Self-Medicating with Weed: Why It Works Until It Doesn't

Withdrawal & Recovery
4–6 Weeks
Withdrawal symptoms often look identical to the condition you were self-medicating. A 4 to 6 week abstinence period is the most reliable way to separate withdrawal from what was there before cannabis.
Budney et al., 2003; Bahji et al., JAMA Network Open, 2020
Budney et al., 2003; Bahji et al., JAMA Network Open, 2020
View as imageIf you only read one thing
Self-medicating with weed works at first because cannabis genuinely changes the brain chemicals behind anxiety, depression, insomnia, and pain. The problem is your brain adapts, so you need more over time, and the real issue underneath never gets treated. When you try to quit, withdrawal feels exactly like the thing you were medicating — which tricks you into thinking you can't cope without it. A 4 to 6 week break is the only reliable way to figure out what's actually you versus what's withdrawal.
Nobody wakes up one morning and decides to become dependent on cannabis. What usually happens is quieter than that. You are dealing with something, anxiety that will not let you sleep, depression that flattens every day into the same grey blur, chronic pain that eats into everything, and you find something that actually helps. It works. So you keep using it. That is not a moral failure. It is a completely rational response to suffering. The problem is what happens next.
This article is about the pattern that develops when cannabis becomes the primary way you manage a condition that existed before you ever lit up. It is not anti-weed. It is about understanding a cycle that traps a lot of people without them realizing how it happened.
Key Takeaways
- Self-medicating means using a substance to manage symptoms of a condition that is undiagnosed, untreated, or undertreated
- Cannabis genuinely affects the brain systems behind anxiety, depression, insomnia, PTSD, chronic pain, and ADHD — which is why it works in the short term
- Tolerance forces you to use more over time, and the real condition underneath goes untreated while THC covers it up
- Withdrawal symptoms often look just like the original condition, so it is nearly impossible to tell what is "you" versus what is withdrawal without 4 to 6 weeks off
- This is not about whether cannabis is good or bad — it is about the difference between managed medical use and unmanaged self-medication
- A 4 to 6 week break is the most reliable way to figure out which symptoms are withdrawal and which point to a real underlying condition
What Self-Medication Actually Means
Self-medication is using a substance to manage symptoms of a condition that has not been formally diagnosed or is not being adequately treated. The term comes from Edward Khantzian, a psychiatrist at Harvard, who first articulated the self-medication hypothesis in the 1980s. Khantzian proposed that people do not use substances randomly. They are drawn to specific substances that address specific forms of internal distress. A person with social anxiety gravitates toward alcohol. A person with undiagnosed ADHD gravitates toward stimulants. And a person with anxiety, insomnia, or emotional dysregulation gravitates toward cannabis.
