Cannabis-Induced Psychosis: What It Is, Who's at Risk, and What to Do
Mental Health Deep
5x Risk
Daily use of high-potency cannabis was linked to five times the odds of a first psychotic episode, and roughly 18% of cannabis-induced psychosis cases progress to a longer-term psychotic disorder.
Di Forti et al., The Lancet Psychiatry, 2019
Di Forti et al., The Lancet Psychiatry, 2019
View as imageIf you only read one thing
Cannabis-induced psychosis is rare but real — and it's becoming more common as THC potency rises. Daily use of high-potency weed (above 10% THC) carries about 5 times the odds of a first psychotic episode. Most episodes are temporary and clear up within days to weeks. But about 18% of cases lead to a longer-term psychotic disorder, usually in people who already had the genetic wiring for it. Your biggest risk factors are family history, high-potency products, daily use, and being under 25.
Cannabis-induced psychosis is one of the most alarming things that can happen during or after cannabis use. It goes far beyond feeling paranoid or anxious while high. During a psychotic episode, a person loses contact with reality. They may see or hear things that are not there, believe things that have no basis in fact, or become so confused that their thinking and speech stop making sense to the people around them. It is uncommon, but it is real, and the rising potency of modern cannabis products has made it more visible in emergency rooms across the country.
Understanding what cannabis-induced psychosis actually is, who is most vulnerable, and what to do if it happens is important whether you use cannabis yourself or care about someone who does. This is not about fear. It is about having the information you need to make informed decisions.
Key Takeaways
- Cannabis-induced psychosis is a short break from reality — hallucinations, delusions, or complete disconnection — that goes far beyond normal paranoia or anxiety while high
- ER visits tied to cannabis psychosis have jumped sharply since legalization, which is why rising THC potency is at the center of this conversation
- Your genes play a big role — variations in the COMT and AKT1 genes and a family history of psychotic disorders can make you significantly more vulnerable
- Most cannabis-induced psychotic episodes are temporary and clear up within days to weeks, but for roughly 18 percent of people the episode uncovers or kicks off a longer-term psychotic disorder
- Only a small number of cannabis users ever experience this, but the consequences are serious enough that knowing the risk factors matters
- Di Forti et al. (2019, The Lancet Psychiatry) found that daily use of high-potency cannabis (THC above 10%) was linked to about five times the odds of a first psychotic episode compared to people who never used
What Cannabis-Induced Psychosis Actually Looks Like
Psychosis is a clinical term for a break from reality. It is not a personality flaw or a sign of weakness. It is a disruption in how the brain processes and interprets information. In cannabis-induced psychosis, this disruption is triggered by cannabis use, typically during intoxication or shortly after.
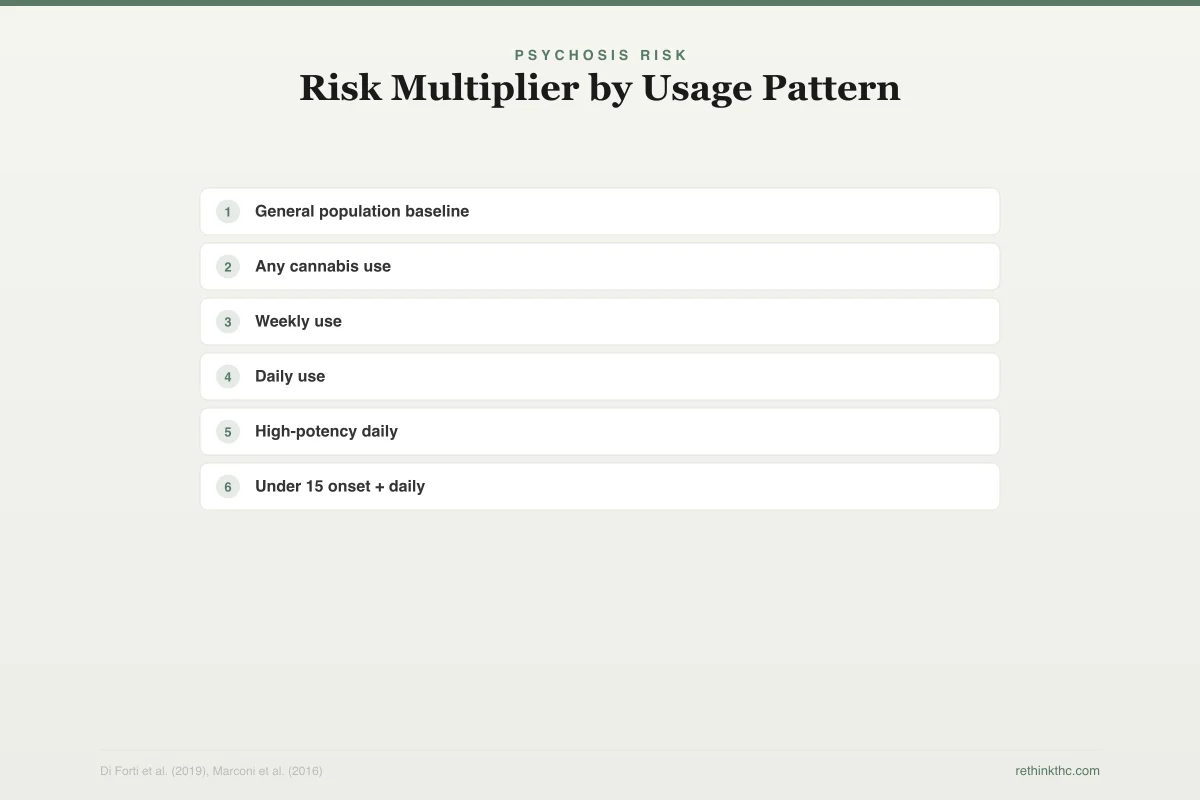
Psychosis Risk
Risk Multiplier by Usage Pattern
Relative risk of first psychotic episode vs. non-users
General population baseline
1x
Any cannabis use
1.4x
Weekly use
2x
Daily use
3.2x
High-potency daily
4.8x
Under 15 onset + daily
5x+
Absolute risk remains low: ~3% of daily users vs. ~0.7% baseline. Higher relative risk does not mean most users will develop psychosis.
The symptoms fall into a few categories.
Hallucinations. Seeing, hearing, or feeling things that are not present. Auditory hallucinations, hearing voices or sounds that nobody else hears, are the most common type in cannabis-related psychotic episodes.
