Physical vs Psychological Cannabis Dependence: What Science Actually Shows
Balanced Cannabis Science
9%
About 9 percent of people who try cannabis develop dependence, rising to 17 percent for teen-onset users, and withdrawal symptoms hit 47 percent of regular users, settling the question of whether cannabis is physically addictive.
Volkow et al., New England Journal of Medicine, 2014
Volkow et al., New England Journal of Medicine, 2014
View as imageIf you only read one thing
Cannabis creates both physical and psychological dependence, and the difference matters less than people think. Your brain physically adapts to THC by pulling receptors offline — that is why you build tolerance and feel withdrawal when you stop. About 47% of regular users get real withdrawal symptoms. At the same time, habit loops, emotional coping, and social identity keep you using even after the physical part fades. Both types are real, both happen in your brain, and both respond to proven strategies.
The single most common thing people say when they first realize they have a problem with cannabis is some version of: "But weed is not physically addictive, so this must all be in my head." That framing is decades out of date, and it causes real harm because it leads people to dismiss their own experience and delay seeking support. Cannabis produces measurable physical dependence, measurable psychological dependence, and a clinical diagnosis that encompasses both. The debate about which kind of addiction counts as "real" is a distraction from the more useful question, which is what to do about it.
Key Takeaways
- Cannabis creates both physical dependence (tolerance and withdrawal) and psychological dependence (habit, coping, identity) — and research backs up both
- The "physical vs psychological" distinction matters less than people think, because both happen in your brain and both respond to the same proven strategies
- About 9% of people who try cannabis develop dependence — rising to 17% for those who start as teens — according to a major review in the New England Journal of Medicine
- The DSM-5 does not even use the terms "physical" or "psychological" addiction — it defines Cannabis Use Disorder through 11 specific behavioral and functional criteria
- Withdrawal symptoms are real, clinically recognized, and hit about 47% of regular users, which settles the "is it physically addictive" question once and for all
- After physical withdrawal passes, psychological factors like habit loops, emotional coping, and social identity are what drive relapse — so behavioral strategies matter more for long-term success than managing acute symptoms alone
Where the "Not Physically Addictive" Idea Came From
For most of the twentieth century, addiction science used physical withdrawal symptoms as the primary marker of "real" dependence. Heroin caused vomiting and shaking when people stopped. Alcohol caused seizures. These dramatic physical symptoms made the physical dependence visible and undeniable. Because early cannabis researchers did not observe comparable physical collapse when heavy users stopped, the conclusion was that cannabis was not physically addictive.
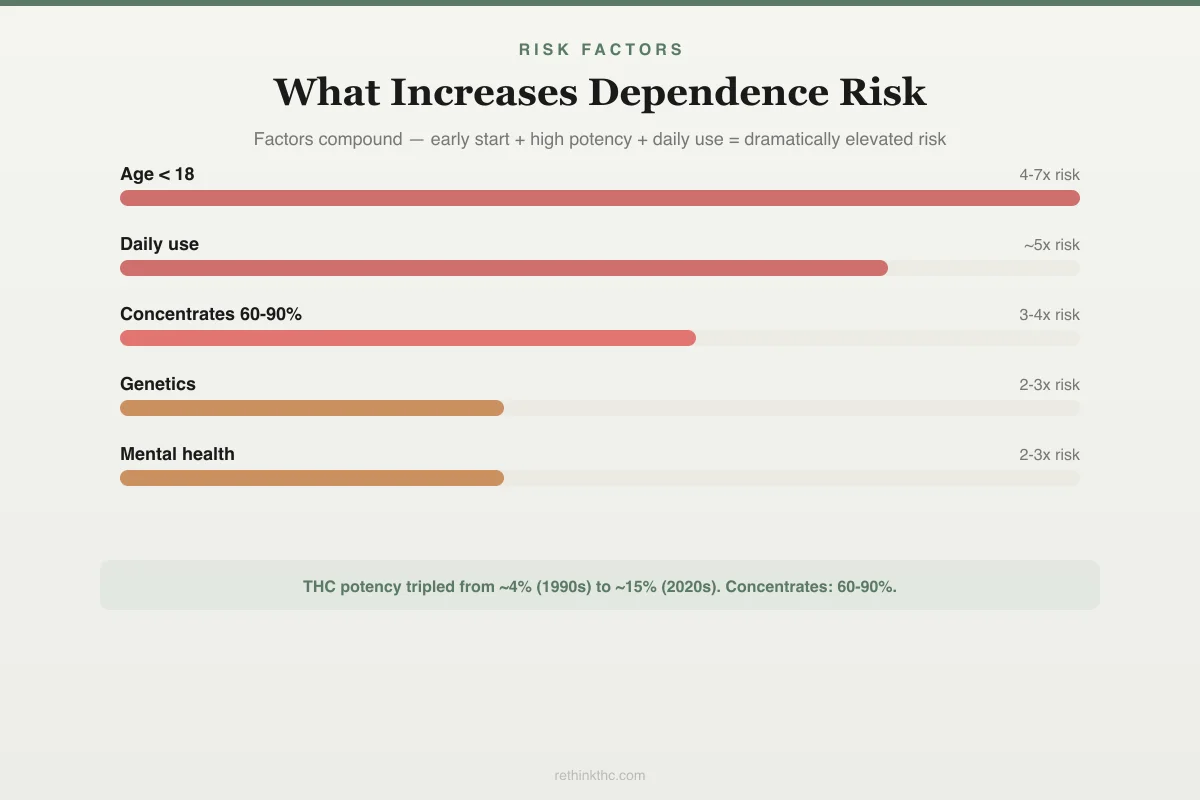
Risk Factors
What Increases Your Risk of Cannabis Dependence
These factors compound — early start + high potency + daily use = dramatically elevated risk.
Age of first use
Before 18
Frequency
Daily use