Here is how the self-medication cycle works — and where it closes into a trap.
Cannabis & Mental Health
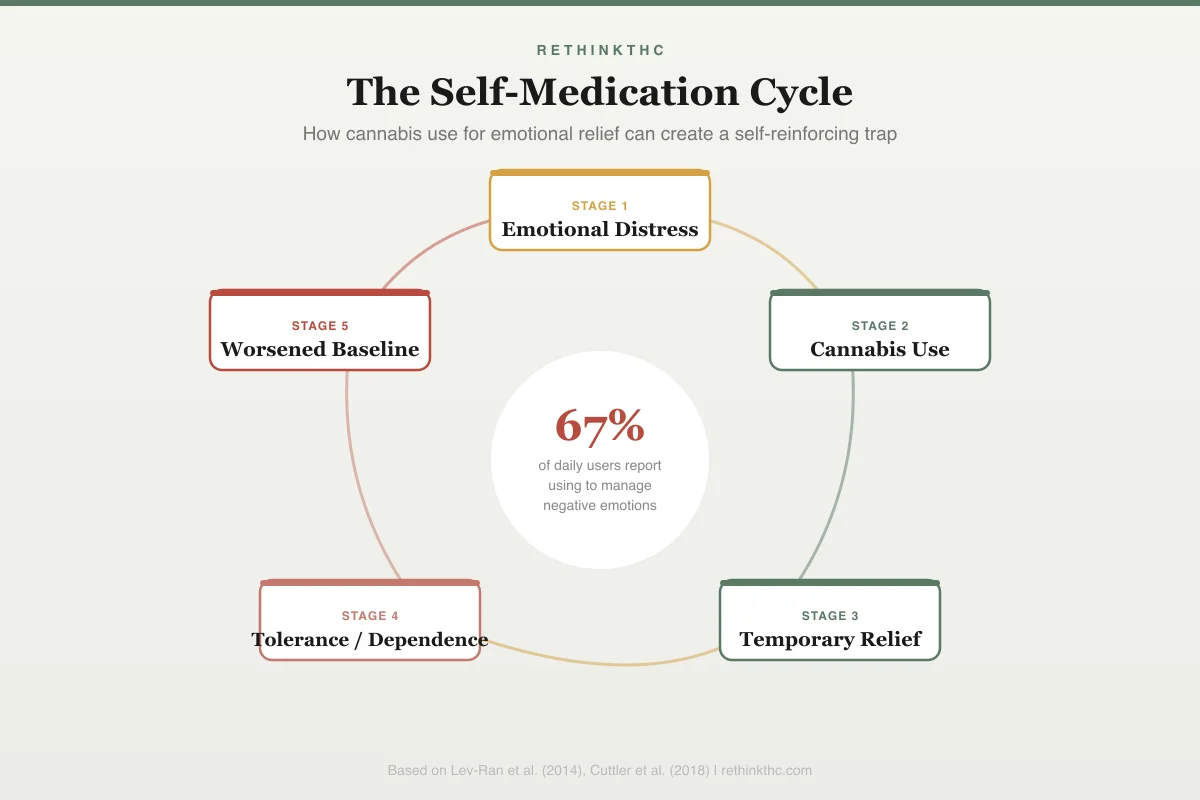
The Self-Medication Cycle
67%
of daily users report using cannabis
to manage negative emotions
Emotional Distress
Anxiety, depression, stress, or trauma symptoms surface
Cannabis Use
Reach for cannabis to cope with difficult feelings
Temporary Relief
Symptoms subside briefly, reinforcing the behavior
Tolerance / Dependence
Need more to achieve the same relief; withdrawal when stopping
Worsened Baseline
Underlying symptoms return worse than before use began
This is not weakness. It is pattern recognition. You found something that relieved your symptoms, and your brain filed that information under "solutions that work." The fact that it was a substance rather than a prescription or a therapy session does not change the logic behind it. Your brain does not distinguish between sources of relief. It just knows what makes the pain stop.
The Conditions People Most Commonly Self-Medicate With Cannabis
Cannabis is not a random coping tool. It affects very specific neurotransmitter systems, which is why certain conditions drive self-medication more than others.
| Condition | Why Cannabis Feels Helpful | The Trap | Withdrawal Mimics |
|---|---|---|---|
| Anxiety | Dampens amygdala; boosts GABA | Rebound anxiety exceeds original levels | Anxiety peaks days 3–10 |
| Depression | Triggers dopamine in reward pathway | Anhedonia worsens with chronic use | Flat mood, emptiness for weeks |
| Insomnia | Suppresses REM; shortens sleep latency | Sleep architecture degrades over time | Severe insomnia for 2–6 weeks |
| PTSD | Reduces nightmares and hypervigilance | Trauma processing stalls | Nightmares return; hyperarousal spikes |
| Chronic pain | Activates CB1 pain modulation | Tolerance requires dose escalation | Pain sensitivity may temporarily increase |
| ADHD | Raises dopamine; quiets mental noise | Masks ADHD while worsening long-term dopamine | Focus problems amplified in withdrawal |
Anxiety. THC dampens the amygdala and boosts GABA, your brain's primary calming neurotransmitter. A 2009 review by Crippa and colleagues documented the complex relationship between cannabis and anxiety, noting that low doses reduce anxiety while higher doses and chronic use can worsen it.[2] For someone with generalized anxiety or social anxiety, this feels like the volume on their internal alarm system has been turned down. The relief is real and immediate. A detailed breakdown of this mechanism is covered in weed withdrawal anxiety.
Depression. Cannabis triggers dopamine release in the reward pathway, which temporarily counters the flat, anhedonic feeling of depression. When nothing else feels good, THC can provide a window of something resembling pleasure or engagement. The challenge of quitting weed with depression is that withdrawal-driven anhedonia can be nearly indistinguishable from the depression itself.
Insomnia. THC suppresses REM sleep and shortens sleep latency, meaning you fall asleep faster.[8] For someone who lies awake for hours with a racing mind, this is transformative. The tradeoff in sleep architecture shows up later.
