Weed and Anxiety: The Paradox That Traps People
Withdrawal & Recovery
3x Potency
THC potency has roughly tripled since the mid-1990s, shifting the average cannabis experience toward the anxiety-producing end of the dose-response curve.
ElSohly et al., Biological Psychiatry, 2016
ElSohly et al., Biological Psychiatry, 2016
View as imageIf you only read one thing
Weed does calm anxiety — but only in the short term. Over weeks and months of regular use, your brain dials down its own anxiety regulation because THC is doing the job. Eventually you need weed just to feel normal, and your anxiety between sessions is worse than it was before you started. About half of regular users get real withdrawal symptoms when they stop, and anxiety is one of the biggest ones. The good news: it's temporary. Most people's anxiety peaks in the first week after quitting and is back to normal (or better) within a month.
Most people who use weed for anxiety did not plan to become dependent on it. The pattern usually starts the same way. You try cannabis. It works. The racing thoughts quiet down, the chest tightness loosens, and for the first time in as long as you can remember, your brain stops scanning for threats. It feels like medicine. It feels like the answer. The question of does weed help or hurt anxiety is one of the most common searches from people caught in this exact loop.
Then, gradually, something shifts. The relief gets shorter. The anxiety between sessions gets worse. You start needing weed not to feel good, but to feel normal. And at some point you realize that you are using cannabis to manage anxiety that was not this bad before you started using cannabis. That is the paradox. And understanding exactly how it works is the first step toward getting out of it.
Key Takeaways
- Cannabis has a two-phase effect on anxiety — low doses tend to calm it and high doses tend to make it worse — and individual genetics, sex, and baseline anxiety level determine where that line falls for you
- Long-term regular use is linked to higher rates of anxiety disorders, not lower, despite the short-term relief
- The cycle goes like this: weed calms anxiety, tolerance builds, anxiety comes back between sessions, you use more weed to manage anxiety that weed is now partly causing
- THC potency has roughly tripled since the mid-1990s, while CBD and terpenes that may buffer anxiety have been stripped out of modern products
- CBD has genuine anxiolytic properties through a different brain pathway than THC, but switching substances does not break an avoidance-based coping pattern
- About 47% of regular cannabis users get clinically significant withdrawal symptoms when they stop, and anxiety is one of the most commonly reported
- No large placebo-controlled trial has shown that cannabis improves anxiety disorders long-term — the evidence for medical cannabis and anxiety is weaker than most people assume
- Breaking the cycle means a temporary spike in anxiety during withdrawal before your natural regulation comes back online, typically by weeks 2 to 4
The Short-Term Effect: Why It Feels Like It Works
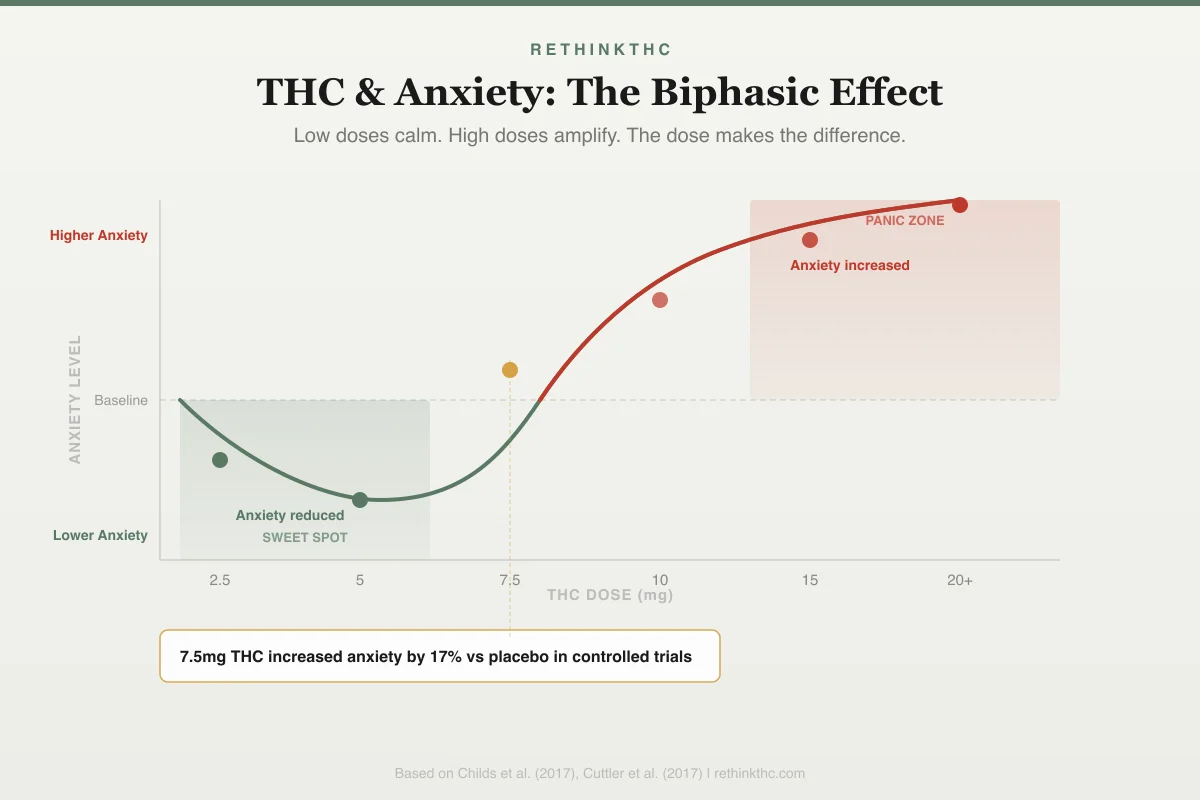
Cannabis does reduce anxiety in the short term. This is not a placebo effect, and it is not "all in your head." There is a documented neurochemical mechanism behind it. The chart below shows exactly where that line sits — and why the gap between calm and panic is narrower than most people think.
Biphasic Dose Response
THC & Anxiety: The Dose Makes the Difference
Low doses calm. High doses amplify.