Potency
60-90% THC concentrates
Genetics
40-60% heritable
Mental health
Anxiety/depression/PTSD
Duration
Years of daily use
THC potency tripled from ~4% (1990s) to ~15% (2020s). Concentrates reach 60-90%. Higher potency = steeper risk curve.
This framework was always incomplete. It centered visible bodily symptoms while ignoring what was happening neurologically. As brain imaging technology improved and researchers could actually observe what happened to the brain during and after cannabis use, the picture changed substantially.
The other problem was that "psychological addiction" became shorthand for "not a real problem," implying that someone could simply decide to stop and the problem would disappear. This misunderstands how psychology works. Compulsive behavior patterns, emotional dependency, and habituated responses to stress are as grounded in brain biology as any physical symptom. The brain is the organ that drives all of it.
The Physical Dependence Evidence
Physical dependence has a specific scientific meaning: the body adapts to a substance such that removing it produces measurable physiological changes. By this definition, cannabis clearly produces physical dependence in regular users.
The primary mechanism is CB1 receptor downregulation. CB1 receptors are the docking stations in your brain where THC attaches to produce its effects. When you use cannabis regularly, your brain responds to the persistent activation of these receptors by reducing both the number of receptors available and their sensitivity. This is called downregulation, and it is a fundamental adaptive process your brain uses with many different substances, not just cannabis.
A study published in Biological Psychiatry[1] found that daily cannabis users show approximately 15% lower CB1 receptor availability compared to non-users, and that this reduction is measurable with brain imaging. CB1 receptor recovery begins within 2 days of stopping cannabis use. A 2012 study in Molecular Psychiatry[2] found that receptors normalize to baseline levels at around day 28 of abstinence.
That receptor adaptation is the physical basis for both tolerance (needing more cannabis to get the same effect, because your receptors are less responsive) and withdrawal (feeling worse than normal when you stop, because your natural endocannabinoid system is running below capacity). Both are textbook indicators of physical dependence.
Withdrawal symptoms from cannabis are now officially recognized in the DSM-5 as cannabis withdrawal syndrome. The recognized symptoms include irritability, anger, anxiety, sleep difficulty, decreased appetite, restlessness, and physical symptoms like headaches, sweating, and stomach pain. A 2003 study published in the Journal of Abnormal Psychology[3] documented that these symptoms typically begin within days 1 to 3 of stopping, peak between days 2 and 6, and largely resolve within 4 to 14 days for most users.
A 2020 meta-analysis in JAMA Network Open[4] analyzed data across multiple large studies and found that 47% of frequent cannabis users experience clinically significant withdrawal symptoms when they stop. Nearly one in two. This is not a fringe effect observed in laboratory conditions. It is what happens to roughly half of all regular users in the real world.
This body of evidence settles the question. Cannabis produces physical dependence by every meaningful scientific criterion.
