The Proven Medical Benefits of Cannabis: What Research Supports
Balanced Cannabis Science
79 Trials
A landmark JAMA meta-analysis of 79 randomized controlled trials and 6,462 participants found moderate evidence that cannabinoids help with chronic pain and spasticity, with weaker evidence for most other claimed benefits.
Whiting et al., JAMA, 2015
Whiting et al., JAMA, 2015
View as imageIf you only read one thing
Cannabis has real medical benefits — but only for a few specific conditions. Chronic nerve pain, chemo nausea, MS muscle stiffness, and two rare childhood seizure disorders have decent evidence behind them. Most other claims people make about medical cannabis are running way ahead of what studies actually show. And here's the big catch: almost all the good research used pharmaceutical-grade products with exact doses, not the flower or edibles you'd buy at a dispensary.
Cannabis has real medical applications. That statement should not be controversial, but it often is, because the conversation around cannabis tends to collapse into two opposing camps. One side claims cannabis cures nearly everything. The other dismisses any therapeutic value as stoner mythology. Neither position reflects the research.
The evidence base for medical cannabis is uneven. For some conditions, we have solid data from well-designed studies. For others, we have promising signals buried in small, short-term trials that cannot support the confident claims made about them. And for many popular uses, we have little more than anecdote.
This article walks through what the research actually supports, condition by condition, distinguishes between different types of cannabinoid products, and is honest about the quality-of-evidence problem that defines this entire field.
Key Takeaways
- A 2015 JAMA meta-analysis of 79 randomized controlled trials found moderate evidence that cannabinoids help with chronic pain and spasticity, with weaker evidence for other conditions
- Three FDA-approved cannabinoid medications exist: dronabinol and nabilone (synthetic THC for nausea) and Epidiolex (plant-derived CBD for rare epilepsies)
- The difference between pharmaceutical cannabinoids with controlled dosing and whole-plant cannabis from a dispensary matters — because most clinical evidence comes from the pharmaceutical products
- Cannabis research is held back by federal scheduling restrictions, small sample sizes, short studies, and the fact that dispensary products look nothing like what was tested in clinical trials
- Being honest about what cannabis can and cannot do medically is more useful than dismissing all benefits or overstating weak evidence
- The gap between pharmaceutical cannabinoids in clinical trials and high-THC dispensary products is big enough that treating them as the same thing is genuinely misleading
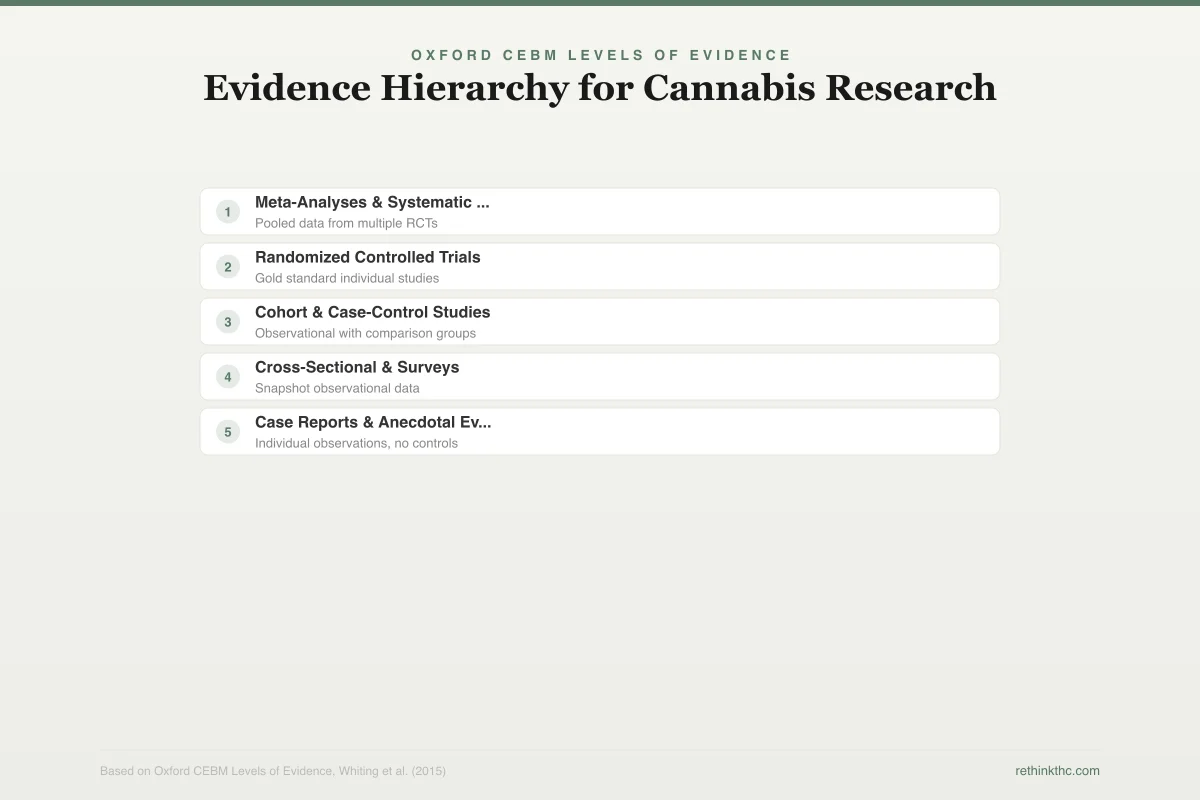
The Evidence Hierarchy: Not All Studies Are Equal
Before reviewing specific conditions, it helps to understand how medical evidence is graded. A single person reporting that cannabis helped their pain is an anecdote. A survey of 500 people reporting the same thing is observational data. A randomized controlled trial (where participants are randomly assigned to receive cannabis or a placebo, and neither they nor the researchers know which is which) is experimental evidence. A meta-analysis that pools the results of many randomized controlled trials is the strongest form of evidence available.