7.5mg THC increased anxiety by 17% vs placebo in controlled trials
A 2009 review by Crippa and colleagues, published in Human Psychopharmacology, examined the full range of cannabis effects on anxiety.[1] They confirmed that cannabinoids modulate the amygdala, your brain's threat detection center. THC dampens amygdala reactivity, which means your brain becomes less sensitive to perceived threats. Situations that would normally trigger an anxiety response get flagged as less dangerous.
At the same time, THC increases GABA activity. GABA is your brain's primary inhibitory neurotransmitter, the chemical that tells neurons to slow down. It is the same system targeted by benzodiazepines like Xanax and Ativan. When THC boosts GABA, you feel genuinely calmer. Your thoughts slow. Your muscles relax. The physical experience of anxiety diminishes.[1]
THC also suppresses glutamate, your brain's primary excitatory neurotransmitter. Glutamate is the accelerator. GABA is the brake. Cannabis presses the brake and eases off the accelerator at the same time. The net result is a brain that is measurably less reactive to stress.[1]
This is why it feels like medicine. Because pharmacologically, in the short term, it is functioning like one.
The Dose Problem: When Relief Becomes Panic
Even in single sessions, the relationship between weed and anxiety is not straightforward. Crippa's 2009 review identified what researchers call a biphasic response, meaning the effect reverses depending on the dose.[1]
At low doses, THC tends to reduce anxiety. At high doses, THC tends to increase it, sometimes dramatically. High-dose THC can trigger acute anxiety reactions, paranoia, and in some cases full panic attacks. Crippa and colleagues noted that anxiety reactions are among the most frequent acute adverse effects of cannabis use.
This creates a narrow window. The amount that calms you and the amount that sends you into panic are not that far apart, and the line between them shifts based on your tolerance, the specific product, your mental state going in, and your environment. Anyone who has ever taken one hit too many and spent the next two hours convinced their heart was going to explode has experienced the upper end of this biphasic curve. The biphasic effect explained in detail covers exactly why low doses calm and high doses panic, and what determines where your threshold sits.
High-dose anxiety reactions can escalate into full panic attacks or intense paranoia, both of which are among the most common reasons people end up in emergency rooms for cannabis-related complaints.
This problem has gotten worse over time. A 2016 study by ElSohly and colleagues, published in Biological Psychiatry, documented that THC potency in cannabis products roughly tripled between 1995 and 2014[2], increasing from approximately 4 percent to approximately 12 percent. Concentrates and modern vape cartridges can exceed 80 percent THC. The products available today push users toward the anxiety-producing end of the dose curve far more easily than what was available a generation ago.
What to Do If You Are Having a Cannabis Panic Attack Right Now
If you landed on this page mid-panic, here is what you need to know right now.
You are not dying. Your heart is racing because THC stimulates your sympathetic nervous system. It feels terrifying, but it is not a heart attack. If you smoked or vaped, the acute effects will peak within minutes and begin fading within 2 to 3 hours.[9] If you ate an edible, it may take longer — up to 4 to 6 hours — but it will still end.
Breathe slowly. Inhale for 4 counts, hold for 7, exhale for 8. Repeat until your heart rate drops. If counting feels impossible, just make your exhale longer than your inhale. That is enough. More techniques are in the breathing exercises guide.
Ground yourself. Name 5 things you can see, 4 you can touch, 3 you can hear, 2 you can smell, 1 you can taste. This pulls your brain out of the spiral. The full grounding techniques guide has more options.
Try black pepper. Some people find that chewing black peppercorns or sniffing ground pepper helps reduce THC-induced anxiety. The terpene beta-caryophyllene in black pepper may interact with cannabinoid receptors. It is anecdotal but widely reported.
A 2022 randomized controlled trial found that cannabis containing equal amounts of THC and CBD produced significantly less anxiety than THC-dominant cannabis, especially when baseline anxiety was low before use.[10] If you have CBD on hand, it may take the edge off, though it will not work instantly if you are already mid-panic.
For a full walkthrough of what is happening in your body and why, see greening out explained, weed panic attacks, or if you are helping someone else, how to help someone who is greening out.
Why Weed Makes Some People Anxious and Others Calm
The dose curve is real, but it is not the whole story. Two people smoke the same joint. One relaxes. The other has a panic attack. Same THC, same setting, opposite outcomes. The paradox goes deeper than dose.
Your Genetics Set the Starting Line
Your DNA influences how your body processes THC and how your brain responds to it. Several gene variants have been linked to cannabis-anxiety sensitivity.
One of the most studied is the FAAH gene (C385A variant). FAAH is the enzyme that breaks down anandamide, your body's internally produced cannabinoid. People who carry the C385A variant break down anandamide more slowly, meaning they walk around with naturally higher endocannabinoid tone. For these individuals, adding external THC on top of an already active endocannabinoid system may push the balance past the anxiety threshold more easily.
A 2017 randomized controlled trial using both fMRI and PET imaging found that individual differences in amygdala CB1 receptor density directly predicted how much anxiety THC produced.[11] People with more CB1 receptors in their amygdala experienced more THC-induced anxiety. Your brain's hardware literally determines how much anxiety a given dose produces.
Another gene variant — AKT1 — affects sensitivity to THC's cognitive effects. A double-blind study found that carriers of the AKT1 rs1130233 A-allele made significantly more errors on a cognitive task after THC, while people without that variant were unaffected.[12] If THC scrambles your thinking, that cognitive disruption feeds into anxiety.
None of this means cannabis sensitivity is entirely predetermined. But it does mean that "weed helps my anxiety" from one person and "weed gives me panic attacks" from another can both be genetically honest statements about the same drug.
Sex, Tolerance, and Starting State
The literature suggests that women may be more sensitive to certain acute effects of cannabis, including anxiety and cognitive disruption, though the findings are not as large or consistent as many people assume. Hormonal cycles, body composition, and metabolism all influence how THC distributes and how long it stays active.
Tolerance matters enormously. Regular users have downregulated CB1 receptors, which shifts their dose-response curve to the right. What panics a first-time user may barely register for a daily user. But tolerance to the anxiety-producing effects and tolerance to the calming effects do not develop at the same rate, which is one reason the therapeutic window narrows over time.
