Cannabis for Chronic Pain: What the Research Actually Supports
Balanced Cannabis Science
6,462 Patients
A 2015 JAMA review of 79 randomized controlled trials found moderate evidence that cannabinoids help with chronic pain, but effect sizes were modest and most studies used pharmaceutical-grade products unlike what dispensaries sell.
Whiting et al., JAMA, 2015
Whiting et al., JAMA, 2015
View as imageIf you only read one thing
Cannabis can help with some chronic pain, but not the kinds most people assume. The best evidence is for nerve pain — things like diabetic neuropathy or pain after shingles. For headaches, back pain, and general inflammation, the research is weak. The biggest catch: most studies used pharmaceutical-grade cannabinoids at precise doses, not what you'd buy at a dispensary. And tolerance builds, so the same dose stops working over months of daily use.
Chronic pain affects roughly 20% of adults worldwide, and for many of them, conventional treatments are either inadequate or come with side effects that erode quality of life. Opioids carry addiction and overdose risks. NSAIDs damage the gut and kidneys over time. Physical therapy helps but does not eliminate pain for everyone. Against this backdrop, it makes sense that millions of people have turned to cannabis as an alternative.
The question is not whether people are using cannabis for pain. They are, in enormous numbers. The question is what the research actually supports, where the evidence is strong, where it is weak, and what you should know before making a decision about your own pain management.
Key Takeaways
- Chronic pain is the most commonly cited reason for medical cannabis use, and a 2015 JAMA review of 79 randomized controlled trials found moderate evidence that cannabinoids help with chronic pain
- The strongest evidence is for neuropathic pain (nerve pain) and cancer-related pain, while evidence for headaches, acute pain, and inflammatory conditions is still weak
- THC and CBD work differently for pain, and whole-plant cannabis is not the same as the pharmaceutical cannabinoids used in most clinical trials
- Effective doses vary widely between people, and the tolerance that builds with regular THC use means the same dose stops working over time
- Most cannabis pain studies are small, short-term, and use pharmaceutical-grade products that look very different from what you can get at a dispensary
- Tolerance to THC-based pain relief builds over weeks to months of daily use — so the same dose stops working and increasing it raises both side effects and dependence risk
How the Endocannabinoid System Processes Pain
Your body has a built-in system called the endocannabinoid system (ECS) that plays a direct role in how you experience and regulate pain. This is not a peripheral system. It is one of the core mechanisms through which your body modulates pain signals.
Condition-by-Condition
Cannabis for Pain: Evidence by Condition
Not all chronic pain responds equally to cannabinoids
Neuropathic Pain
Multiple RCTs, NNT = 5.6 (1 in 6 patients benefits)
MS Spasticity Pain
Sativex approved in 25+ countries for spasticity
Cancer Pain
Limited RCTs, modest benefit as add-on to opioids
Fibromyalgia
Observational data only, no strong RCT evidence
Arthritis
CB2 rationale exists, clinical data insufficient
Migraines
Widespread anecdotal use, minimal controlled research
Acute / Surgical Pain
Not effective — variable onset, impractical for acute use
Lu and Mackie published a comprehensive review of the endocannabinoid system in 2016 in Biological Psychiatry.[2] The review documented that the ECS includes two primary receptors, CB1 and CB2, along with endogenous cannabinoids (your body's own cannabis-like molecules) called anandamide and 2-AG. CB1 receptors are concentrated in the brain and spinal cord. CB2 receptors are found primarily in immune cells and peripheral tissues.
Both receptor types are involved in pain processing. CB1 receptors modulate how pain signals travel through the central nervous system. CB2 receptors influence inflammatory responses at the site of injury or disease. When you stub your toe and the initial sharp pain fades to a dull ache over minutes, your endocannabinoid system is part of what makes that happen.