The visual below shows how different types of evidence rank — and why most medical cannabis claims sit in the lower tiers.
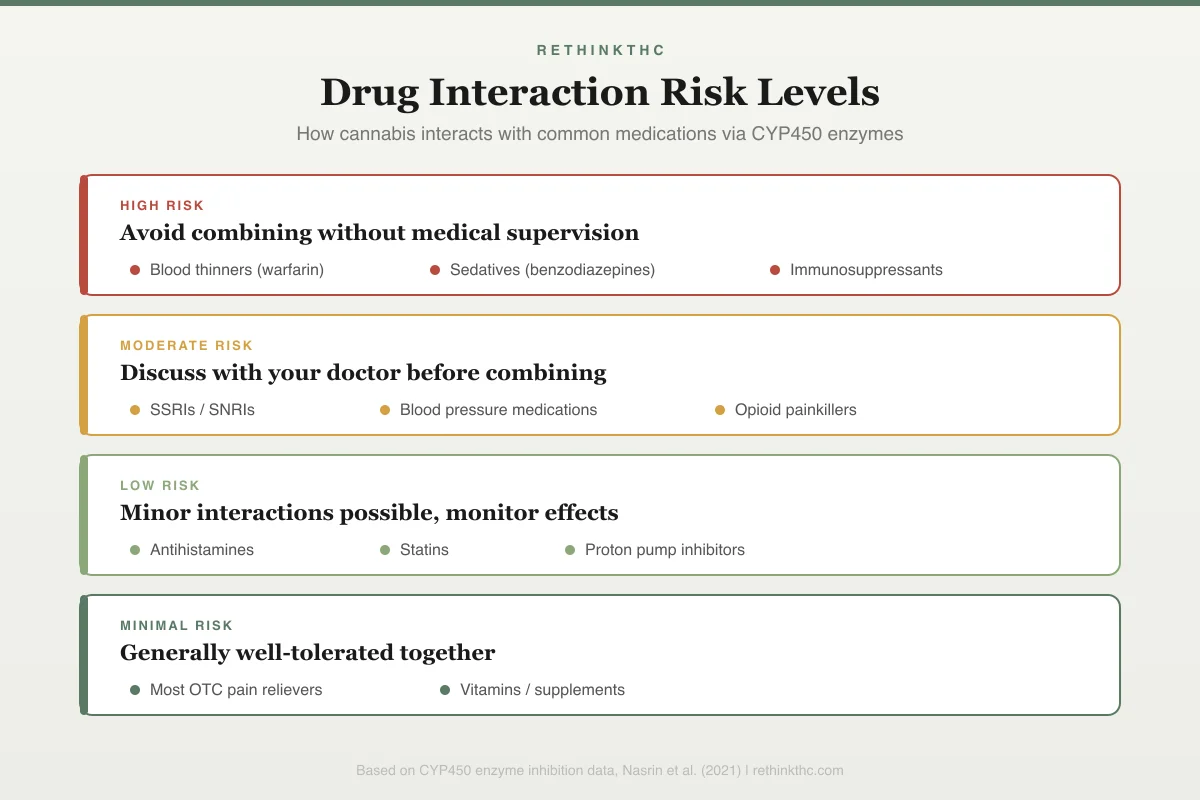
CYP450 Enzyme Interaction Chart
Drug Interaction Risk Levels
Avoid combining without medical supervision
Discuss with your doctor before combining
Minor interactions possible, monitor effects
Generally well-tolerated together
Most of what you read about medical cannabis online comes from anecdotes and observational data. The experimental evidence is thinner than the public conversation suggests. That does not mean the benefits are not real. It means the confidence we can place in specific claims varies enormously depending on which condition we are discussing.