Your baseline anxiety level going in may be the single most important variable. The Hutten 2022 study found that when baseline anxiety was low, CBD completely counteracted THC-induced anxiety. When baseline anxiety was already high, CBD did not help.[10] If you are already anxious before you use, you are starting closer to the panic threshold. The margin for error is smaller.
Set and Setting
Your mindset going in and the environment you use in both modulate the pharmacological response. Using alone in a familiar, safe space while relaxed produces a different experience than using at a loud party while already on edge. This is not woo. It is context-dependent pharmacology. The same dose in different conditions produces measurably different subjective effects.
This is why asking "is weed good or bad for anxiety" is the wrong question. The right question is: what is weed doing to YOUR anxiety, given YOUR genetics, YOUR tolerance, and YOUR baseline?
CBD vs THC: A Different Pathway, Not an Escape
When people realize that THC is worsening their anxiety, the first thing many of them reach for is CBD. It is marketed as the anxiolytic alternative — all the calm, none of the panic. The pharmacology partially supports this. But the full picture is more complicated than the marketing suggests.
CBD does not work through the same mechanism as THC. Where THC binds directly to CB1 receptors in your brain (which is what produces the high, the amygdala dampening, and at higher doses, the anxiety), CBD primarily modulates serotonin 5-HT1A receptors — the same target as buspirone, a prescription anti-anxiety medication. CBD also inhibits the breakdown of anandamide, which means it may gently boost your body's own endocannabinoid signaling without the flood that comes from THC.
The clinical evidence is real but limited. A 2011 randomized controlled trial gave 600 milligrams of pharmaceutical-grade CBD to patients with social anxiety disorder who had never been treated. During a simulated public speaking test, the CBD group showed significantly less anxiety, cognitive impairment, and discomfort than the placebo group — performing nearly identically to healthy controls.[13]
A 2024 quasi-experimental study by Bidwell and colleagues at the University of Colorado Boulder compared CBD-dominant and THC-dominant cannabis use over four weeks. CBD-dominant users reported lower anxiety scores, less tension, and less paranoia than THC-dominant users.[14]
Those are encouraging findings. Here is the problem.
Most consumer CBD products are nothing like what was used in clinical trials. The Bergamaschi study used 600 milligrams of pharmaceutical-grade, lab-verified CBD. Most CBD gummies and tinctures on the market contain 10 to 25 milligrams per dose, and independent lab testing repeatedly shows that the actual CBD content often does not match the label. Some products contain enough THC to trigger cravings or produce mild intoxication. The unregulated market makes consistent dosing nearly impossible.
More importantly, even if the CBD is high quality and accurately dosed, switching from THC to CBD does not break the anxiety cycle if the underlying pattern is avoidance-based coping. If you are reaching for a substance every time anxiety shows up — any substance, including CBD — you are still outsourcing your anxiety regulation to something external. You are still in the trap. The substance changed; the pattern did not.
For someone choosing between THC and CBD, CBD is the less harmful option. But switching the substance without examining the pattern keeps the avoidance intact. For more on CBD's anxiolytic properties, see the guide on CBD and anxiety research. If you are considering CBD specifically during the quitting process, CBD for weed withdrawal covers the tradeoffs. And for a broader comparison of how the two compounds work differently in your brain, see CBD vs THC.
The Terpene Factor: Why Your Grandparents' Weed Did Not Do This
There is one more piece of the anxiety puzzle that most people never consider: it is not just that modern weed has more THC. It is that modern weed has lost the other compounds that may have been protecting you from THC's anxiety effects.
ElSohly's potency analysis found that between 1995 and 2014, while THC content tripled, the CBD-to-THC ratio collapsed from approximately 14:1 to 80:1.[2] CBD nearly vanished from the supply. But it was not just CBD. Whole-plant cannabis contains dozens of terpenes — aromatic compounds that give different strains their distinct smells and flavors — and there is growing evidence that some of these terpenes modulate THC's effects on anxiety.
In 2024, a double-blind randomized controlled trial at Johns Hopkins University tested d-limonene, a terpene found in citrus peels and many cannabis strains, alongside THC. Participants who received 30 milligrams of THC with 15 milligrams of d-limonene reported significantly less anxiety and paranoia than those who received the same dose of THC alone. D-limonene did not alter THC's pharmacokinetics or any of its other effects — it selectively reduced the anxiety.[15] This is the first rigorous human evidence for what researchers call the entourage effect: the idea that cannabis compounds work differently together than in isolation.
The practical implication is that the market has been moving in exactly the wrong direction for anxiety. Concentrates, distillate vape cartridges, and high-THC flower have been selectively bred and processed to maximize THC while stripping out CBD, terpenes, and other minor cannabinoids. The products that dominate today are pharmacologically different from the whole-plant cannabis that existed a generation ago. They deliver more of the compound that produces anxiety and less of the compounds that may have been buffering it.
This is still emerging research. The Spindle RCT is a single study, and optimal terpene ratios for anxiety reduction have not been established. But it raises a question worth sitting with: some of the anxiety epidemic among cannabis users may not just be about who is using or how much they are using. It may be about what they are using.
This reinforces the paradox from another angle. The cannabis market, driven by consumer demand for higher potency, is engineering products that make the anxiety trap more likely, not less.
The Long-Term Trap: How Relief Becomes the Problem
The short-term anxiolytic (anxiety-reducing) effects of cannabis are real. The problem is what happens when those short-term effects meet daily use over weeks, months, and years.
Your brain adapts. This is not a flaw in your brain. It is what brains do. When any external chemical consistently alters a neurochemical system, the brain adjusts its own production to compensate. With regular cannabis use, this means your brain reduces its sensitivity to GABA (because THC is boosting it externally), increases glutamate receptor density (because THC is suppressing it externally), and downregulates CB1 receptors (the docking stations THC binds to).[7]
The result is tolerance. The same amount of weed produces less anxiety relief. So you use more, or switch to stronger products, which drives further adaptation. Meanwhile, your brain's natural anxiety regulation capacity has declined because it has been outsourced to THC.