Cannabis introduces external cannabinoids, primarily THC and CBD, that interact with these same receptors. THC binds directly to CB1 receptors, which is why it produces psychoactive effects along with pain modulation. CBD works through more indirect mechanisms, influencing endocannabinoid tone without producing a high.
The logic behind cannabis for pain is grounded in real biology. The question is whether introducing external cannabinoids actually produces clinically meaningful pain relief that justifies the risks, and whether it does so consistently enough to be considered a reliable treatment. A more detailed look at how the endocannabinoid system functions and adapts is covered in endocannabinoid system and withdrawal.
What the Largest Review Found
The most comprehensive review of cannabinoids for medical use was published in 2015 by Whiting and colleagues in JAMA.[1] This was not a single study. It was a systematic review and meta-analysis of 79 randomized controlled trials involving 6,462 participants.
The review examined cannabinoids for a range of medical conditions, including chronic pain, nausea and vomiting from chemotherapy, spasticity in multiple sclerosis, and several others. For chronic pain specifically, the findings were notable but measured.
The review found moderate-quality evidence that cannabinoids were associated with a greater reduction in chronic pain compared to placebo. The average number of patients reporting at least a 30% reduction in pain was greater in the cannabinoid groups than in the placebo groups.
However, several important caveats accompany this finding. The effect sizes were modest, meaning cannabinoids reduced pain somewhat but did not eliminate it for most people. The studies used pharmaceutical-grade cannabinoids with controlled dosing, not dispensary products. And the evidence quality was rated "moderate" rather than "high," reflecting limitations in study design, sample size, and duration.
This is the best evidence we have, and it supports a cautious conclusion: cannabinoids can reduce chronic pain for some people, but the effect is moderate and the evidence base has real limitations.
Evidence Review
Cannabis for pain: where the evidence is strong vs. weak
Source: Whiting et al. (2015), JAMA — 79 RCTs, 6,462 patients
 View as image
View as image| Pain Condition | Evidence Quality | Key Finding | Product Studied |
|---|---|---|---|
| Neuropathic pain | Moderate | Consistent benefit across multiple trials | Nabiximols, dronabinol, smoked cannabis |
| Cancer-related pain | Moderate | Modest additional benefit as adjunct to opioids | Nabiximols, dronabinol |
| MS spasticity | Moderate | Patient-reported improvement in tightness and spasms | Nabiximols (1:1 THC:CBD) |
| Fibromyalgia | Low | Inconsistent results, small studies only | Various |
| Headaches/migraines | Very low | Minimal controlled data despite anecdotal reports | Various |
| Acute pain | Very low | No consistent benefit over placebo | Dronabinol, smoked cannabis |
| Inflammatory conditions | Low | Theoretical basis from CB2 receptors, limited clinical data | Various |
Where the Evidence Is Strongest
Not all chronic pain responds the same way to cannabinoids. The research suggests that certain types of pain show more consistent benefit than others.