The Psychological Dependence Evidence
Psychological dependence refers to the mental and behavioral components of dependence: compulsive use despite negative consequences, reliance on a substance to manage emotional states, deeply ingrained habit loops, and a sense of identity or social belonging organized around use.
Cannabis is well-documented to produce all of these.
Habit and automaticity. Repeated behaviors become automatic over time through a process of neural pathway strengthening. When you have smoked every evening after work for three years, that behavior pattern is wired into your brain's procedural memory (the system that runs automatic behaviors without conscious deliberation). The cue (getting home from work) triggers the craving and the behavior before conscious thought has a chance to intervene. This is not weakness. It is how habit formation works neurologically, and it applies to anything you do repeatedly in the same context.
Emotional coping dependence. THC suppresses activity in the amygdala (the brain region that processes stress, fear, and negative emotion), reduces cortisol (the primary stress hormone), and increases dopamine release (the neurotransmitter associated with reward and mood). For someone dealing with anxiety, trauma, chronic pain, or depression, these effects provide genuine short-term relief. The problem is that consistent external management of emotional states prevents the brain from developing and using its own regulatory capacities. People who have used cannabis to cope with stress for years often find that anxiety, irritability, and emotional dysregulation are severe during the first weeks after quitting, not only because of withdrawal but because the coping tool they relied on is gone.
This pattern is well-captured in discussions of self-medicating with weed. The emotional dependence component can be more difficult to address than the physical withdrawal because it requires developing alternative coping strategies, not just waiting out a biological timeline.
Identity and social context. For many heavy users, cannabis is woven into their social identity, daily rituals, friend group, and self-concept. Quitting can feel like a loss of social belonging and a disruption of personal identity, not just a behavioral change. This dimension of dependence has no physical symptom to point to, but it is no less real in its power to maintain use and to make quitting difficult.
Why the Distinction Matters Less Than People Think
The physical versus psychological framing creates a false hierarchy where physical dependence is treated as "serious" and psychological dependence is treated as "just mental." This has two practical consequences, both harmful.
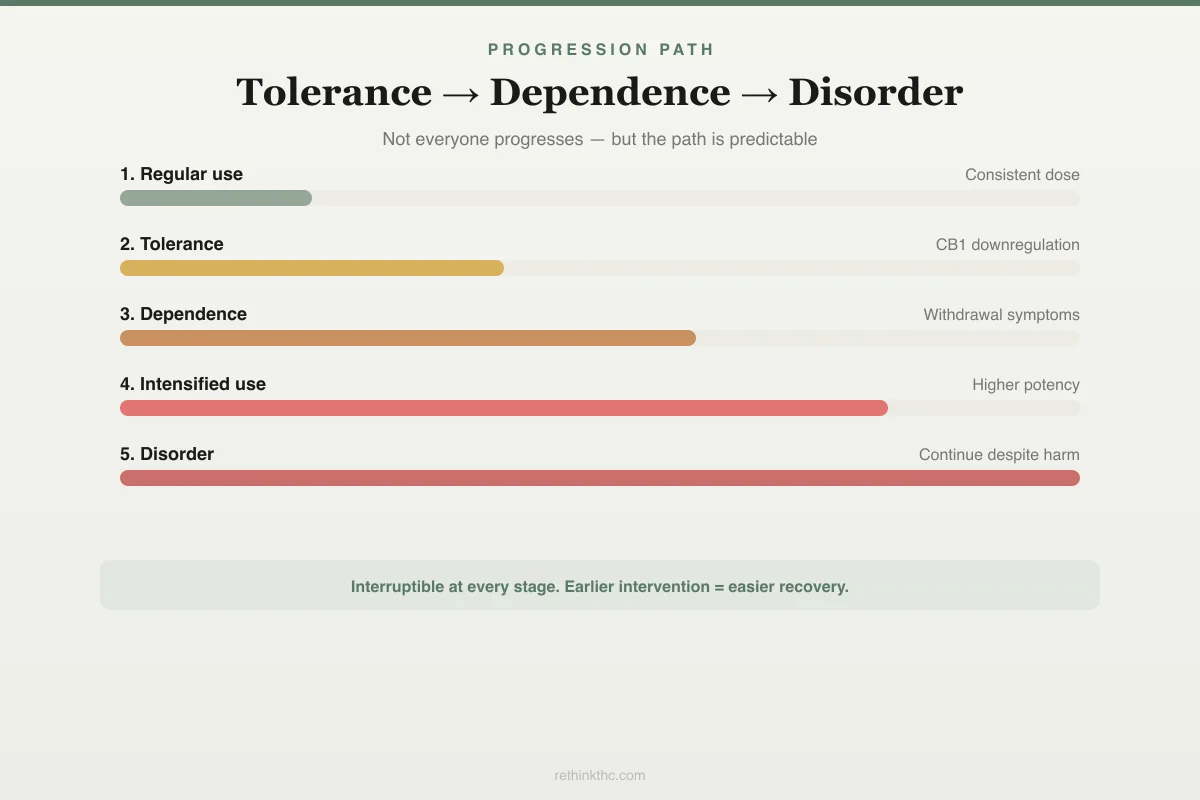
Progression Path
From Tolerance to Dependence to Disorder
Not everyone progresses — but when it happens, the path is predictable.