This is where the trap closes. Between sessions, when THC levels in your brain dip, your anxiety spikes. Not to your old baseline, but above it. Your GABA system is dampened. Your glutamate system is sensitized. Your amygdala, which THC had been suppressing, rebounds with increased reactivity. You feel more anxious sober than you did before you ever started using weed. If you have been using for years and this pattern sounds familiar, you are experiencing what happens when weed stops working for anxiety.
The logical response to that anxiety is to use again. And it works, briefly. The THC pushes the numbers back toward manageable for a few hours. Then it wears off, the rebound returns, and the cycle repeats. You are now using cannabis to treat withdrawal-induced anxiety that would not exist without the cannabis.
Crippa's review found a high prevalence of anxiety disorders among frequent cannabis users[1], a finding reinforced by a 2019 meta-analysis linking adolescent cannabis use to significantly increased risk of anxiety in young adulthood.[8] The relationship is complicated (some people with anxiety are drawn to cannabis, while cannabis use can also generate anxiety), but the bidirectional nature of the relationship is well-established. Whether cannabis caused your anxiety or your anxiety led you to cannabis, regular use tends to worsen the anxiety picture over time.
The Withdrawal Layer
When someone who has been using daily for months or years decides to quit, the anxiety gets worse before it gets better. This is withdrawal anxiety, and it is biologically distinct from both your natural anxiety baseline and the rebound anxiety between sessions.
A 2020 meta-analysis by Bahji and colleagues, published in JAMA Network Open, found that approximately 47 percent of regular cannabis users experience clinically significant withdrawal symptoms when they stop.[3] Anxiety is one of the most commonly reported withdrawal symptoms, often described as a persistent, free-floating dread that does not attach to any specific worry.
During withdrawal, the adaptations your brain made to accommodate daily THC are now working against you. Your dampened GABA system is running without the THC that was compensating for it. Your upregulated glutamate receptors are firing without anything to suppress them. Your amygdala is fully unsuppressed for the first time in however long you have been using. Your cortisol (stress hormone) regulation is disrupted. For some people, this manifests as health anxiety during weed withdrawal, where the physical sensations of withdrawal trigger fears of serious illness that compound the existing anxiety.
The combination produces anxiety that can feel more intense than anything you experienced before using cannabis. This is not evidence that you need weed. It is evidence that your brain adapted to weed and is now readjusting to life without it. The weed withdrawal anxiety article covers this phase in clinical detail, including the timeline for resolution.
For most people, withdrawal anxiety peaks between days 3 and 10 and resolves significantly by weeks 2 to 3.[6] By day 28, CB1 receptors have returned to approximately normal density[5], and the biological basis for withdrawal-driven anxiety has largely resolved.
Here is how the three types break down by origin, timeline, and what to do about each one.
| Type | Origin | Timeline | What to Do |
|---|---|---|---|
| Withdrawal anxiety | Neurochemical rebound from stopping THC | Peaks days 3–10, resolves weeks 2–4 | Wait it out; exercise, sleep hygiene, breathing exercises |
| Cannabis-induced anxiety | Develops during months/years of regular use | Resolves after quitting, may take longer than withdrawal | Quit and allow full recalibration (4–8 weeks) |
| Pre-existing anxiety | Present before cannabis use began | Persists beyond 6 weeks of abstinence | Professional treatment (therapy, possibly medication) |
| Combined | Mix of pre-existing + cannabis-worsened | Withdrawal layer resolves first; baseline remains | 4–6 weeks abstinence to separate the layers, then targeted treatment |
Does Medical Cannabis Actually Treat Anxiety?
Anxiety is one of the top qualifying conditions for medical cannabis in most legal states. Surveys of medical cannabis patients consistently report that cannabis reduces their anxiety — one study of over 1,500 dispensary members found that 71.8 percent reported reducing their anti-anxiety medications after starting medical cannabis. Those patient experiences are real.
But qualifying condition does not equal proven treatment. And patient-reported substitution is not the same as a placebo-controlled trial.
Here is what the rigorous evidence actually shows: no large, randomized, placebo-controlled trial has demonstrated that cannabis (THC-dominant or whole-plant) improves anxiety disorders over the long term. The strongest clinical data is for CBD specifically, not THC, and mostly from small trials or pilot studies. The evidence for nabilone (a synthetic cannabinoid) reducing PTSD-related nightmares is the one area with relatively consistent support, but that is a specific symptom in a specific condition, not a general anxiolytic effect.
Meanwhile, the epidemiological data points in the opposite direction. A 2026 systematic review found that cannabis use disorder is notably prevalent among people with anxiety disorders.[16] A 2019 meta-analysis found that cannabis use in adolescence is linked to significantly increased risk of anxiety in young adulthood.[8] The short-term relief is well-documented. The long-term benefit is not.
The disconnect makes sense once you understand the paradox. Medical cannabis patients feel better in the short term for the same reason recreational users feel better in the short term: THC dampens the amygdala and boosts GABA. But the neuroadaptation, tolerance, and rebound cycle described throughout this article does not care whether your cannabis came with a medical recommendation or not. The pharmacology is the same.
This article is not anti-cannabis. It is pro-evidence. If medical cannabis helps you function, you are under clinical supervision, and your provider is monitoring your anxiety trajectory over time, that is a legitimate treatment choice. But if "medical" is a label you are using to avoid examining whether cannabis is making your anxiety worse over months and years, the paradox still applies. For a broader look at what the research does and does not support, see medical benefits of cannabis.