Conditions With the Strongest Evidence
| Condition | Evidence Level | Key Finding | Product Studied |
|---|---|---|---|
| Chronic neuropathic pain | Moderate | Modest but real reduction vs. placebo | Pharmaceutical cannabinoids (dronabinol, nabiximols) |
| Chemo nausea/vomiting | Moderate | Effective in patients who fail standard anti-nausea meds | Dronabinol, nabilone (FDA-approved) |
| MS spasticity | Moderate | Patient-reported improvement; less clear on objective scales | Nabiximols (Sativex) |
| Rare epilepsies | Strong | Significant seizure reduction in Dravet/Lennox-Gastaut | Epidiolex (purified CBD, FDA-approved) |
| Anxiety (CBD) | Preliminary | Preclinical promise; large clinical trials still needed | Pharmaceutical-grade CBD |
| Sleep | Low | Secondary outcome in pain studies; few primary sleep trials | Various |
| PTSD | Limited | Nightmare reduction with nabilone; broader evidence weak | Nabilone (synthetic THC) |
| Appetite (AIDS wasting) | Established | FDA-approved for this indication | Dronabinol (FDA-approved) |
| IBD, glaucoma, depression | Very limited | Insufficient controlled evidence for clinical recommendations | Various |
The pyramid below maps where each evidence type sits in the hierarchy.
Oxford CEBM Levels of Evidence
Evidence Hierarchy for Cannabis Research
Stronger evidence at the top, weaker at the base
Meta-Analyses & Systematic Reviews
Pooled data from multiple RCTs
Randomized Controlled Trials
Gold standard individual studies
Cohort & Case-Control Studies
Observational with comparison groups
Cross-Sectional & Surveys
Snapshot observational data
Case Reports & Anecdotal Evidence
Individual observations, no controls
Most public claims about medical cannabis rely on evidence from the bottom two tiers -- the strongest evidence covers only a few conditions
Chronic Pain
Chronic pain is the condition with the most robust evidence supporting cannabinoid use. A landmark 2015 meta-analysis by Whiting and colleagues, published in JAMA, reviewed 79 randomized controlled trials involving 6,462 participants.[1] A 2022 pharmacology-based meta-analysis covering all relevant medical indications confirmed and extended these findings.[4] Both reviews found moderate-quality evidence that cannabinoids are associated with a greater reduction in chronic pain compared to placebo.
"Moderate-quality evidence" is a specific designation. It means the effect is likely real, but the confidence could be strengthened by additional large, well-designed studies. It is a meaningful finding, not a ringing endorsement and not a dismissal.
The types of chronic pain studied varied. Neuropathic pain (nerve-based pain from conditions like diabetes, HIV, or spinal cord injury) showed the most consistent benefit. Other pain types, including cancer pain, and fibromyalgia, showed more mixed results. The magnitude of relief was real but modest. Cannabinoids do not eliminate chronic pain. They reduce it by a clinically meaningful amount in a subset of patients.
One important caveat: many of the pain studies used pharmaceutical cannabinoid products (dronabinol, nabiximols) with precise dosing, not the whole-plant cannabis available at dispensaries. The assumption that dispensary products will produce identical results is common but unproven. For a deeper exploration of the pain research specifically, see cannabis and chronic pain research.
Chemotherapy-Induced Nausea and Vomiting
This is one of the oldest and most established medical uses of cannabinoids. The same Whiting 2015 meta-analysis found moderate-quality evidence that cannabinoids reduce nausea and vomiting associated with chemotherapy. This application has been recognized since the 1980s and led to the FDA approval of two synthetic cannabinoid medications: dronabinol (brand name Marinol) and nabilone (brand name Cesamet).
Both medications mimic THC. They were developed specifically because THC's antiemetic (anti-nausea) properties were well-documented in early clinical research. Patients who did not respond to standard anti-nausea medications sometimes responded to these cannabinoid alternatives. The evidence here is among the most consistent in the entire medical cannabis literature. For a closer look at how cannabinoids work specifically for chemotherapy patients, see cannabis for chemo nausea.
Spasticity in Multiple Sclerosis
Spasticity refers to involuntary muscle tightness and spasms, commonly experienced by people with multiple sclerosis (MS). The Whiting 2015 review found moderate-quality evidence that cannabinoids, particularly nabiximols (a pharmaceutical spray containing both THC and CBD, marketed as Sativex in some countries), reduce patient-reported spasticity.