Pain Modulation
How Cannabis Modulates Pain Signals
Cannabinoids intervene at four points along the ascending pain pathway
Peripheral Nerves
Injury siteCB1 & CB2 receptors reduce pain signals at the source of tissue damage or inflammation
CB1 + CB2Spinal Cord
Dorsal hornCB1 receptors modulate pain signal transmission before it reaches the brain
CB1Brain — Thalamus
Pain perceptionAlters how pain signals are processed and perceived — reduces intensity
CB1Brain — Limbic System
Emotional responseChanges the emotional dimension of pain — "pain is there but doesn't bother me"
CB1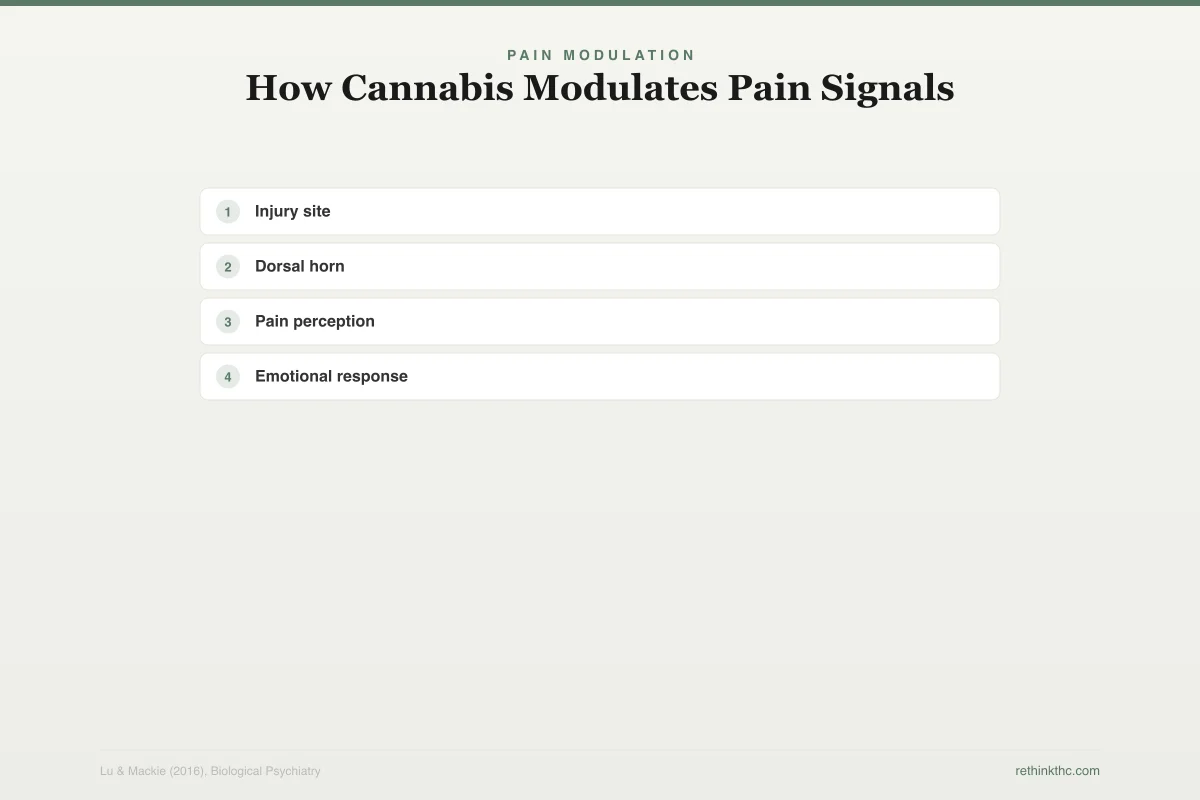
Neuropathic Pain
Neuropathic pain, which results from damage to the nervous system itself (as seen in diabetic neuropathy, HIV-associated neuropathy, postherpetic neuralgia, and some spinal cord injuries), is the pain category with the most consistent evidence for cannabinoid benefit. The Whiting 2015 review found that the evidence for neuropathic pain was among the strongest across all pain types examined.
This makes biological sense. Neuropathic pain involves dysfunctional signaling in the central and peripheral nervous systems, and CB1 receptors are heavily concentrated along these pain pathways. Modulating CB1 activity with cannabinoids has a plausible mechanism for reducing the abnormal pain signals that characterize neuropathic conditions.
Cancer-Related Pain
Cancer pain is another area where cannabinoids have shown promise, particularly as an adjunct (add-on) to existing pain management rather than a standalone treatment. Several studies included in the Whiting review examined cannabinoids for cancer pain that was not adequately controlled by opioids alone. The results suggested modest additional benefit when cannabinoids were added to existing pain regimens. For a focused look at how cannabinoids apply specifically to cancer pain beyond the nausea context, see cannabis and cancer pain.