The Three Types of Anxiety in Cannabis Users
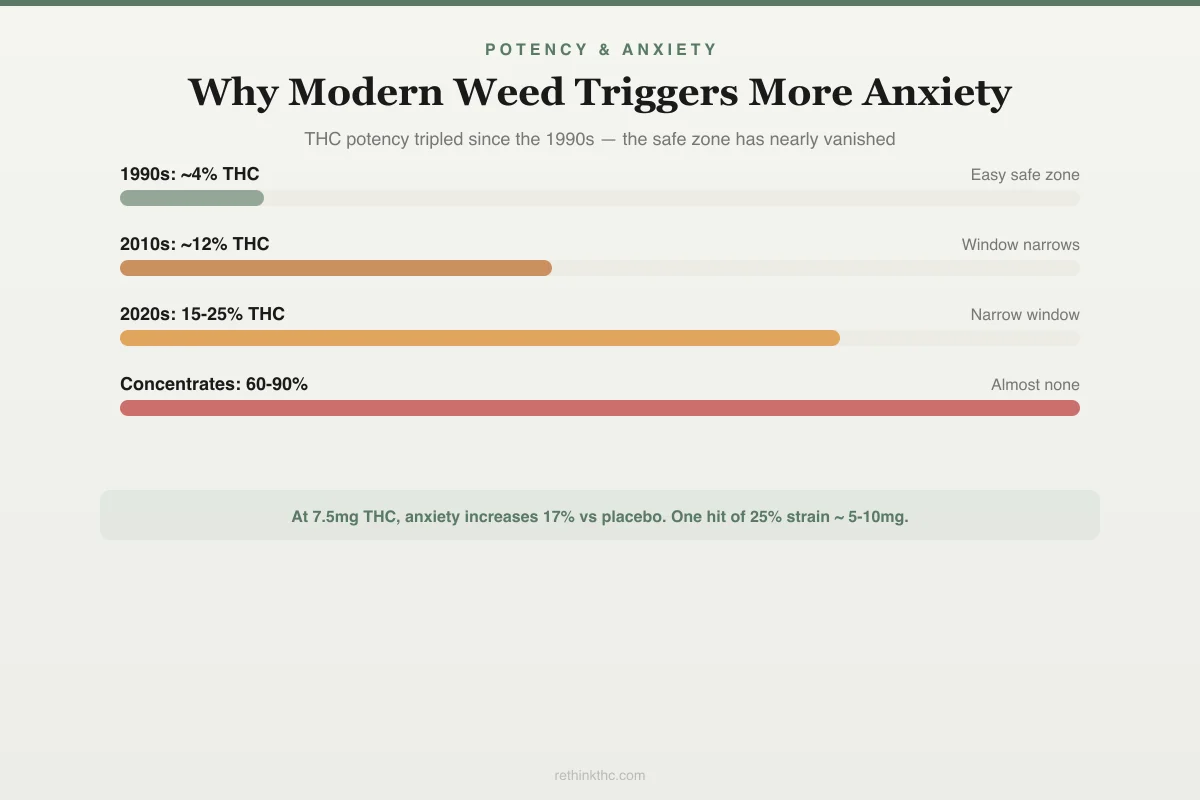
Understanding which type of anxiety you are dealing with determines what to do about it. There are three distinct patterns, and they require different approaches. The infographic below shows why this problem has gotten dramatically worse over the past two decades.
Potency & Anxiety
Why Modern Weed Triggers More Anxiety
THC potency roughly tripled since the 1990s. The "safe zone" for anxiety relief has nearly vanished.
Low dose easy
Easier to stay in anxiety-reducing zone
Window narrows
Harder to avoid anxiety-producing doses
Narrow window
Even one hit can cross the anxiety threshold
Almost none
Nearly impossible to microdose. Panic zone likely.
At 7.5mg THC, anxiety increases 17% vs placebo. One hit of a 25% strain delivers ~5-10mg — right at the tipping point.
Withdrawal anxiety is the acute increase in anxiety that occurs when you stop using after regular use. It follows the cannabis withdrawal timeline, peaks in the first week, and resolves within 2 to 4 weeks.[6] If your anxiety appeared only after you quit and improves steadily over weeks, this is likely what you are experiencing.
Cannabis-induced anxiety develops during or as a result of regular use. You were not particularly anxious before you started using, but over months or years of use, anxiety became a feature of your life. This type typically resolves after quitting, though it may take longer than pure withdrawal anxiety because the sensitization built up over a longer period. The does weed help anxiety article examines this pattern in depth.
Pre-existing anxiety was present before cannabis entered the picture. You started using weed specifically because you were anxious, and it worked for a while. When you quit, the withdrawal anxiety eventually fades, but the underlying anxiety condition remains because it was never caused by cannabis in the first place. It was masked by it. The self-medicating anxiety with weed article covers this scenario and what to do about it. If your anxiety takes the form of generalized anxiety disorder (GAD), the interplay with cannabis use has its own specific pattern worth understanding.
Many people have a combination. You may have had mild anxiety before using, used weed to manage it, and had your anxiety worsened by both the chronic use and the withdrawal. The way to sort this out is time. Give yourself at least 4 to 6 weeks of abstinence. The withdrawal anxiety will resolve in that window. Whatever remains after 6 weeks is likely your actual baseline and can be addressed with a healthcare provider.
The withdrawal anxiety vs real anxiety article provides a detailed framework for telling these apart.
Weed and Specific Anxiety Disorders
The paradox does not affect all anxiety disorders equally. Cannabis interacts differently with each one, and understanding your specific pattern matters for deciding what to do next.
Generalized Anxiety Disorder (GAD)
GAD may be the anxiety disorder most tightly interwoven with cannabis use. A 2016 longitudinal study of over 2,500 adolescents found that generalized anxiety was the only anxiety symptom that independently predicted both starting cannabis use and using more frequently over time.[18] People with GAD are drawn to cannabis because the constant, diffuse worry responds well to THC's amygdala dampening. It works, until tolerance makes it stop working, and then the rebound worry is worse than what you started with.
A 2025 analysis of the National Epidemiologic Survey found that under DSM-5 criteria, past-year generalized anxiety disorder was significantly associated with past-year cannabis use disorder.[17] GAD and cannabis use disorder feed each other. The paradox in its purest form.
For a deep dive into this specific interplay, see weed and generalized anxiety disorder.
Social Anxiety Disorder
Cannabis removes social inhibition. For someone with social anxiety, a hit before a party can feel like putting on armor. The problem is that every social success while high gets attributed to the weed, not to you. You never build the evidence that you can handle social situations on your own. The more you rely on cannabis for social confidence, the less natural social confidence you develop.