The evidence is stronger for patient-reported improvement than for objective measurement. In other words, patients consistently report feeling less stiff and having fewer spasms, but the improvement does not always show up on clinical spasticity scales. This discrepancy could mean that cannabinoids improve the subjective experience of spasticity (which matters enormously to patients) without dramatically changing the underlying muscle tone. Nabiximols is approved for MS spasticity in over 25 countries, though not in the United States. For a detailed look at the clinical evidence behind Sativex and spasticity outcomes, see cannabis and multiple sclerosis spasticity.
Conditions With Moderate or Emerging Evidence
Epilepsy (Specific Syndromes)
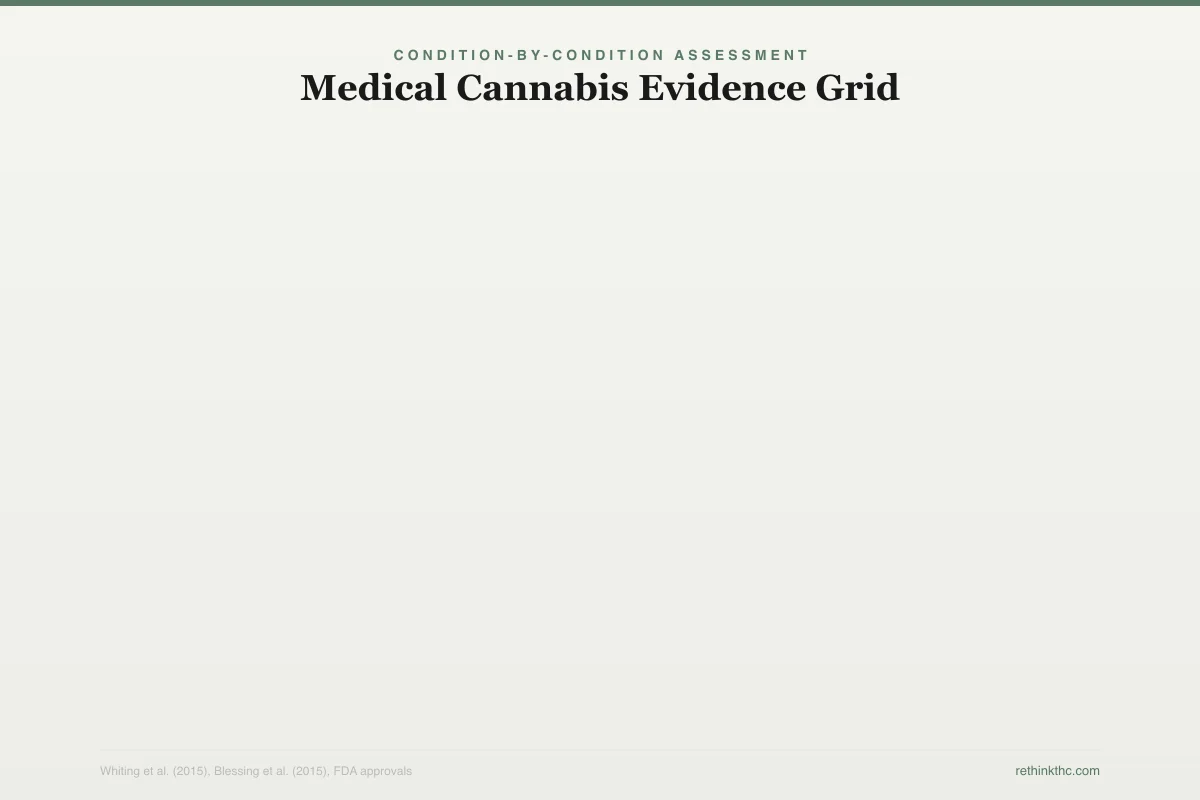
The grid below maps how the evidence stacks up across conditions and product types.
Condition-by-Condition Assessment
Medical Cannabis Evidence Grid
Evidence quality varies enormously by condition
Chronic Neuropathic Pain
Multiple RCTs, 2015 JAMA meta-analysis
Chemo Nausea/Vomiting
FDA-approved (dronabinol, nabilone)
MS Spasticity
Sativex approved in 25+ countries
Epilepsy (CBD)
FDA-approved Epidiolex for Dravet/LGS
Anxiety (CBD)
Promising preclinical, limited RCTs
Sleep Disorders
Mixed results, mostly secondary outcomes
Appetite/Cachexia
FDA-approved for AIDS wasting
PTSD
Reduced nightmares with nabilone, small studies
Glaucoma
Short-lived effect, outdated approach
Inflammation/IBD
Observational data, mixed RCT results
In 2018, the FDA approved Epidiolex, a purified CBD (cannabidiol) medication, for two rare and severe forms of childhood epilepsy: Dravet syndrome and Lennox-Gastaut syndrome. This was a significant milestone because Epidiolex is derived from the cannabis plant (not synthesized) and was approved through the standard FDA drug approval process, including large randomized controlled trials. A 2022 meta-analysis confirmed significant seizure reduction with CBD in these syndromes, as well as in tuberous sclerosis complex.[5]
The evidence for Epidiolex in these specific epilepsy syndromes is strong. It reduced seizure frequency significantly compared to placebo. However, this evidence applies to a specific, pharmaceutical-grade CBD product at specific doses for specific seizure disorders. It does not support the broader claim that CBD from a dispensary or supplement store will help with seizures generally. The purity, dosing, and patient population matter. The full story of how Epidiolex went from clinical trials to FDA approval is covered in cannabis and epilepsy: the Epidiolex story.