MS Spasticity
While not strictly a "pain" condition, spasticity in multiple sclerosis (involuntary muscle tightness and spasms) causes significant discomfort and functional impairment. The Whiting review found moderate evidence supporting nabiximols (a pharmaceutical spray containing THC and CBD in a 1:1 ratio) for MS-related spasticity. This is one of the few areas where a specific cannabinoid product has regulatory approval in multiple countries.
Where the Evidence Is Weak
Acute Pain
Cannabis is not well-suited for acute pain management. The onset time, variable dosing, and psychoactive effects make it impractical for situations like postoperative pain or injury. The existing studies on cannabinoids for acute pain have not shown consistent benefit, and in some cases, cannabinoid groups performed no better than placebo.
Headaches and Migraines
Despite widespread anecdotal reports that cannabis helps with headaches, the controlled research is minimal. The few studies that exist are small, methodologically limited, and do not support confident conclusions. The Whiting review did not find sufficient evidence to support cannabinoids for headache disorders.
Inflammatory Pain Conditions
For conditions like rheumatoid arthritis, fibromyalgia, and inflammatory bowel disease, the evidence is early-stage and inconsistent. While CB2 receptors are involved in immune and inflammatory responses (which provides a theoretical basis), the clinical trial data has not yet demonstrated reliable benefit. Some patients report improvement, but the controlled evidence remains insufficient to draw firm conclusions.
Whole-Plant Cannabis vs. Pharmaceutical Cannabinoids
Here is a critical distinction that gets lost in most conversations about cannabis and pain. The vast majority of the studies in the Whiting review used pharmaceutical cannabinoids (dronabinol, nabilone, or nabiximols), not the cannabis flower, edibles, or vape products available at dispensaries.
Risk-Benefit Comparison
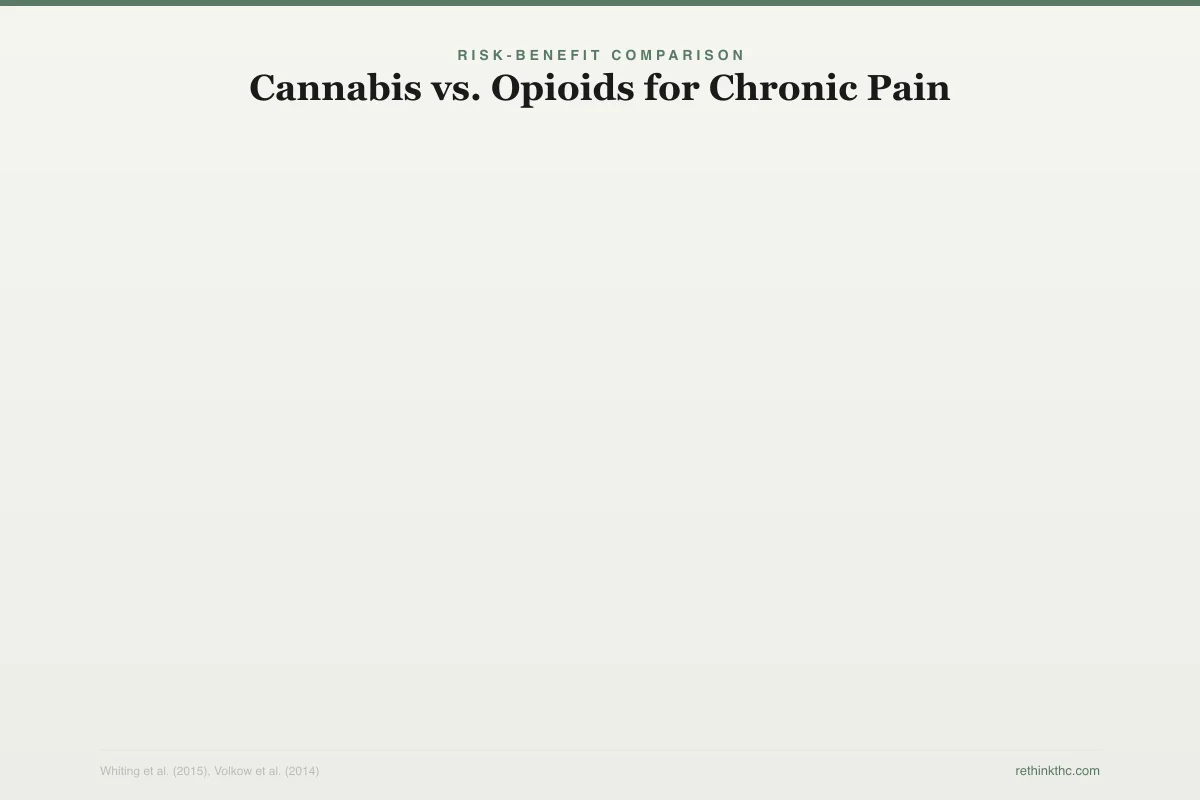
Cannabis vs. Opioids for Chronic Pain
Different risk profiles, different trade-offs
Pain Efficacy (Chronic)
Moderate
High (short-term)
Addiction Potential
Low–moderate (~9%)
High (~25-30%)
Fatal Overdose Risk
None documented
High (80K+ deaths/yr US)
Tolerance Development
Yes (weeks–months)
Yes (days–weeks)
Cognitive Side Effects
Memory, attention
Sedation, confusion
Serious Medical Risks
Psychiatric (anxiety, psychosis risk)
Respiratory depression, constipation
Cannabis carries lower acute danger but is not a direct replacement — efficacy is moderate, and tolerance still develops over time