PTSD. Cannabis can reduce nightmares and dampen the hypervigilance that defines PTSD. A 2017 review by Steenkamp and colleagues examined the evidence for cannabis as a PTSD treatment and found that while some cannabinoids showed promise, the evidence base remained insufficient for clinical recommendation.[3] The full picture of how weed interacts with PTSD is more complicated than the short-term relief suggests, and quitting weed with PTSD requires specific strategies because withdrawal can temporarily amplify trauma responses. For people whose cannabis use traces back to early life experiences, the relationship between childhood trauma, adverse childhood experiences, and cannabis use adds another layer to the self-medication pattern.
Chronic pain. The endocannabinoid system is directly involved in pain modulation. THC activates CB1 receptors that reduce pain signal transmission. For people with conditions that cause persistent pain, cannabis can be more tolerable than opioids and more effective than over-the-counter options.
ADHD. Some people with undiagnosed ADHD report that cannabis helps them slow down, focus, or quiet the noise in their head. The relationship between quitting weed and ADHD is complex because the symptoms overlap in ways that make it hard to separate one from the other.
OCD. Cannabis can temporarily quiet intrusive thoughts by dampening the anxiety that drives compulsive loops. But the relief masks the OCD rather than treating it, and withdrawal often intensifies the intrusive thought patterns. The relationship between weed and OCD intrusive thoughts explains why this particular form of self-medication tends to backfire.
A 2013 study by Lev-Ran and colleagues, published in Comprehensive Psychiatry, found significant associations between cannabis use and anxiety, depression, and other mental health conditions.[1] The study noted that while the direction of causality was complex, the pattern of cannabis use increasing alongside mental health symptoms was consistent across populations.
Why It Works in the Short Term
The reason self-medication with cannabis is so common is that it genuinely works at first. THC is not a placebo. It produces real, measurable changes in the brain systems that drive anxiety, pain, insomnia, and mood regulation. When you smoke and your anxiety drops within minutes, that is a chemical event. Your amygdala is being dampened. Your GABA levels are being boosted. Your cortisol response is being blunted.[2]
This is also why dismissing self-medication as "just getting high" misses the point entirely. Many people who self-medicate do not particularly enjoy being stoned. They are chasing the absence of symptoms, not the presence of euphoria. The high is a side effect. The relief is the goal.
Why It Becomes a Trap
The problem with self-medication is not that it does not work. It is that it works just well enough to prevent you from solving the actual problem while gradually creating new ones.
Tolerance Erodes the Relief
Your brain adapts to the presence of THC by downregulating CB1 receptors and adjusting GABA and glutamate production.[6][7] The dose that worked three months ago no longer produces the same relief. So you increase the dose, switch to concentrates, or use more frequently. This is not a willpower issue. It is basic neurobiology. Your brain is recalibrating around the chemical you keep introducing, which is the same process that drives cannabis withdrawal when you eventually stop. If you recognize this escalation pattern, the is weed addictive article examines the spectrum of dependence in detail.
The Underlying Condition Goes Untreated
While THC manages the symptoms, the condition itself continues unchecked. Anxiety disorders do not resolve because you suppress the symptoms. Depression does not lift because you override the anhedonia with dopamine hits. ADHD does not improve because you quiet the noise for a few hours. In some cases, prolonged heavy use can even trigger new problems, including cannabis-induced psychosis in people with genetic vulnerability. In many cases, the condition worsens over time because it is not receiving the specific treatment it needs, whether that is therapy, medication, lifestyle changes, or a combination.
Withdrawal Mimics the Original Condition
This is where the trap gets truly difficult. When you stop using cannabis, withdrawal produces symptoms that look almost identical to the conditions you were self-medicating in the first place. Anxiety. Depression. Insomnia. Irritability. Difficulty concentrating. Approximately 47 percent of regular cannabis users experience clinically significant withdrawal symptoms when they stop.[5] If you were using weed for anxiety and then experience intense anxiety when you quit, your brain draws the obvious but potentially wrong conclusion: "I need cannabis to function."
This creates a cycle that can feel impossible to escape. You quit, the symptoms return, you interpret them as proof that you need cannabis, and you go back to using. Each cycle reinforces the belief that cannabis is a medical necessity rather than a temporary bandage.
The Diagnostic Confusion Problem
This is the part that does not get enough attention. Self-medication with cannabis creates a fog around diagnosis that makes it genuinely difficult for you or a professional to know what you are dealing with.