Regular use
Consistent dose and frequency, predictable effects
Tolerance develops
Need more to get same effect — CB1 receptors downregulate
Dependence emerges
Feel "off" on non-use days: irritability, sleep loss, appetite drop
Use intensifies
Switch to higher potency, more frequent sessions, larger amounts
Disorder criteria met
Continue despite problems, can't cut down, time spent recovering
The good news: this path is interruptible at every stage. Earlier intervention = easier recovery.
First, people who experience clear physical symptoms (withdrawal, tolerance) sometimes conclude they have a "real" addiction while people who experience primarily behavioral and emotional dependence conclude theirs is "just a habit" that should be easy to break. The second group often delays seeking support because they feel they do not qualify.
Second, even when people accept that psychological dependence is serious, the word "psychological" can imply that the solution is just willpower or attitude change. It is not. Psychological dependence is produced by specific changes in how your brain's reward circuitry, habit systems, and emotional regulation networks are wired. Changing those patterns requires behavioral and sometimes pharmacological interventions, exactly as physical dependence does.
Brain imaging research has repeatedly demonstrated that the cravings, compulsive urges, and reward system changes associated with substance dependence are measurable in the brain regardless of whether the substance is one that also produces dramatic physical withdrawal. The brain of someone with a strong psychological cannabis dependence does not look meaningfully different from the brain of someone with a physical one. Both show altered dopamine system function, altered prefrontal cortex (the brain's decision-making and impulse control center) activity, and modified reward pathway responses.
The is weed addictive question, which people debate endlessly, produces more clarity when you stop asking about category and start asking about consequences.
The DSM-5 Framework: Cannabis Use Disorder
Modern addiction medicine has largely moved past the physical versus psychological debate. The DSM-5 replaced both terms with a single diagnosis called Cannabis Use Disorder (CUD), which is defined by 11 criteria organized around behavioral patterns, functional impairment, and loss of control. You need to meet at least 2 of the 11 criteria within a 12-month period to qualify for the diagnosis.
The criteria include things like: using more cannabis than intended, spending a lot of time obtaining, using, or recovering from cannabis, giving up important activities because of cannabis, continuing to use despite knowing it is causing problems, experiencing cravings, and experiencing tolerance or withdrawal. Notice that tolerance and withdrawal are two of the eleven criteria, not the only two, and you do not need either one to meet the diagnostic threshold.
This framework captures the full spectrum of problematic cannabis use without requiring a checklist of dramatic physical symptoms. It also distinguishes between mild (2 to 3 criteria), moderate (4 to 5 criteria), and severe (6 or more criteria) CUD, which maps to the real-world variation in how disruptive cannabis dependence can be.
A 1994 study in Experimental and Clinical Psychopharmacology found that approximately 9% of people who ever use cannabis develop dependence. A 2014 review by Volkow and colleagues, published in the New England Journal of Medicine, confirmed that 9% figure for lifetime users, and found that the rate rises to 17% for those who begin using in adolescence. The higher adolescent rate is significant because the adolescent brain, specifically the prefrontal cortex and the endocannabinoid system, is still developing during the teenage years, making it more vulnerable to the long-term effects of regular THC exposure. The cannabis and the developing brain article covers that evidence in detail.
These numbers mean that the majority of people who try cannabis do not develop Cannabis Use Disorder. But 9% of all ever-users represents millions of people, and the adolescent risk rate of 17% is high enough to warrant serious consideration among young users.
What This Means for Quitting Strategies
Understanding that both physical and psychological components are real has direct implications for how you approach stopping.
