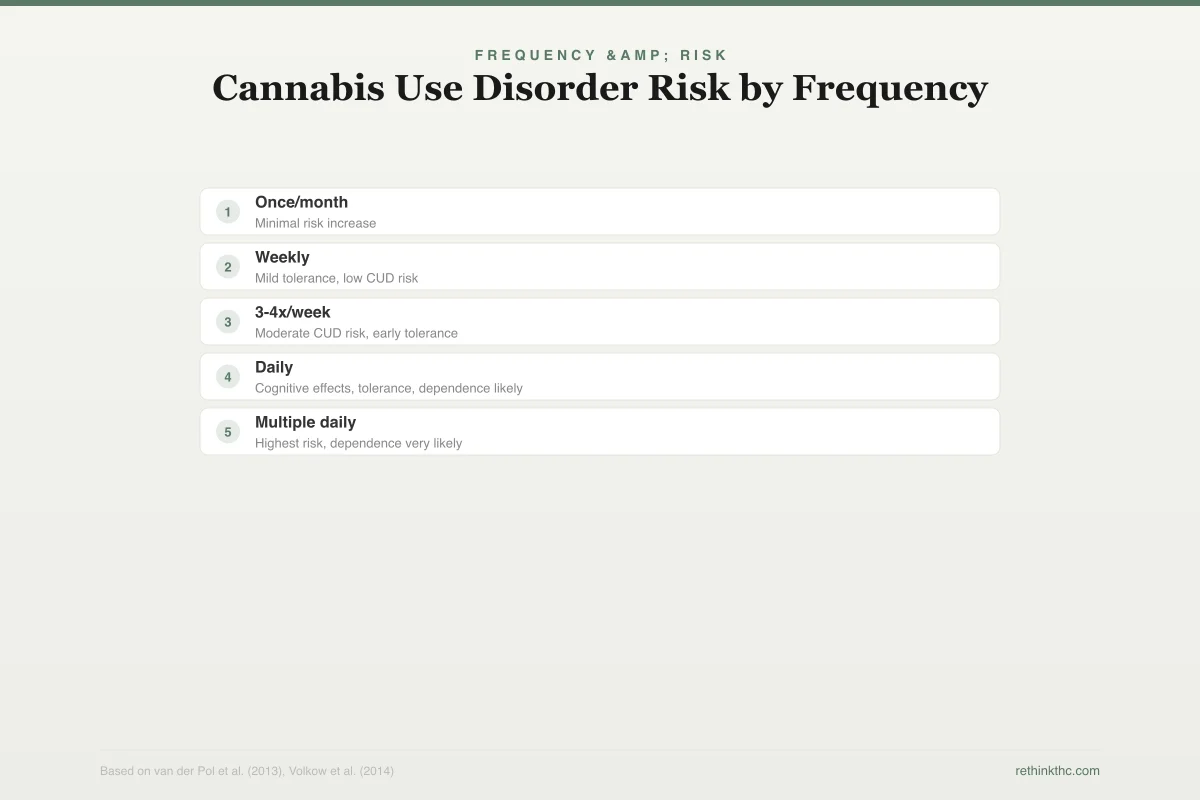
Frequency & Risk
Cannabis Use Disorder Risk by Frequency
Relative risk of CUD compared to non-use baseline
~1x
~2x
~5x
~9x
>9x
Once/month
Weekly
3-4x/week
Daily
Multiple daily
Frequency is the strongest behavioral predictor of cannabis-related problems
This does not mean cannabis causes psychosis in most users. The absolute risk remains low. But for individuals with genetic predisposition to psychotic disorders, high-potency daily use represents a meaningful and avoidable risk factor. This finding is relevant to the addiction question because compulsive daily use of high-potency products is precisely the pattern that CUD describes.
Why the "It Is Not Addictive" Myth Persists
Given the weight of evidence, why do so many people still believe cannabis cannot be addictive? Several factors contribute.
The comparison trap. Cannabis withdrawal is not life-threatening. It does not produce the acute medical danger of opioid, alcohol, or benzodiazepine withdrawal. People equate "addictive" with "can kill you if you stop," and since cannabis withdrawal does not reach that threshold, they conclude it is not real dependence. But the DSM-5 does not define addiction by withdrawal severity alone. It defines it by a pattern of use that causes impairment and distress despite the desire to stop.