The visual below maps how common conditions overlap with both cannabis effects and withdrawal symptoms — which is why telling them apart without a sustained break is so difficult.
Self-Medication Matrix
Conditions Commonly Self-Medicated With Cannabis
| Condition | Short-Term Relief | Long-Term Evidence | Withdrawal Overlap | Diagnostic Confusion |
|---|---|---|---|---|
| Anxiety | Yes | Weak | High | High |
| Depression | Partial | Weak | High | High |
| Insomnia | Yes | Weak | High | Medium |
| PTSD | Yes | Moderate | Medium | Medium |
| Chronic Pain | Yes | Moderate | Low | Low |
| ADHD | Partial | None | Medium | High |
Anxiety
Short-term
YesLong-term
WeakWithdrawal
HighDx Confusion
HighDepression
Short-term
PartialLong-term
WeakWithdrawal
HighDx Confusion
HighInsomnia
Short-term
YesLong-term
WeakWithdrawal
HighDx Confusion
MediumPTSD
Short-term
YesLong-term
ModerateWithdrawal
MediumDx Confusion
MediumChronic Pain
Short-term
YesLong-term
ModerateWithdrawal
LowDx Confusion
LowADHD
Short-term
PartialLong-term
NoneWithdrawal
MediumDx Confusion
High
Consider someone who has been using cannabis daily for three years to manage what they believe is anxiety. Is the anxiety a standalone disorder that existed before cannabis use? Is it partially caused by chronic cannabis use itself? Is it a withdrawal symptom that resolves after a few weeks? Or is it some combination of all three?
While you are actively using, these questions are nearly impossible to answer. THC is constantly modulating the same systems that the underlying condition affects. It is like trying to diagnose a hearing problem while someone is playing loud music. You cannot get a clear signal.
The 4 to 6 Week Test
The most reliable way to distinguish withdrawal from an underlying condition is time. Withdrawal symptoms follow a predictable timeline. Acute symptoms typically peak in the first week or two and resolve significantly by weeks 3 to 4.[4] Lingering symptoms like mood instability and sleep disruption generally normalize by weeks 4 to 6.
If the symptoms you were self-medicating resolve within that window, they were likely withdrawal-driven or at least significantly amplified by cannabis use. If they persist at meaningful intensity beyond 6 weeks with no improvement, there is probably an underlying condition that needs its own treatment.
This is not a DIY diagnostic tool. It is a framework that helps you and a healthcare provider separate the layers of what is happening. But it requires a period of sustained abstinence, which is exactly the thing that self-medication makes feel unbearable. That is the core difficulty.
Getting the Right Help
If you recognize yourself in this article, the path forward involves a few key steps.
Talk to a doctor or therapist before you quit. If you are self-medicating a real condition, stopping cold turkey without a plan can be unnecessarily brutal. A provider can help you taper if needed, offer temporary support for the acute withdrawal phase, and begin assessing what the underlying condition actually is. If access to in-person care is a barrier, online therapy options for cannabis-related anxiety can be a practical starting point.
Name what you are treating. Get specific about which symptoms cannabis manages for you. Anxiety? Insomnia? Pain? Difficulty focusing? The more precise you can be, the more targeted the treatment plan can be. Many of the conditions people self-medicate with cannabis have effective, evidence-based treatments that do not carry the tolerance and withdrawal issues.
Be honest about the full picture. If a healthcare provider does not know you have been using cannabis daily, they cannot accurately diagnose you. Cannabis use affects nearly every mental health screening tool. Full disclosure leads to better care.
Expect discomfort and plan for it. The withdrawal period is genuinely difficult, especially when your symptoms overlap with a pre-existing condition. Having a plan for how to quit weed that accounts for your specific situation makes the process more manageable. Understanding the dopamine recovery timeline can also help you anticipate the emotional flatness that often follows quitting and recognize it as temporary neurochemistry rather than permanent depression.
Be patient with the diagnostic process. It may take several weeks after quitting before a provider can give you a clear picture of what you are dealing with. This is frustrating, but it is honest. Diagnosing through the noise of withdrawal is imprecise. Waiting until the withdrawal clears produces better answers.
A Note on Prescribed Medical Cannabis
This article is about unmanaged self-medication, not about prescribed medical cannabis used under professional supervision for specific conditions. People with certain chronic pain conditions, treatment-resistant epilepsy, or chemotherapy-related symptoms may have legitimate, monitored medical use. The distinction is not recreational versus medical. The distinction is between a managed treatment plan with professional oversight and a pattern of self-directed use that prevents you from addressing the root cause of your symptoms.