A 2023 nationally representative survey found significant cannabis use prevalence among people with DSM-5 social anxiety disorder.[19] Interestingly, the CBD research here is relatively strong. The Bergamaschi 2011 RCT showed that 600 milligrams of CBD reduced social anxiety during a public speaking test to levels comparable to healthy controls.[13] But the same avoidance-trap caveat applies: if CBD becomes the new thing you need to take before social situations, you are still outsourcing your anxiety regulation.
For the full picture, see weed and social anxiety.
Panic Disorder
Here the data tells a surprising story. A 3-year population-based longitudinal study found that cannabis use was not associated with an increased risk of developing new anxiety disorders, including panic disorder.[20] However, people who already had panic disorder were significantly more likely to start using cannabis — classic self-medication. The problem is not that cannabis causes panic disorder. It is that people with panic disorder are drawn to cannabis, and the withdrawal rebound cycle makes panic episodes more frequent and more intense over time.
For more on the acute panic experience, see weed panic attacks.
PTSD
The biology linking the endocannabinoid system to PTSD is compelling. PTSD involves hyperactivation of the threat circuitry — exactly what THC dampens. Veterans and trauma survivors often describe cannabis as the only thing that quiets the hypervigilance, reduces nightmares, and allows sleep. The endocannabinoid system is directly involved in fear extinction (the process by which your brain learns that a threat has passed), and there is a reasonable biological case that modulating this system could help.
But the clinical evidence has not matched the biology. Reviews of the literature have found that the one area with consistent signal is nabilone (a synthetic cannabinoid) for PTSD-related nightmares. Beyond that, cannabis use in PTSD patients is associated with worse overall outcomes in depression, anxiety, and substance misuse. The withdrawal rebound on threat circuitry is particularly devastating for people whose threat circuitry was already dysregulated by trauma.
For a dedicated guide, see quitting weed with PTSD.
The Common Thread
Each disorder has its own version of the paradox. The mechanism differs — amygdala dampening for GAD, social disinhibition for social anxiety, threat circuit suppression for PTSD — but the trap is the same. Short-term relief. Long-term worsening. A withdrawal barrier that makes quitting feel like proof you need the drug.
Why the Paradox Is So Effective at Trapping People
The reason so many people get stuck in the weed-and-anxiety cycle is not weakness or lack of willpower. It is because the cycle is neurologically reinforcing at every step.
Immediate relief is more persuasive than delayed harm. Your brain weighs near-term consequences far more heavily than long-term ones. A hit that eliminates anxiety in 10 minutes is neurologically more compelling than abstract knowledge that daily use worsens anxiety over months. This is not a character flaw. It is how human reward circuitry works.
The comparison point shifts. When your between-session anxiety is worse than your pre-cannabis anxiety (because of tolerance and rebound effects), the relief from using feels even more dramatic. You are comparing "anxious from withdrawal" to "calm after a hit," which makes cannabis seem more effective than it actually is. If you could compare "calm after a hit" to "how you would feel after 4 weeks of no use," the picture would look very different. But you cannot feel that future state. You can only feel the present one.
The withdrawal barrier. Every attempt to quit involves a period where anxiety gets worse before it gets better. If you do not know this is coming, or if you do not know it is temporary, the obvious conclusion is "I need weed to manage my anxiety." Each failed quit attempt reinforces the belief that cannabis is necessary, when in reality what you experienced was a temporary withdrawal state.
Breaking the Cycle
There is no way to break the cycle without going through a period of increased anxiety. That is the biological reality. Your brain adapted to THC, and undoing that adaptation involves discomfort. But there are ways to make the process more manageable. If you are in the early days and your anxiety feels unbearable, understanding why anxiety gets worse before it gets better can help you hold on.
Understand the timeline. Knowing that withdrawal anxiety peaks in the first week and resolves by weeks 2 to 3 changes your relationship to the discomfort. It is not indefinite. It is a defined window with a documented endpoint.
Address sleep. Anxiety and sleep disruption feed each other during withdrawal. Poor sleep increases anxiety sensitivity, and elevated anxiety disrupts sleep. Breaking one side of this cycle helps the other. Practical sleep strategies make a meaningful difference. See how to sleep without weed for evidence-based approaches.
Use active coping techniques. When anxiety spikes acutely, breathing exercises designed for withdrawal anxiety and grounding techniques can bring your nervous system back under control within minutes. The anxiety response technique for weed withdrawal provides a structured step-by-step method you can use in real time when anxiety escalates. These are not permanent fixes, but they get you through the acute moments.
Exercise. Aerobic exercise increases your body's production of endocannabinoids, the natural chemicals that THC mimics. A 2012 study by Raichlen and colleagues, published in the Journal of Experimental Biology, found that exercise significantly increases endocannabinoid levels[4], contributing to the phenomenon known as "runner's high." During withdrawal, exercise partially replaces the endocannabinoid boost that THC was providing.
Do not judge your baseline by the first two weeks. Your anxiety during acute withdrawal is not your anxiety without weed. It is your anxiety during a temporary neurological transition. Your actual sober baseline will not be clear until at least 4 weeks after quitting.[5] Making conclusions before then is like judging the weather by looking at a storm.
Consider professional support. If your anxiety before cannabis was severe enough to drive daily self-medication, there is a real possibility that an underlying anxiety condition needs treatment. A therapist or psychiatrist can help you address the root cause rather than managing it through a cycle of use and withdrawal. The guide on whether you need therapy to quit weed can help you decide, and if you are currently on medication, quitting weed while on anxiety medication covers what to discuss with your prescriber. This is not a detour. For many people, it is the actual solution. For a complete step-by-step plan, see our guide on how to quit weed.
The Other Side of the Paradox
There is a version of this that nobody talks about while they are in the cycle, but that people consistently describe after they have been through it.