Slow onset. Cannabis dependence typically develops gradually over months or years of regular use. There is no dramatic moment of becoming addicted. The progression from occasional use to tolerance to dependence to disordered use is subtle enough that many people do not notice it happening until they try to stop and cannot.
Cultural identity. For many users, cannabis is woven into social identity, stress management routines, and personal philosophy. Acknowledging that it might be causing problems can feel like betraying a community or admitting failure. This is not a weakness. It is a well-documented psychological dynamic that applies to any substance or behavior that carries social meaning.
Outdated information. Much of what the public "knows" about cannabis comes from research and messaging that predates the current potency landscape. The cannabis available today is a fundamentally different product than what was studied in the 1970s and 1980s, but public perception has not caught up.
What Makes Cannabis Different
Being evidence-based means acknowledging what cannabis is not, alongside what it is.
Cannabis dependence is real, but it is not equivalent to opioid or alcohol dependence. The overall dependence rate (9%) is lower than any other commonly used recreational substance except possibly psychedelics. Withdrawal, while genuinely uncomfortable, resolves on its own within weeks and does not carry medical risk. The is weed addictive overview covers the broader spectrum of what dependence looks like in practical terms.
Most people who use cannabis, even regularly, do not develop a use disorder. The majority of those who do develop one fall in the mild category. Cannabis does not produce the rapid, devastating physical deterioration associated with methamphetamine, heroin, or alcohol use disorder.
None of these facts erase the reality of CUD. They contextualize it. Understanding that cannabis occupies a specific place on the risk spectrum, lower than many substances but meaningfully above zero, is more useful than either exaggeration or denial.
The Recovery Evidence
The same brain imaging research that documents the problem also documents the solution. Hirvonen's 2012 study[1] showed that CB1 receptors begin recovering within two days of abstinence and approach normal levels by approximately 28 days. D'Souza and colleagues' 2016 study in Biological Psychiatry: Cognitive Neuroscience and Neuroimaging confirmed[8] that this recovery process begins rapidly once THC exposure stops.
The brain changes that produce dependence are not permanent. They are adaptations that reverse when the stimulus is removed. This is true for the vast majority of users, including long-term, heavy users. The process is uncomfortable, but it is temporary and well-documented. For those considering a reset, the tolerance break guide provides a structured approach to the process.
When to Seek Professional Help
If you recognize multiple DSM-5 criteria in your own use pattern, that recognition is valuable regardless of what you decide to do with it. You do not need to meet a certain threshold of suffering to deserve support.
Consider reaching out to a healthcare provider if you have tried to quit or cut back multiple times without success, if cannabis use is affecting your work or relationships, if you are using cannabis to manage anxiety, depression, PTSD, or another condition that could benefit from its own treatment, or if withdrawal symptoms are severe enough to interfere with daily functioning.
If you are experiencing thoughts of self-harm at any point, reach out immediately.
SAMHSA's National Helpline is free, confidential, and available 24 hours a day, 7 days a week: 1-800-662-4357. They can connect you with local treatment resources regardless of your insurance or financial situation.
The Honest Answer
The answer to "is weed addictive?" is not a satisfying yes or no. It is a conditional yes with important qualifiers. Cannabis can produce real, measurable, diagnosable dependence in approximately 9% of people who try it, 17% of those who start as teenagers, and roughly 47% of daily users experience withdrawal. The brain changes underlying this dependence are documented, the diagnostic criteria are established, and the prevalence is rising alongside potency.
Cannabis is also less likely to produce dependence than tobacco, alcohol, heroin, or cocaine. Withdrawal is self-limiting and not medically dangerous. Most users do not develop problems.
Both of these things are true at the same time. The science does not ask you to pick a side. It asks you to look clearly at what is happening in your own brain and your own life, and make decisions based on evidence rather than mythology in either direction.