Delusions. Strongly held beliefs that are clearly disconnected from reality. These can include paranoid delusions (believing someone is following you or plotting against you), grandiose delusions (believing you have special powers), or referential delusions (believing that unrelated events, such as a song on the radio, contain personal messages directed at you).
Disorganized thinking. Thoughts become fragmented and difficult to follow. Speech may jump between unrelated topics, trail off mid-sentence, or become incoherent. The person may struggle to answer simple questions or follow a basic conversation.
Loss of insight. This is the defining feature that separates psychosis from intense anxiety or paranoia. During a psychotic episode, the person typically does not recognize that their perceptions are distorted. They believe fully in what they are experiencing. If you have ever felt paranoid while high but knew on some level that the paranoia was the weed talking, that is not psychosis. Psychosis is when that awareness disappears.
These episodes can last hours to days. In most cases of purely cannabis-induced psychosis, the symptoms resolve as the drug clears the body and the brain stabilizes. But during the episode, the experience is genuinely frightening for the person and for anyone around them.
The ER Data: This Is Increasing
One of the clearest signals that cannabis-induced psychosis is a growing clinical concern comes from emergency department data in states that legalized recreational cannabis early.
A 2019 study by Monte and colleagues, published in the Annals of Internal Medicine, examined[1] cannabis-related emergency department visits in Colorado between 2012 and 2016. They found that visits involving psychotic symptoms or acute psychiatric disturbance increased significantly after legalization, with high-potency edibles and concentrates disproportionately represented.
A broader analysis published by Myran and colleagues in JAMA Network Open examined data from Ontario, Canada, following legalization there. They found a notable increase in cannabis-related emergency visits involving psychosis, particularly among males between 18 and 44.
Di Forti and colleagues published a landmark 2019 study in The Lancet Psychiatry examining[2] cannabis use and psychotic disorders across 11 sites in Europe and Brazil. They found that daily use of high-potency cannabis (THC above 10%) was associated with approximately five times the odds of experiencing a first psychotic episode compared to people who had never used cannabis. In cities where high-potency cannabis dominated the market, such as London and Amsterdam, the population-attributable fraction was significant, meaning a meaningful percentage of first-episode psychosis cases could be statistically linked to high-potency cannabis use.
These are not small or speculative findings. They point to a consistent pattern: as THC potency rises and access expands, psychosis-related events increase at the population level.
Why THC Potency Is Central to This Risk
The connection between higher-potency cannabis and psychosis risk is not incidental. It runs through specific neurological pathways.
THC acts primarily on CB1 receptors in the brain. These receptors are concentrated in areas involved in perception, cognition, and emotional regulation, including the prefrontal cortex, hippocampus, and amygdala. At typical doses, THC produces the familiar effects of euphoria, altered perception, and relaxation. But at high doses, THC can overwhelm the system. The prefrontal cortex, which is responsible for logical reasoning and reality testing, becomes disrupted. Dopamine signaling in the mesolimbic pathway (the reward and motivation circuit) surges in ways that mirror what happens in primary psychotic disorders like schizophrenia.