Anxiety (CBD Specifically)
A 2015 review by Blessing and colleagues, published in Neurotherapeutics, examined the preclinical and clinical evidence for CBD as a treatment for anxiety disorders.[2] The review found substantial preclinical evidence (meaning animal studies and early-phase human studies) supporting CBD's potential for generalized anxiety disorder, panic disorder, social anxiety disorder, obsessive-compulsive disorder, and PTSD.
The word "potential" is doing significant work in that sentence. The preclinical evidence is genuinely promising. CBD appears to modulate serotonin signaling and reduce amygdala reactivity in ways that are relevant to anxiety. But the clinical trial evidence in humans is still limited to small studies with short follow-up periods. We do not yet have the large, long-term randomized trials needed to make definitive claims about CBD for anxiety.
It is also critical to distinguish CBD from THC in this context. THC, particularly at higher doses, can increase anxiety rather than reduce it. The relationship between cannabis and anxiety is dose-dependent, cannabinoid-dependent, and individual-dependent. For a detailed look at what the clinical evidence actually shows, see does CBD work for anxiety?. For more on the broader relationship between cannabis and anxiety, see does weed help anxiety.
Sleep
Many people use cannabis to help with sleep, and subjective reports of improved sleep onset are common. However, the Whiting 2015 meta-analysis found only low-quality evidence for cannabinoids improving sleep, and most of the sleep improvement observed in trials was a secondary outcome in studies designed to measure something else (usually pain). There are very few large, well-designed trials examining cannabinoids as a primary sleep treatment.
What research does show is that THC suppresses REM sleep (the dreaming phase of sleep).[6] For people with PTSD-related nightmares, this can be therapeutic. For everyone else, chronic REM suppression may impair memory consolidation and emotional processing. The sleep question is more complicated than "cannabis helps you sleep," and the evidence base does not yet support confident claims in either direction.
Appetite Stimulation
Dronabinol (synthetic THC) is FDA-approved for appetite stimulation in patients with AIDS-related wasting syndrome. The evidence for this specific application is established. Whether whole-plant cannabis effectively stimulates appetite in other contexts (cancer cachexia, eating disorders) is less clear from controlled research, though the subjective experience of increased appetite from THC is one of the most universally reported effects.
Conditions With Limited or Preliminary Evidence
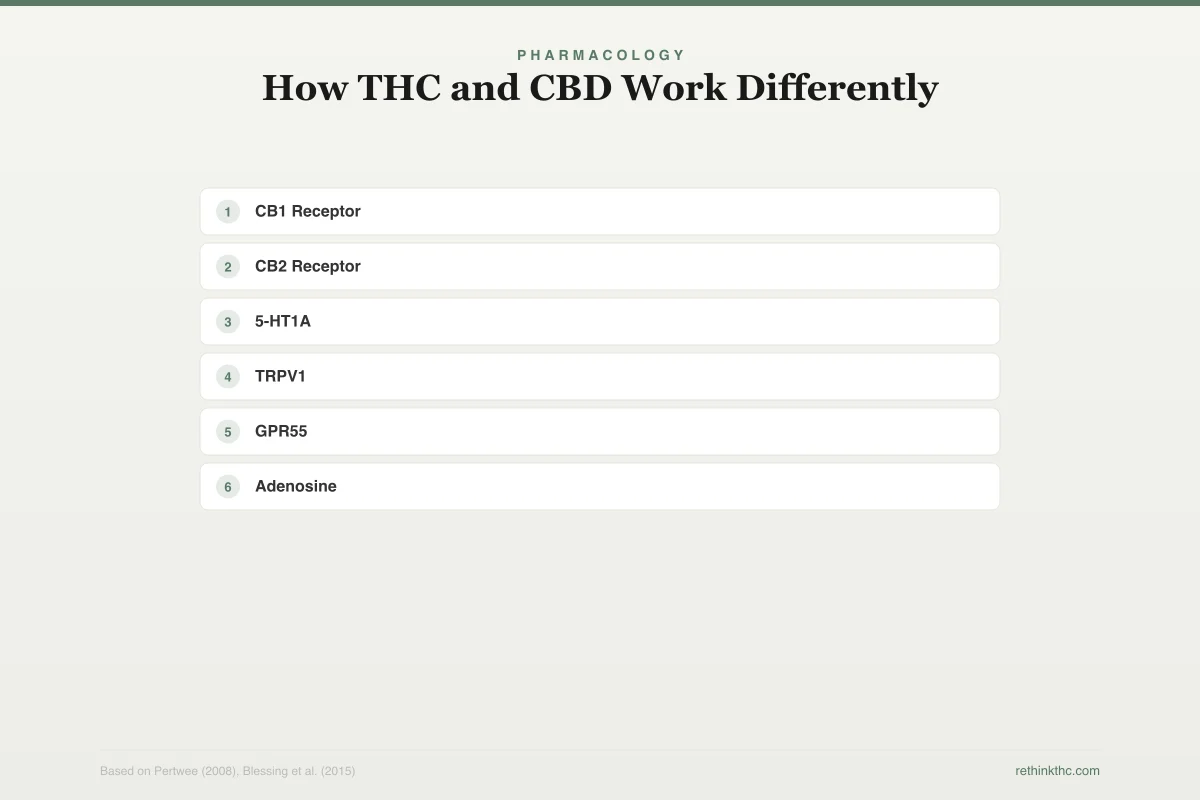
Several conditions are frequently cited in popular media as treatable with cannabis, but the evidence remains preliminary. The diagram below shows the pathways through which cannabinoids interact with your body's systems.
Pharmacology
How THC and CBD Work Differently
Two cannabinoids, distinct mechanisms of action
Direct Binding
Agonist at cannabinoid receptors
Indirect Action
Modulates multiple receptor systems
THC produces its effects by directly activating CB1 receptors -- CBD works through multiple indirect pathways, which is why it lacks psychoactive effects but has broader therapeutic potential