The Bottom Line
The DSM-5 recognizes Cannabis Use Disorder as a diagnosable condition with 11 criteria and three severity levels. About 9% of people who try cannabis develop dependence, rising to 17% for adolescent-onset users. A 2020 meta-analysis found that 47% of regular users experience clinically significant withdrawal symptoms. The neuroscience is clear: chronic THC exposure causes CB1 receptor downregulation (confirmed by PET imaging), reduced endocannabinoid production, and altered dopamine signaling. CUD prevalence doubled between 2001 and 2013 as THC potency tripled. Cannabis has a lower dependence rate than tobacco, alcohol, or opioids, but the brain changes are real and measurable. The recovery evidence is equally clear: CB1 receptors begin normalizing within 2 days and return to baseline by approximately day 28.
Sources & References
- 1RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩
- 2RTHC-00159·Budney, Alan J. et al. (2004). “Yes, Cannabis Withdrawal Is Real. This 2004 Review Mapped What It Looks Like..” American Journal of Psychiatry.Study breakdown →PubMed →↩
- 3RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩
- 4RTHC-00975·Hasin, Deborah S. et al. (2015). “The Largest Study of Cannabis Addiction in America.” JAMA Psychiatry.Study breakdown →PubMed →↩
- 5RTHC-01144·ElSohly, Mahmoud A. et al. (2016). “U.S. Cannabis Potency Tripled Over Two Decades While CBD Nearly Vanished.” Biological Psychiatry.Study breakdown →PubMed →↩
- 6RTHC-00591·Meier, Madeline H. et al. (2012). “From Teen Years to 38: Heavy, Long-Term Cannabis Use Tracked With Lower Cognitive Scores.” Proceedings of the National Academy of Sciences (PNAS).Study breakdown →PubMed →↩
- 7RTHC-02010·Di Forti, Marta et al. (2019). “Daily High-Potency Cannabis Use and Psychosis Risk: The Largest European Study Drew a Direct Line.” The Lancet Psychiatry.Study breakdown →PubMed →↩
- 8RTHC-01134·D'Souza, Deepak Cyril et al. (2016). “Brain Cannabinoid Receptors Drop With Heavy Use, Then Rebound Within Days of Stopping.” Biological Psychiatry: Cognitive Neuroscience and Neuroimaging.Study breakdown →PubMed →↩
What the Research Shows
This section synthesizes 1,380 peer-reviewed studies on Cannabis Addiction. Stronger evidence means more consistency across study types.
Meta-analysis of 28+ twin studies found genetics explained 40-48% of cannabis initiation and 51-59% of problematic use, with environment more influential for initiation
Strong EvidenceA meta-analysis found cannabis use associated with 2
Strong EvidenceMeta-analysis of 37 studies found one-third of first-episode psychosis patients use cannabis, with regular use typically starting 6
Strong EvidenceWhere Scientists Disagree
Areas where research shows conflicting results or ongoing scientific debate.
Data from 120 subjects showed cannabis tolerance develops and fades quickly, while withdrawal symptoms including insomnia, irritability, and tremor appeared after as few as 7 days of use
Moderate EvidenceA 1992 review found that despite widespread human use, animals would not self-administer THC and evidence of brain reward pathway stimulation was minimal
Moderate EvidenceAmong New York young adults, early alcohol use (ages 13-16) was the strongest predictor of later marijuana and cigarette use, supporting an age-dependent gateway pattern
Moderate EvidenceAmong 1,481 heavy smokers trying to quit with nicotine patches, marijuana users had half the odds of success
Moderate EvidenceWhat We Still Don't Know
- Long-term prospective studies tracking outcomes over 5+ years are largely absent from the literature.
- Research on diverse populations (different ages, ethnicities, and medical backgrounds) remains limited.
Evidence Breakdown
Distribution of study types in this research area. Higher-tier evidence (meta-analyses, RCTs) provides stronger conclusions.
Research Timeline
How our understanding of this topic has evolved.
Pre-2000
14 studies published. Includes 1 strong-evidence studies.
2000–2009
69 studies published. Includes 4 RCTs, 5 strong-evidence studies.
2010–2014
156 studies published. Includes 1 meta-analyses, 15 RCTs, 10 strong-evidence studies.
2015–2019
320 studies published. Includes 7 meta-analyses, 23 RCTs, 42 strong-evidence studies.
2020–present
821 studies published. Includes 20 meta-analyses, 57 RCTs, 161 strong-evidence studies.