When to Seek Professional Help
If you have been self-medicating with cannabis and want to stop, professional support can make a significant difference. This is especially true if you have a history of mental health conditions, if your daily use is heavy, or if previous attempts to quit have been derailed by the return of symptoms.
Safety
ModerateDon't quit alone if you have a serious mental health condition
Concern
If cannabis has been your primary way of managing severe anxiety, depression, PTSD, or any condition involving suicidal thoughts, stopping abruptly without professional support can make those symptoms temporarily much worse during the withdrawal window.
What the research says
This is not a reason to keep self-medicating forever. It is a reason to involve a doctor or therapist before you quit, so they can provide temporary support, monitor your symptoms, and step in if withdrawal unmasks something that needs immediate treatment.
Particularly relevant for: Anyone self-medicating a diagnosed or suspected mental health condition with daily cannabis
What to do
Talk to a doctor or therapist before quitting. If you experience severe depression or thoughts of self-harm at any point, contact SAMHSA at 1-800-662-4357 or text HELLO to 741741 immediately.
Clinical guidance based on Budney et al. (2003), Bahji et al. (2020)
Seek help immediately if you experience severe depression, panic, or thoughts of self-harm during weed withdrawal or at any point in the process. If you are part of the LGBTQ+ community navigating cannabis use and recovery, identity-affirming support resources can make a meaningful difference in the process. SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
The Reframe
Self-medication is not a character flaw. It is what happens when real symptoms meet an accessible solution in the absence of better options. The problem is not that you found something that helped. The problem is that it stopped helping the way it used to, and now it is standing between you and the treatment that could actually resolve what you have been carrying.
Stepping away from cannabis when it has been your primary coping tool is one of the hardest things you can do. It means sitting with the unmanaged version of whatever you were medicating, at least temporarily, while you and a provider figure out what it actually is. That takes courage, not weakness. And the clarity that comes out the other side, knowing what is actually yours to deal with versus what was withdrawal, versus what was a side effect of chronic use, is worth the discomfort it takes to get there.
The Bottom Line
Self-medicating with cannabis is not a moral failure — it is a rational response to real symptoms when better options are unavailable or unknown. THC genuinely affects the brain systems involved in anxiety, depression, insomnia, PTSD, chronic pain, and ADHD, which is why it works in the short term. The trap forms when tolerance erodes the relief, forcing dose escalation while the underlying condition goes untreated. Withdrawal then mimics the original condition, creating a cycle where quitting feels like proof that cannabis is medically necessary. A sustained abstinence period of 4 to 6 weeks is the most reliable way to separate withdrawal from a genuine underlying condition that needs its own treatment.
Sources & References
- 1RTHC-00698·Lev-Ran, Shaul et al. (2013). “Most Cannabis Use Came From People With Recent Mental Illness in a Large U.S. Survey.” Comprehensive Psychiatry.Study breakdown →PubMed →↩
- 2RTHC-00349·Crippa, Jose Alexandre S. et al. (2009). “Cannabis both calms and panics — the biphasic dose-response explains why the same drug produces opposite anxiety effects.” Human Psychopharmacology: Clinical and Experimental.Study breakdown →PubMed →↩
- 3RTHC-01528·Steenkamp, Maria M. et al. (2017). “Cannabis for PTSD: Promising Biology, Very Little Proof It Actually Works as Treatment.” Depression and Anxiety.Study breakdown →PubMed →↩
- 4RTHC-00134·Budney, Alan J. et al. (2003). “When Heavy Users Quit Cannabis, Symptoms Show Up Fast and Ease Within Two Weeks.” Journal of Abnormal Psychology.Study breakdown →PubMed →↩
- 5RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩
- 6RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩
- 7RTHC-01338·Bonnet, Udo et al. (2017). “Comprehensive review of cannabis withdrawal: symptoms, brain mechanisms, gender differences, and treatment options.” Substance abuse and rehabilitation.Study breakdown →PubMed →↩
- 8RTHC-01161·Gates, Peter et al. (2016). “Systematic Review Confirms Cannabis Withdrawal Disrupts Sleep, but Specific Mechanisms Remain Unclear.” Substance abuse.Study breakdown →PubMed →↩