This matters for several reasons.
Consistency. Pharmaceutical cannabinoids deliver a precise, reproducible dose. Dispensary products vary in potency, cannabinoid ratios, terpene profiles, and actual content (which may differ from what the label says).
Composition. Most pain studies used either pure THC, pure CBD, or a specific THC-to-CBD ratio. Dispensary products often contain dozens of cannabinoids and terpenes in varying proportions.
Administration route. Many studies used oral or sublingual (under the tongue) delivery, which produces different absorption kinetics than smoking or vaping.
When someone says "the research supports cannabis for chronic pain," what the research actually supports is specific pharmaceutical cannabinoids at controlled doses for specific types of pain. Extrapolating from those findings to "I should buy an edible at the dispensary for my back pain" involves several assumptions that may or may not hold up.
THC vs. CBD for Pain
THC and CBD contribute to pain management through different mechanisms, and understanding the distinction matters for making informed choices.
THC works primarily by binding to CB1 receptors in the central nervous system. It can reduce pain perception, but it also produces psychoactive effects, impairs cognition and motor function, and carries risks of tolerance, dependence, and addiction. Higher doses do not necessarily mean better pain relief, and the side effects (dizziness, sedation, anxiety, cognitive impairment) increase with dose.
CBD does not bind directly to CB1 receptors in the same way and does not produce a high. It appears to work through multiple mechanisms, including modulating endocannabinoid tone, interacting with serotonin receptors, and influencing inflammatory pathways. The evidence for CBD as a standalone pain treatment is still developing, but it does not carry the same dependence or cognitive impairment risks as THC.
The Whiting 2015 review found that products combining THC and CBD (like nabiximols) showed benefit for certain conditions, which suggests that the interaction between the two compounds may be important. This aligns with the "entourage effect" hypothesis, the idea that cannabis compounds work better together than in isolation, though this hypothesis remains debated.
The Dosing Challenge
One of the most significant practical problems with cannabis for pain is dosing. Unlike conventional medications where a doctor can prescribe a specific milligram dose based on established guidelines, cannabis dosing is highly variable and poorly standardized.