Inflammatory bowel disease (Crohn's disease, ulcerative colitis) has some observational data suggesting symptom relief, but randomized trials have produced mixed results. Glaucoma was one of the earliest proposed medical uses, but the intraocular pressure reduction from cannabis is short-lived (requiring dosing every few hours) and modern glaucoma medications are more effective and practical — the full history is covered in cannabis and glaucoma: the original claim revisited. Depression has almost no controlled trial evidence supporting cannabis use, and some observational data suggests cannabis may worsen depressive symptoms over time.
PTSD sits in a complicated middle ground. The most consistent finding is reduced nightmares with nabilone (a synthetic cannabinoid), but the broader evidence for cannabis as a PTSD treatment is limited by small sample sizes and methodological problems. The subjective reports of benefit are widespread, but subjective reports alone cannot establish efficacy. Tourette's syndrome has a small but intriguing evidence base, with some controlled trials suggesting THC may reduce tic frequency and severity — see cannabis and Tourette's syndrome for the full picture.
For each of these conditions, the honest summary is the same: there are reasons to continue researching, but not enough evidence to make confident clinical recommendations.
Pharmaceutical Cannabinoids vs. Whole-Plant Cannabis
This distinction is one of the most important and most frequently ignored in the medical cannabis conversation.
The three FDA-approved cannabinoid products are:
- Dronabinol (Marinol): Synthetic THC. Approved for chemotherapy nausea and AIDS wasting.
- Nabilone (Cesamet): Synthetic THC analog. Approved for chemotherapy nausea.
- Epidiolex: Plant-derived, purified CBD. Approved for Dravet and Lennox-Gastaut syndrome epilepsy.
Each of these products delivers a known quantity of a specific cannabinoid at a consistent dose. This is how all pharmaceutical drugs work. You know exactly what you are taking and how much.
Whole-plant cannabis from a dispensary is fundamentally different. It contains hundreds of compounds (THC, CBD, other cannabinoids, terpenes, flavonoids) in ratios that vary by strain, grower, harvest, and even which part of the plant was used. THC potency in commercially available cannabis has changed dramatically over time. A 2016 analysis by ElSohly and colleagues, published in Biological Psychiatry, documented that THC potency in confiscated cannabis roughly tripled between 1995 and 2014, while CBD content declined.[3]
This means the cannabis available today is a very different product from what was studied in most clinical trials. Higher THC concentrations with less CBD may produce different therapeutic effects and different risk profiles than what the research literature reflects. When someone says "studies show cannabis helps with pain," the studies usually tested a specific cannabinoid product at a specific dose, not a high-THC flower purchased from a dispensary. Understanding the difference between CBD and THC, both chemically and in terms of effects, is essential context for evaluating any medical claim. The CBD vs THC comparison breaks this down in detail. If you are considering a CBD product specifically, the CBD oil quality guide covers what to look for and what to avoid.