Your anxiety regulation system, once it has recovered from chronic THC exposure, works. Not perfectly. Not like a drug that switches anxiety off. But it works the way it is supposed to: responding proportionally to actual circumstances, recovering after stress, allowing you to sit with moderate discomfort without it spiraling into panic. The emotional range you get back includes some anxiety, because anxiety is a normal human signal. But it also includes the ability to process and move through anxiety on your own, without needing to reach for something external every time. You may also notice that your social behavior shifts as the anxiety recalibrates, which is a normal part of rediscovering how you relate to people without THC modulating your comfort level. And if you have been wondering why weed makes you anxious now when it did not before, that reversal is itself a signal that your neurochemistry has shifted in response to chronic use.
That capacity was always there. It was just offline while THC was doing the job for it. The paradox of weed and anxiety is that the thing that seems to fix the problem is the thing that prevents you from developing the ability to handle the problem yourself.
Safety
ModerateWithdrawal anxiety can feel overwhelming — that's normal, but watch for red flags
Concern
Cannabis withdrawal anxiety peaks in the first week and can feel more intense than anything you experienced before using. For most people it resolves within 2-4 weeks. But in some cases — especially if you had severe anxiety before cannabis — withdrawal can unmask symptoms that need professional treatment.
What the research says
The key distinction: withdrawal anxiety improves steadily week over week. If your anxiety is getting worse after 2 weeks, is not improving at all by week 4, or includes daily panic attacks or thoughts of self-harm, that's beyond normal withdrawal.
Particularly relevant for: Anyone quitting after months or years of daily use, especially those who started using specifically to manage anxiety
What to do
If anxiety is severe enough to prevent working, maintaining relationships, or leaving the house — or if you have any thoughts of self-harm — reach out now. SAMHSA: 1-800-662-4357 (free, 24/7). Crisis Text Line: text HELLO to 741741.
Bahji et al. (2020), JAMA Network Open; Budney et al. (2003), J Abnorm Psychol
When to Seek Professional Help
Anxiety is a normal part of cannabis withdrawal for most people. It is uncomfortable but temporary and resolves without medical intervention in the majority of cases.
However, seek professional help if your anxiety is severe enough to prevent you from working, maintaining relationships, or caring for yourself. If withdrawal anxiety is making it difficult to leave the house, that level of impairment warrants professional support. Seek help if you are experiencing daily panic attacks that persist beyond two weeks. Seek help if you had a diagnosed anxiety disorder before using cannabis and symptoms return with full intensity after quitting. And seek immediate help if you experience any thoughts of self-harm.
SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and open 24 hours a day, 7 days a week. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
Getting professional support is not a sign that quitting failed. It is a sign that you are taking your mental health seriously enough to address it directly rather than through self-medication.
The Bottom Line
Weed calms anxiety in the short term, but regular use makes anxiety worse over time. Your brain adapts to THC by dialing down its own anxiety regulation, which means you feel more anxious between sessions than you did before you started using. This creates a cycle where you need weed to manage anxiety that weed is now partly causing. Modern cannabis is much stronger than what was available a generation ago, and the terpenes and CBD that may have buffered anxiety in older products have been stripped out of most concentrates and vape carts. Individual genetics, sex, and baseline anxiety level all affect where you fall on the dose-response curve — which is why the same strain can calm one person and panic another. CBD has real anxiolytic properties, but switching substances does not break the pattern if the pattern is avoidance. Breaking the cycle means going through a temporary spike in anxiety — usually peaking around days 3 to 10 after quitting — before your natural regulation comes back online. By 4 to 6 weeks, most people find their anxiety is equal to or better than it was before cannabis. If anxiety persists beyond 6 weeks, it may be a pre-existing condition worth addressing with a professional.
Sources & References
- 1RTHC-00349·Crippa, Jose Alexandre S. et al. (2009). “Cannabis both calms and panics — the biphasic dose-response explains why the same drug produces opposite anxiety effects.” Human Psychopharmacology: Clinical and Experimental.Study breakdown →PubMed →↩
- 2RTHC-01144·ElSohly, Mahmoud A. et al. (2016). “U.S. Cannabis Potency Tripled Over Two Decades While CBD Nearly Vanished.” Biological Psychiatry.Study breakdown →PubMed →↩
- 3RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩
- 4RTHC-00608·Raichlen, David A. et al. (2012). “Runner's High Has an Endocannabinoid Signature in Humans. Dogs Show It Too..” Journal of Experimental Biology.Study breakdown →PubMed →↩
- 5RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩
- 6RTHC-00134·Budney, Alan J. et al. (2003). “When Heavy Users Quit Cannabis, Symptoms Show Up Fast and Ease Within Two Weeks.” Journal of Abnormal Psychology.Study breakdown →PubMed →↩
- 7RTHC-01338·Bonnet, Udo et al. (2017). “Comprehensive review of cannabis withdrawal: symptoms, brain mechanisms, gender differences, and treatment options.” Substance abuse and rehabilitation.Study breakdown →PubMed →↩
- 8RTHC-02048·Gobbi, Gabriella et al. (2019). “Adolescent cannabis use linked to 37% higher depression risk and 3.5x higher suicide attempt risk in young adulthood.” JAMA psychiatry.Study breakdown →PubMed →↩
- 9RTHC-00138·Grotenhermen, Franjo (2003). “The Complete Guide to How Cannabis Moves Through Your Body.” Clinical pharmacokinetics.Study breakdown →PubMed →↩
- 10RTHC-03920·Hutten, Nadia R P W et al. (2022). “Cannabis with equal THC and CBD causes less anxiety than THC alone, especially in calm users.” Psychopharmacology.Study breakdown →PubMed →↩
- 11RTHC-01334·Bhattacharyya, Sagnik et al. (2017). “THC-induced anxiety in humans is linked to CB1 receptor density in the amygdala.” Scientific reports.Study breakdown →PubMed →↩