Dosing Protocol
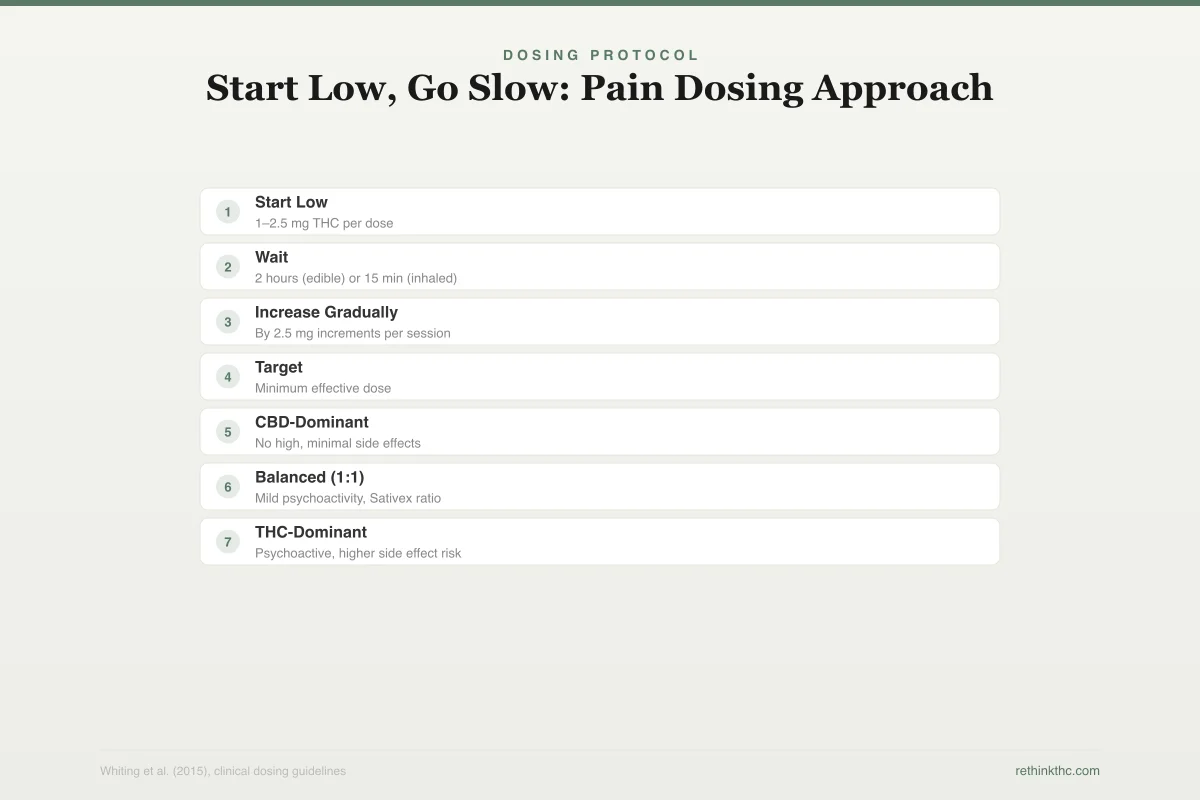
Start Low, Go Slow: Pain Dosing Approach
The evidence-based titration strategy for chronic pain
Start Low
1–2.5 mg THC per doseBegin at the lowest available dose to assess tolerance
Wait
2 hours (edible) or 15 min (inhaled)Edibles take much longer to peak — do not re-dose early
Increase Gradually
By 2.5 mg increments per sessionOnly increase if prior dose was insufficient and tolerated
Target
Minimum effective doseMore is not better — higher doses increase side effects without proportional pain relief
Product Type by Pain Condition
Best for: Inflammation, mild pain
No high, minimal side effects
Best for: General chronic pain
Mild psychoactivity, Sativex ratio
Best for: Neuropathic pain
Psychoactive, higher side effect risk
Effective doses for pain relief differ enormously between individuals based on tolerance, body weight, genetics, the type of pain, the route of administration, and the specific product being used. There is no equivalent of "take 400mg of ibuprofen every 6 hours" for cannabis. What provides relief for one person may do nothing for another or produce intolerable side effects in a third.