Understanding how your body's own cannabinoid system works provides useful context for understanding why external cannabinoids produce the effects they do. The endocannabinoid system explained simply article covers this in detail.
The Quality-of-Evidence Problem
The medical cannabis field has a structural evidence problem that affects nearly every claim made about it.
The risks of cannabis use exist alongside the potential benefits. A nationally representative survey of over 36,000 U.S. adults found that approximately 6 percent met criteria for a lifetime cannabis use disorder under DSM-5, and among people who used cannabis in the past year, roughly 30 percent met criteria for a use disorder.[7] A 2024 systematic review found that cannabis smoking was associated with elevated risk of myocardial infarction even after adjusting for tobacco use, particularly in younger users, though non-smoked cannabis was not associated with significant cardiac risk.[8] Chronic use is associated with bronchitis symptoms. These findings provide important context for evaluating any therapeutic claim.
The quality-of-evidence problem has several layers.
Federal scheduling. Cannabis remains a Schedule I substance in the United States, which has historically made it extremely difficult to conduct large, well-funded clinical trials. Researchers face regulatory barriers that do not apply to studies of other medications. This has artificially limited the evidence base.
Small sample sizes. Many cannabis studies involve fewer than 100 participants. This makes it difficult to detect real effects, increases the risk of false positives, and limits the ability to identify which patient subgroups benefit most.
Short study durations. Most clinical trials of cannabinoids last weeks to months. We have very limited data on long-term therapeutic use, long-term side effects, or how tolerance (needing increasing doses for the same effect) affects outcomes over years.
Heterogeneous products. Studies use different cannabinoid formulations, doses, routes of administration, and patient populations, making it difficult to compare results across trials or pool data meaningfully.
Publication bias. Studies with positive results are more likely to be published than studies with negative or null results, which can inflate the apparent evidence for benefit.
None of this means medical cannabis does not work. It means the evidence is not as strong as the public conversation often implies, and that honest engagement with the research requires acknowledging both what we know and what we do not yet know.
The Dependence Question
Any honest discussion of medical cannabis must acknowledge dependence risk, including the reality that cannabis can interact with other medications in ways that complicate treatment plans — a concern that is especially relevant for older adults managing multiple prescriptions. The Hasin 2016 survey estimated that approximately 6 percent of people who use cannabis will meet criteria for a lifetime use disorder.[7] Among those who use daily, rates are substantially higher — research consistently shows that frequency of use is the strongest predictor of developing a use disorder. Among those who begin using in adolescence, the risk increases further, because the developing brain is more vulnerable to THC-driven neuroadaptation. Approximately 47 percent of regular users experience clinically significant withdrawal symptoms when they stop.[9]
Safety
ModerateDependence risk is real, even for medical users
Concern
About 6% of all cannabis users develop a use disorder. Among daily users, rates are much higher. Nearly half of regular users experience withdrawal symptoms — irritability, sleep problems, anxiety, and cravings — when they stop.
What the research says
Dependence doesn't make medical cannabis inappropriate, but it means use should include monitoring. Many effective medications carry dependence risk — the key is awareness and a plan.
Particularly relevant for: Anyone using cannabis regularly, especially daily users and those who started young
What to do
Track your usage patterns. If you notice you need more to get the same effect, or you feel lousy when you skip a day, talk to a healthcare provider. Have an exit strategy before you start.
Hasin et al. (2016), Am J Psychiatry; Bahji et al. (2020), JAMA Network Open
This does not mean medical cannabis is inappropriate. Many effective medications carry dependence risks (opioids, benzodiazepines, certain sleep medications). But it means the decision to use cannabis medicinally should include awareness of this risk, monitoring for escalating use, and a plan for what happens if dependence develops. For a balanced exploration of cannabis and addiction, see is weed addictive.