Murray and colleagues, writing in a 2016 review in World Psychiatry, summarized the dose-response relationship clearly: the higher the THC dose and the more frequent the exposure, the greater the risk of psychotic symptoms. This is consistent across observational studies, clinical case reports, and controlled laboratory experiments where THC was administered to healthy volunteers.
The products most associated with psychotic episodes in clinical reports are concentrates (dabs, wax, and high-potency vape cartridges reaching 60 to 95% THC) and edibles (where dosing errors are common and the onset is delayed, leading people to consume more than intended). These products deliver THC loads that far exceed what the brain encounters from moderate-potency flower.
Genetic Vulnerability: Why It Happens to Some and Not Others
Most people who use high-potency cannabis do not develop psychosis. The question of why some individuals are vulnerable while others are not leads directly to genetics.
Two genes have received the most research attention.
COMT (catechol-O-methyltransferase). This gene produces an enzyme that breaks down dopamine in the prefrontal cortex. People with a specific variation of this gene, the Val/Val variant, metabolize dopamine more slowly. When THC triggers a dopamine surge, these individuals clear it less efficiently, which means the prefrontal cortex is disrupted for longer and more severely. Caspi and colleagues' 2005 study in Biological Psychiatry found that cannabis users with the Val/Val COMT genotype were significantly more likely to develop psychotic symptoms than those with other variants.
AKT1. This gene is involved in dopamine signaling downstream of the initial receptor activation. A 2012 study by Di Forti and colleagues, published in Biological Psychiatry, found that cannabis users carrying a specific AKT1 variant (the C/C genotype) had approximately twice the risk of developing a psychotic disorder compared to carriers of other variants. The risk increased further with daily use.
Beyond specific genes, family history is the most accessible risk indicator. If you have a first-degree relative (parent or sibling) with schizophrenia, schizoaffective disorder, or another psychotic disorder, your baseline vulnerability to psychosis is elevated. Cannabis use, particularly heavy or high-potency use, can act as an environmental trigger on top of that existing vulnerability.
The science here is not saying cannabis "causes" schizophrenia. It is saying that for people with a genetic predisposition, cannabis can act as the match that lights a fire the kindling was already set for. For people without that predisposition, the same match falls on bare ground.
Safety
CriticalKnow your family history
Concern
If a parent or sibling has schizophrenia, schizoaffective disorder, or another psychotic disorder, your genetic vulnerability to cannabis-induced psychosis is significantly elevated. The AKT1 C/C genotype alone doubles the risk; combined with daily use, the odds multiply further.
What the research says
Family history is the most accessible screening tool. You don't need genetic testing — just knowing whether psychotic disorders run in your family is the single most important piece of information for assessing your personal risk.
Particularly relevant for: Anyone with a first-degree relative (parent, sibling) with a psychotic disorder
What to do
If you have a family history of psychotic disorders, avoid high-potency cannabis products entirely. If you choose to use, lower-potency flower with lower frequency is a meaningful harm reduction step. Any psychotic symptoms — even brief ones — warrant immediate medical evaluation.
Caspi et al. (2005), Di Forti et al. (2012, 2019)
Temporary Episode vs. Unmasking a Longer-Term Condition
This distinction matters enormously, and it is one of the most anxiety-producing questions people face after a psychotic episode.
Cannabis-induced psychosis in the strict clinical sense is a temporary event. The psychotic symptoms emerge during or shortly after cannabis use and resolve, usually within days to a few weeks, once the cannabis clears and the brain stabilizes. The person returns to their baseline mental functioning. This is what happens in the majority of cases.
However, a significant minority of people who experience a cannabis-induced psychotic episode go on to receive a diagnosis of a longer-term psychotic disorder, most commonly schizophrenia. A 2019 meta-analysis by Murrie and colleagues, published in Schizophrenia Bulletin, found[3] that approximately 18% of people who experienced a substance-induced psychosis later converted to a diagnosis of schizophrenia or a related disorder. Cannabis had one of the highest conversion rates among all substances studied.
This does not mean cannabis caused the schizophrenia. The prevailing clinical interpretation is that these individuals already had the genetic and neurodevelopmental foundation for a psychotic disorder, and cannabis accelerated the timeline or acted as the triggering event. Without cannabis, the disorder may have emerged later, or possibly not at all.
This is particularly relevant for younger users. The typical age of onset for schizophrenia overlaps with the peak years of cannabis use (late teens to mid-twenties), and the developing brain is more susceptible to both THC-driven disruption and the emergence of psychotic disorders.