The physical component (withdrawal) is time-limited and follows a predictable biological trajectory. Research establishes that the acute phase resolves for most people within two weeks, and receptor recovery is largely complete by day 28. The most useful tools during this phase are managing discomfort (sleep hygiene, exercise, nutrition), tracking progress to avoid the false perception that it is not improving, and having accurate expectations. Knowing that day four is typically the worst point helps you stay the course when you reach it.
The psychological component requires different tools. Habit patterns need to be interrupted and replaced, not just stopped. If you smoked every evening, the evening slot needs to be filled with something else, because leaving a behavioral void invites relapse. Coping functions that cannabis served need to be replaced with other strategies, whether that is exercise, therapy, social support, or structured relaxation practices. Identity and social dimensions, particularly if your friend group is built around cannabis use, may need more intentional work over a longer timeline.
For most people, the psychological component is what drives relapse after the physical withdrawal has passed. Research on cannabis relapse consistently shows that cravings triggered by environmental cues, stress, and social situations are the primary mechanisms, not ongoing physical symptoms. This is why strategies that address habit loops and coping patterns, like cognitive behavioral therapy, are among the most effective interventions for Cannabis Use Disorder.
The signs of cannabis use disorder article provides a closer look at the diagnostic criteria and how they show up in practice. If you are trying to cut back rather than quit entirely, how to cut back on weed covers that approach.
The Dependence Spectrum
One more concept worth understanding: dependence exists on a spectrum, not as a binary. You can be significantly dependent on cannabis without meeting the full DSM-5 diagnostic threshold for Cannabis Use Disorder. You can experience meaningful withdrawal without being a daily user. You can have strong psychological dependence and minimal physical withdrawal, or vice versa.
The spectrum framing is more useful than the categorical one because it allows for an honest assessment of where you actually are. Someone who smokes three to four times a week, notices they are irritable on days they do not use, and finds that cannabis occupies a lot of mental real estate, is experiencing dependence on the spectrum even if they do not identify as having a disorder. That still matters. It still affects their life. And it still responds to the same strategies.
Research using the Anthony 1994 criteria found that the 9% dependence rate includes people across a wide range of use patterns, not just daily heavy users. The risk is not exclusive to the most extreme cases.
When to Seek Professional Help
Cannabis Use Disorder is a recognized medical diagnosis, and there is no reason to navigate it without professional support if you want it. Cognitive behavioral therapy has the strongest evidence base for treating CUD, and many therapists specialize in exactly this. A therapist experienced with substance use can help you understand your specific pattern of dependence, develop coping tools for the psychological components, and work through any underlying conditions (anxiety, depression, trauma) that were being managed with cannabis.
If withdrawal symptoms are severe enough to interfere with work, sleep, or relationships, a healthcare provider can discuss short-term interventions. There is no FDA-approved medication specifically for Cannabis Use Disorder, but some medications can address specific withdrawal symptoms like insomnia or anxiety while the acute phase passes.
SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day, 7 days a week. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
The Bottom Line
Cannabis produces both physical dependence (CB1 receptor downregulation causing tolerance and withdrawal) and psychological dependence (habit formation, emotional coping, identity integration). The distinction matters less than most people think because both are brain-based processes. About 9% of people who ever try cannabis develop dependence, rising to 17% for adolescent-onset users. The DSM-5 replaced the physical/psychological categories with Cannabis Use Disorder, defined by 11 behavioral and functional criteria. Withdrawal affects approximately 47% of regular users, with symptoms beginning days 1 to 3, peaking days 2 to 6, and resolving within 2 to 4 weeks. CB1 receptors normalize by around day 28 of abstinence. Psychological dependence typically drives relapse after physical withdrawal resolves, making behavioral strategies and therapy critical for long-term success.
Sources & References
- 1RTHC-01134·D'Souza, Deepak Cyril et al. (2016). “Brain Cannabinoid Receptors Drop With Heavy Use, Then Rebound Within Days of Stopping.” Biological Psychiatry: Cognitive Neuroscience and Neuroimaging.Study breakdown →PubMed →↩
- 2RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩
- 3RTHC-00134·Budney, Alan J. et al. (2003). “When Heavy Users Quit Cannabis, Symptoms Show Up Fast and Ease Within Two Weeks.” Journal of Abnormal Psychology.Study breakdown →PubMed →↩
- 4RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