What We Know and What We Do Not
What the evidence supports:
- Cannabinoids provide modest but real relief for chronic neuropathic pain
- Synthetic cannabinoids reduce chemotherapy-induced nausea effectively
- Nabiximols reduce patient-reported spasticity in MS
- Purified CBD reduces seizure frequency in specific rare epilepsy syndromes
- CBD shows preclinical promise for anxiety disorders, though large clinical trials are needed
What the evidence does not yet support:
- That whole-plant dispensary cannabis produces the same effects as pharmaceutical cannabinoids tested in clinical trials
- That cannabis is an effective primary treatment for depression, PTSD, glaucoma, or inflammatory bowel disease
- That high-THC cannabis products are therapeutic rather than recreational for most users
- That the benefits of long-term cannabis use outweigh the risks for most medical conditions
What we genuinely do not know:
- The optimal cannabinoid ratios, doses, and delivery methods for specific conditions
- The long-term effects of medical cannabis use over years or decades
- Whether the entourage effect (the idea that whole-plant cannabis works better than isolated cannabinoids) is real and clinically meaningful
- How individual genetic variation affects who benefits and who is harmed
The Honest Position
Cannabis is neither a miracle drug nor a dangerous substance with no medical value. The truth, as usual, is more nuanced and less satisfying than either extreme.
Some people with chronic pain, treatment-resistant nausea, MS spasticity, or rare epilepsy syndromes have genuinely benefited from cannabinoid medications. The evidence for these applications is real, if imperfect. Other claims about medical cannabis are running far ahead of the evidence. And the gap between pharmaceutical cannabinoids studied in clinical trials and the high-THC products sold at dispensaries is large enough that conflating the two is genuinely misleading.
The most useful approach is the same one that applies to any medical treatment: look at the evidence for your specific condition, understand the quality of that evidence, weigh the known benefits against the known risks, discuss it honestly with a healthcare provider, and be willing to adjust course based on your actual experience rather than your hopes or expectations. If you are planning any surgical procedure, be aware that cannabis use affects anesthesia and recovery — see quitting weed before surgery for what your surgical team needs to know. And if you are pregnant or considering pregnancy, the evidence strongly favors stopping — both during pregnancy itself and while breastfeeding.
When to Seek Professional Help
If you are considering cannabis for a medical condition, talk to a healthcare provider who is knowledgeable about cannabinoid medicine. If you are currently using cannabis medicinally and are concerned about dependence, escalating use, or diminishing benefits, that is also worth a clinical conversation.
If you or someone you know is struggling with cannabis dependence, the SAMHSA National Helpline is available 24/7 at 1-800-662-4357. It is free, confidential, and provides referrals to local treatment facilities, support groups, and community-based organizations.
The Bottom Line
Cannabis has real medical uses for a handful of specific conditions — chronic neuropathic pain, chemotherapy nausea, MS spasticity, and rare forms of epilepsy. The evidence for those is moderate, and it comes mostly from pharmaceutical cannabinoid products with controlled dosing, not from the flower or edibles available at a dispensary. For most other conditions people use cannabis for — anxiety, sleep, depression, PTSD — the clinical evidence is preliminary at best. Medical use does not eliminate the risk of dependence, and the gap between what the research supports and what the market claims remains wide. Being honest about that gap is more useful than either dismissing or overstating cannabis as medicine.
Sources & References
- 1RTHC-01077·Whiting, Penny F. et al. (2015). “The Most Comprehensive Review of Medical Cannabis Evidence Found Modest Benefits for Pain, Spasticity, and Nausea.” JAMA.Study breakdown →PubMed →↩
- 2RTHC-00924·Blessing, Esther M. et al. (2015). “CBD and Anxiety in 2015: Promising Signals, Mostly From Single Doses.” Neurotherapeutics.Study breakdown →PubMed →↩
- 3RTHC-01144·ElSohly, Mahmoud A. et al. (2016). “U.S. Cannabis Potency Tripled Over Two Decades While CBD Nearly Vanished.” Biological Psychiatry.Study breakdown →PubMed →↩
- 4RTHC-03713·Bilbao, Ainhoa et al. (2022). “Major meta-analysis of 152 RCTs finds cannabinoid effectiveness varies dramatically by specific drug and condition.” BMC medicine.Study breakdown →PubMed →↩
- 5RTHC-04223·Silvinato, Antônio et al. (2022). “Meta-analysis confirmed CBD reduces seizures by 33% in treatment-resistant epilepsy.” Revista da Associacao Medica Brasileira (1992).Study breakdown →PubMed →↩
- 6RTHC-01161·Gates, Peter et al. (2016). “Systematic Review Confirms Cannabis Withdrawal Disrupts Sleep, but Specific Mechanisms Remain Unclear.” Substance abuse.Study breakdown →PubMed →↩
- 7RTHC-01172·Hasin, Deborah S et al. (2016). “National Survey Finds 2.5% of US Adults Had Cannabis Use Disorder in the Past Year, and Most Never Got Treatment.” The American journal of psychiatry.Study breakdown →PubMed →↩
- 8RTHC-05775·van Amsterdam, Jan et al. (2024). “Cannabis Smoking Is an Independent Risk Factor for Heart Attack, but Edibles May Not Be.” Journal of clinical medicine.Study breakdown →PubMed →↩
- 9RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