This makes titration (starting low and gradually increasing until you find the right dose) essential but also impractical for many people. Without guidance, people tend to either underdose (and conclude cannabis does not work) or overdose (and experience anxiety, cognitive impairment, or other side effects that make them stop).
Risks and Side Effects
Volkow and colleagues published a comprehensive review of the adverse health effects of marijuana in 2014 in the New England Journal of Medicine. The review documented several risks that are relevant to anyone considering cannabis for chronic pain.
Cognitive impairment. Regular cannabis use impairs memory, attention, and executive function. For chronic pain patients who need to work, drive, or manage daily responsibilities, this impairment is a significant cost.
Dependence. Approximately 9% of people who use cannabis develop dependence (rising to roughly 17% among those who start in adolescence and 25-50% among daily users). Chronic pain patients who use daily are in the highest-risk category. Dependence means withdrawal symptoms when you stop, which creates another problem layered on top of the original pain.
Tolerance. The dose that provides pain relief in month one may not work in month six. Tolerance drives dose escalation, which increases side effects and dependence risk. This is a fundamental limitation of THC-based pain management that does not get enough attention.
Respiratory effects. Smoked cannabis exposes the lungs to combustion byproducts. For chronic pain patients who plan to use cannabis long-term, the route of administration matters, and smoking is the worst option from a respiratory standpoint. For a system-by-system breakdown of how cannabis affects your physical health beyond pain, see cannabis and your body.
Mental health effects. Cannabis use is associated with increased risk of anxiety, depression, and, in vulnerable individuals, psychotic symptoms. For chronic pain patients who already face elevated rates of depression and anxiety, this is a meaningful consideration.
Safety
ModerateDaily THC use for pain carries real dependence risk
Concern
Chronic pain patients who use THC daily are in the highest-risk category for cannabis dependence. Approximately 25–50% of daily users develop dependence. Tolerance means the dose that works in month one may not work in month six, driving escalation.
What the research says
Consider CBD-dominant products (lower dependence risk), plan tolerance breaks, use the lowest effective dose, and work with a provider who can monitor for dose creep and dependence signs.
Particularly relevant for: Anyone considering daily cannabis use for chronic pain
What to do
Track your dose weekly. If you're increasing more than once per month, tolerance is winning. Discuss rotation strategies or tolerance breaks with your provider before dependence sets in.
Volkow et al. (2014), NEJM; Whiting et al. (2015), JAMA
For a broader overview of what research supports across all medical cannabis applications, see medical benefits of cannabis.
The Evidence Quality Problem
This is the part of the conversation that requires the most honesty. The evidence for cannabis and chronic pain, while real, has significant quality limitations.
Most studies are small. Sample sizes of 20 to 100 participants are common, which limits the statistical power to detect real effects and makes it harder to identify subgroups that benefit most.
Most studies are short-term. Many last weeks to months, while chronic pain is a condition measured in years and decades. We do not have good data on whether cannabinoid pain relief persists over years of use, especially as tolerance develops.
Many studies use pharmaceutical-grade products. As discussed, these do not directly translate to commercially available cannabis.
Blinding is difficult. THC produces a noticeable high, which means participants often know whether they received the active treatment or placebo. This can inflate the apparent benefit.
Publication bias exists. Studies with positive results are more likely to be published than studies with negative or null results, which can make the overall evidence look more favorable than it truly is.
None of this means the evidence is worthless. The Whiting review was rigorous and transparent about these limitations. But it does mean that confidence in the findings should be proportional to the evidence quality, which is moderate, not high.
What Patients Should Consider Before Trying Cannabis for Pain
If you are considering cannabis for chronic pain management, here are the factors that matter most based on the current evidence.
What type of pain do you have? The evidence is strongest for neuropathic pain and cancer-related pain. If your pain is neuropathic in origin, the biological rationale and clinical data are more supportive. If you have acute pain, headaches, or generalized inflammatory pain, the evidence is substantially weaker.