- 12RTHC-00771·Bhattacharyya, S et al. (2014). “A specific gene variant determined who lost motor control after THC.” Psychological medicine.Study breakdown →PubMed →↩
- 13RTHC-00472·Bergamaschi, Mateus M et al. (2011). “A single dose of CBD brought social anxiety patients' public speaking anxiety down to the level of people without anxiety disorders.” Neuropsychopharmacology : official publication of the American College of Neuropsychopharmacology.Study breakdown →PubMed →↩
- 14RTHC-05140·Bidwell, L Cinnamon et al. (2024). “CBD-dominant cannabis reduced anxiety more than THC-dominant in people with anxiety symptoms.” Cannabis and cannabinoid research.Study breakdown →PubMed →↩
- 15RTHC-05731·Spindle, Tory R et al. (2024). “The Terpene D-Limonene Reduced THC-Induced Anxiety in Humans.” Drug and alcohol dependence.Study breakdown →PubMed →↩
- 16RTHC-08178·Coles, Ashlee R L et al. (2026). “Up to 1 in 5 People With Anxiety Disorders Also Have Cannabis Use Disorder.” Journal of dual diagnosis.Study breakdown →PubMed →↩
- 17RTHC-08025·Zech, James M et al. (2025). “Cannabis Use Disorder Is Strongly Linked to Generalized Anxiety Under DSM-5 Criteria.” Journal of anxiety disorders.Study breakdown →PubMed →↩
- 18RTHC-01271·Stapinski, Lexine A et al. (2016). “Generalized Anxiety in Teens Was the Strongest Predictor of Starting Cannabis Use.” Drug and alcohol dependence.Study breakdown →PubMed →↩
- 19RTHC-04839·Patel, Tapan A et al. (2023). “Weekly Cannabis Use Was Linked to Greater Social Anxiety Severity and Suicide Risk in a National Sample.” Journal of psychiatric research.Study breakdown →PubMed →↩
- 20RTHC-01151·Feingold, Daniel et al. (2016). “Large Prospective Study Finds Cannabis Use Is Not Linked to Most Anxiety Disorders.” European neuropsychopharmacology : the journal of the European College of Neuropsychopharmacology.Study breakdown →PubMed →↩
What the Research Shows
This section synthesizes 227 peer-reviewed studies on Cannabis and Anxiety. Stronger evidence means more consistency across study types.
THC produces a biphasic dose-response on anxiety: low doses (2.5-5mg) reduce anxiety through CB1-mediated dampening of amygdala reactivity, while higher doses (>10mg) increase anxiety, sometimes to the level of panic attacks, through the same receptor system at higher occupancy
Strong EvidenceCBD reduces experimentally induced anxiety (public speaking, fear conditioning) without producing intoxication, primarily through serotonin 5-HT1A receptor agonism and modulation of amygdala and prefrontal cortex activity, as confirmed by fMRI neuroimaging
Strong EvidenceAdolescent cannabis use is associated with significantly elevated risk of anxiety disorders in young adulthood, with meta-analyses of longitudinal studies reporting 28-87% higher odds depending on the specific anxiety measure
Strong EvidenceA Lancet Psychiatry meta-analysis of 83 RCTs found scarce evidence that cannabinoids effectively treat anxiety disorders as a class, with THC-containing products approximately doubling adverse event rates compared to placebo
Strong EvidenceCannabis use disorder co-occurs with anxiety disorders at rates far exceeding chance — up to 1 in 5 individuals with anxiety disorders also meet criteria for CUD, and the relationship appears bidirectional
Strong EvidenceWhere Scientists Disagree
Areas where research shows conflicting results or ongoing scientific debate.
Whether cannabis use causes anxiety disorders or whether people with anxiety are more likely to self-medicate with cannabis remains unresolved, with evidence supporting both directions and shared genetic vulnerability as a third possibility
Moderate EvidenceCBD shows promise for social anxiety disorder specifically, with one RCT showing it reduced public speaking anxiety to levels comparable to healthy controls, but replication in larger, longer trials is needed
Moderate EvidenceThe role of anxiety sensitivity (the tendency to fear anxiety-related sensations) as a specific psychological mechanism driving problematic cannabis use patterns, distinct from general anxiety severity
Moderate EvidenceWhat We Still Don't Know
- No large-scale, multi-site RCTs have tested CBD for generalized anxiety disorder, panic disorder, or social anxiety disorder over treatment periods longer than 8 weeks.
- The impact of modern high-potency cannabis products (concentrates, high-THC vapes) on anxiety risk has not been studied separately from lower-potency flower, despite dramatically different THC exposure levels.
- Prospective studies tracking anxiety outcomes in medical cannabis patients with anxiety-related qualifying conditions are almost entirely absent — most evidence is retrospective or cross-sectional.
- The interaction between cannabis use and standard anxiety treatments (SSRIs, SNRIs, benzodiazepines, CBT) is poorly characterized, despite the high prevalence of concurrent use.
- Sex-specific anxiety responses to cannabis are understudied, despite preliminary evidence that women may be more susceptible to cannabis-related anxiety, particularly at higher doses.
Evidence Breakdown
Distribution of study types in this research area. Higher-tier evidence (meta-analyses, RCTs) provides stronger conclusions.
Research Timeline
How our understanding of this topic has evolved.
Pre-2010
Crippa's 2009 critical review established the biphasic model. Fusar-Poli's 2009 fMRI study provided the first neuroimaging evidence that THC and CBD have opposing effects on amygdala fear processing. Early research was predominantly mechanistic, building the neurobiological framework.
2010-2015
Bergamaschi's 2011 RCT showed CBD normalizing social anxiety. Blessing's 2015 Neurotherapeutics review consolidated the preclinical and clinical evidence for CBD as an anxiolytic. Research shifted from mechanism to clinical translation, with the first controlled human trials.
2015-2020
The 2019 Lancet Psychiatry meta-analysis challenged the therapeutic narrative with its finding of scarce evidence for cannabinoids treating anxiety disorders. Gobbi's 2019 JAMA Psychiatry meta-analysis quantified the adolescent risk. The field matured from case reports to systematic evidence synthesis.
2020-Present
Raminelli's 2025 meta-analysis of 21 trials distinguished pharmaceutical-grade from consumer-grade CBD efficacy. Coles' 2026 systematic review quantified CUD-anxiety comorbidity. Research is now focused on formulation specificity, subtype-specific treatment, and real-world versus laboratory outcomes. 151 of the 227 studies in this corpus were published during this period.