What to Do If This Happens
If you or someone you know experiences psychotic symptoms during or after cannabis use, the immediate priorities are safety and medical evaluation.
During the episode. Stay calm. Do not argue with the person about their hallucinations or delusions. Trying to convince someone in psychosis that their perceptions are wrong is unlikely to work and can increase agitation. Keep the environment quiet and low-stimulation. Remove any objects that could be dangerous. If the person is a danger to themselves or others, or if the episode is severe, call 911.
After the episode resolves. Seek a psychiatric evaluation, even if the person feels completely normal. The evaluation serves two purposes: it rules out other causes of the psychotic symptoms (some medical conditions and other substances can produce psychosis), and it assesses the person's risk for recurrence or for an underlying psychotic disorder.
Going forward. A single episode of cannabis-induced psychosis is a strong clinical signal that the individual should not use cannabis again, particularly high-potency products. The risk of recurrence with continued use is elevated. If there is a family history of psychotic disorders, this signal is even stronger.
If cannabis has been a regular part of your life and you are concerned about dependence or withdrawal, a healthcare provider can help you develop a plan for stopping safely. If you have been using cannabis to manage anxiety, stress, or emotional pain, understanding the pattern of self-medicating with weed can help clarify why stopping feels so difficult and what to address alongside cessation.
When to Seek Professional Help
Any psychotic symptom, hallucinations, delusions, or a sustained break from reality, warrants professional evaluation. Do not wait to see if it happens again. A psychiatric assessment after a first episode is standard clinical practice and does not commit you to any particular treatment.
Seek immediate help if you or someone you know is currently experiencing psychotic symptoms. Go to the nearest emergency department or call 911 if there is any concern about safety.
SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and open 24 hours a day, 7 days a week. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
What This Means for You
Cannabis-induced psychosis is not common. The vast majority of people who use cannabis will never experience it. But the risk is not zero, and it is not evenly distributed. If you use high-potency products, use daily, started using during adolescence, or have a family history of psychotic disorders, your individual risk is meaningfully higher than the population average.
Knowing this does not mean you have to live in fear. It means you have the information to make choices that account for your specific situation. If you carry risk factors, lower-potency products, less frequent use, or abstinence are legitimate harm-reduction strategies. If you have experienced psychotic symptoms while using cannabis, even briefly, that is information worth taking seriously and discussing with a healthcare provider.
Your brain is not broken for reacting this way. Some brains are wired to be more sensitive to what THC does at high doses. Understanding that wiring is not a limitation. It is self-knowledge, and self-knowledge is the foundation of every good decision you make from here.
The Bottom Line
Cannabis-induced psychosis is a brief psychotic episode involving hallucinations, delusions, disorganized thinking, and loss of insight (inability to recognize distorted perceptions), triggered by cannabis use and typically resolving within days to weeks. Rising THC potency is driving increasing ER visits: Monte et al. (2019, Annals of Internal Medicine) documented significant increases in psychosis-related cannabis ER visits in Colorado post-legalization, with concentrates and edibles disproportionately represented. Di Forti et al. (2019, The Lancet Psychiatry, 11 European/Brazilian sites) found daily high-potency cannabis use (THC >10%) associated with ~5x odds of first psychotic episode; in cities where high-potency products dominated, a meaningful percentage of first-episode psychosis cases were statistically attributable to cannabis. Genetic vulnerability centers on two genes: COMT Val/Val variant (slower dopamine clearance, Caspi et al. 2005, Biological Psychiatry) and AKT1 C/C genotype (~2x psychotic disorder risk, Di Forti et al. 2012, Biological Psychiatry). Family history of psychotic disorders is the most accessible risk indicator. Critical distinction: most cannabis-induced psychosis is temporary, but Murrie et al. (2019, Schizophrenia Bulletin) found approximately 18% of substance-induced psychosis cases later converted to schizophrenia or related disorder — cannabis had one of the highest conversion rates. This is interpreted as cannabis triggering or accelerating an existing genetic predisposition rather than causing the disorder de novo.
Sources & References
- 1RTHC-02190·Monte, Andrew A et al. (2019). “Edible cannabis caused more psychiatric and cardiovascular ER visits than expected based on sales volume.” Annals of internal medicine.Study breakdown →PubMed →↩
- 2RTHC-02010·Di Forti, Marta et al. (2019). “Daily High-Potency Cannabis Use and Psychosis Risk: The Largest European Study Drew a Direct Line.” The Lancet Psychiatry.Study breakdown →PubMed →↩
- 3RTHC-02739·Murrie, Benjamin et al. (2020). “One-third of cannabis-induced psychosis cases later develop schizophrenia.” Schizophrenia bulletin.Study breakdown →PubMed →↩