Have you tried first-line treatments? Cannabis should not be the first thing you try. Physical therapy, cognitive behavioral therapy for pain, NSAIDs, nerve blocks, and other established treatments have stronger evidence and should be tried first or alongside cannabis.
How will you manage tolerance? If THC-based products stop working for pain over time (which tolerance predicts), what is your plan? Dose escalation carries increasing risks. Planned tolerance breaks may help but leave you without pain management during the break.
What product and route are you considering? Oral or sublingual products provide more consistent dosing than smoked or vaped cannabis. Products with CBD may carry fewer risks than THC-dominant products. High-potency THC concentrates are the furthest from what was studied in clinical trials.
Are you at risk for dependence? Daily use of THC for pain puts you in the highest-risk category for cannabis dependence. If you have a history of substance use problems, or if you find yourself escalating dose and frequency, this risk deserves serious consideration.
What is your provider's role? Managing chronic pain with cannabis works better with medical oversight than without it. A provider can help with dosing, monitor for side effects, track whether the pain relief is holding or eroding, and integrate cannabis with other treatments.
A Balanced Conclusion
The research on cannabis for chronic pain supports a middle position. It is neither the miracle painkiller that some advocacy groups claim nor the ineffective, dangerous substance that some critics suggest. The evidence shows moderate benefit for specific types of pain, primarily neuropathic, with pharmaceutical-grade cannabinoids at controlled doses.
For many people with chronic pain, cannabis represents one option in a toolkit that should include multiple approaches. It is not a replacement for physical therapy, psychological pain management, or other evidence-based treatments. It may have a role as an adjunct, particularly for neuropathic pain that has not responded adequately to first-line treatments.
The honest state of the science is that we need larger, longer, better-designed studies using the actual products people are buying. Until those exist, decisions about cannabis for pain should be made carefully, with realistic expectations, medical guidance, and an understanding of both the potential benefits and the real risks.
When to Seek Professional Help
Chronic pain is a medical condition that deserves professional management. If you are currently managing pain primarily with cannabis and have not worked with a pain specialist, that is a step worth taking. If your cannabis use for pain has escalated significantly, if you are experiencing dependence symptoms, or if pain is severely limiting your daily functioning, talk to a healthcare provider.
If you are struggling with cannabis dependence or any substance use concerns, SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
The Bottom Line
A 2015 JAMA systematic review of 79 randomized controlled trials found moderate-quality evidence that cannabinoids reduce chronic pain, with the strongest results for neuropathic pain, cancer-related pain, and MS spasticity. However, most studies used pharmaceutical-grade cannabinoids with controlled dosing, not dispensary products, and effect sizes were modest. THC reduces pain perception through CB1 receptors but carries dependence, tolerance, and cognitive impairment risks. CBD works through indirect mechanisms without producing a high. Tolerance to THC-based pain relief develops over weeks to months, driving dose escalation. Evidence for headaches, acute pain, and inflammatory conditions remains weak. The honest conclusion is that cannabinoids can help some people with specific types of chronic pain, but the effect is moderate and decisions should involve medical guidance, realistic expectations, and awareness of risks.
Sources & References
- 1RTHC-01077·Whiting, Penny F. et al. (2015). “The Most Comprehensive Review of Medical Cannabis Evidence Found Modest Benefits for Pain, Spasticity, and Nausea.” JAMA.Study breakdown →PubMed →↩
- 2RTHC-01218·Lu, Hui-Chen et al. (2016). “Your Brain Already Makes Its Own Cannabinoids. Here's How the System Works..” Biological Psychiatry.Study breakdown →PubMed →↩
- 3RTHC-01144·ElSohly, Mahmoud A. et al. (2016). “U.S. Cannabis Potency Tripled Over Two Decades While CBD Nearly Vanished.” Biological Psychiatry.Study breakdown →PubMed →↩