Cannabis and Your Body: What the Research Actually Shows
Body / Physical
183M Patients
A 183-million-patient meta-analysis found no significant link between cannabis and heart attack or stroke in the general population, but the acute cardiovascular stress during each session is real and measurable.
Theerasuwipakorn et al., Systematic Review and Meta-Analysis, 2023
Theerasuwipakorn et al., Systematic Review and Meta-Analysis, 2023
View as imageIf you only read one thing
Cannabis affects almost every system in your body — heart, lungs, hormones, appetite, immune system. But the biggest study ever done (183 million patients) found no clear link to heart attacks. Smoking it irritates your lungs but doesn't cause cancer the way tobacco does. It messes with your hormones and fertility, but those effects mostly reverse when you stop. The real answer isn't 'safe' or 'dangerous' — it depends on how you use it, how much, and what your body is already dealing with.
Cannabis does things to your body. That sentence is not controversial. What those things are, how much they matter, and whether they add up to serious harm or manageable risk is where the conversation gets complicated. The physical health effects of cannabis span your cardiovascular system, your lungs, your hormones, your metabolism, your immune function, and your reproductive system. Some of these effects are well-documented. Others are still being mapped.
This article walks through what research actually shows about cannabis and your physical health, system by system. The goal is not to tell you cannabis is safe or dangerous. It is to give you the information you need to make decisions that account for what science currently knows and, just as importantly, what it does not.
If you want to understand why cannabis affects your body in the first place, it helps to start with the endocannabinoid system, the body-wide signaling network that THC plugs into. Every physical effect discussed below traces back to how THC and other cannabinoids interact with that system.
Key Takeaways
- A 2023 meta-analysis of 20 studies and 183 million patients found that cannabis was NOT significantly linked to heart attack or stroke in the general population — though the acute stress on your heart during each session is real and measurable
- Smoked cannabis produces many of the same lung irritants as tobacco smoke, but large-scale studies have not found the same strong connection to lung cancer or COPD that tobacco carries
- THC triggers hunger by activating CB1 receptors in the part of your brain that controls appetite — yet chronic users paradoxically tend to have lower BMI in population studies despite the munchies
- Cannabis affects testosterone, estrogen, cortisol, and fertility markers — though most hormonal effects appear to reverse after you stop, based on what research shows so far
- How cannabis affects your body depends heavily on how you consume it, how much, how often, and your individual biology — which is why blanket statements about safety or harm are misleading
- Women build tolerance faster, report worse withdrawal, and store THC longer because of higher body fat — while men show more consistent effects on sperm count and motility
Cardiovascular Effects: What Your Heart Actually Goes Through
Every time you use cannabis, your cardiovascular system responds. THC activates the sympathetic nervous system, your body's fight-or-flight response, producing a measurable increase in heart rate. Most users experience an increase of 20 to 50 beats per minute, though some studies have documented increases as high as 100%. This effect typically peaks within 15 to 30 minutes and resolves over the next 1 to 3 hours.
Cannabis & Your Body
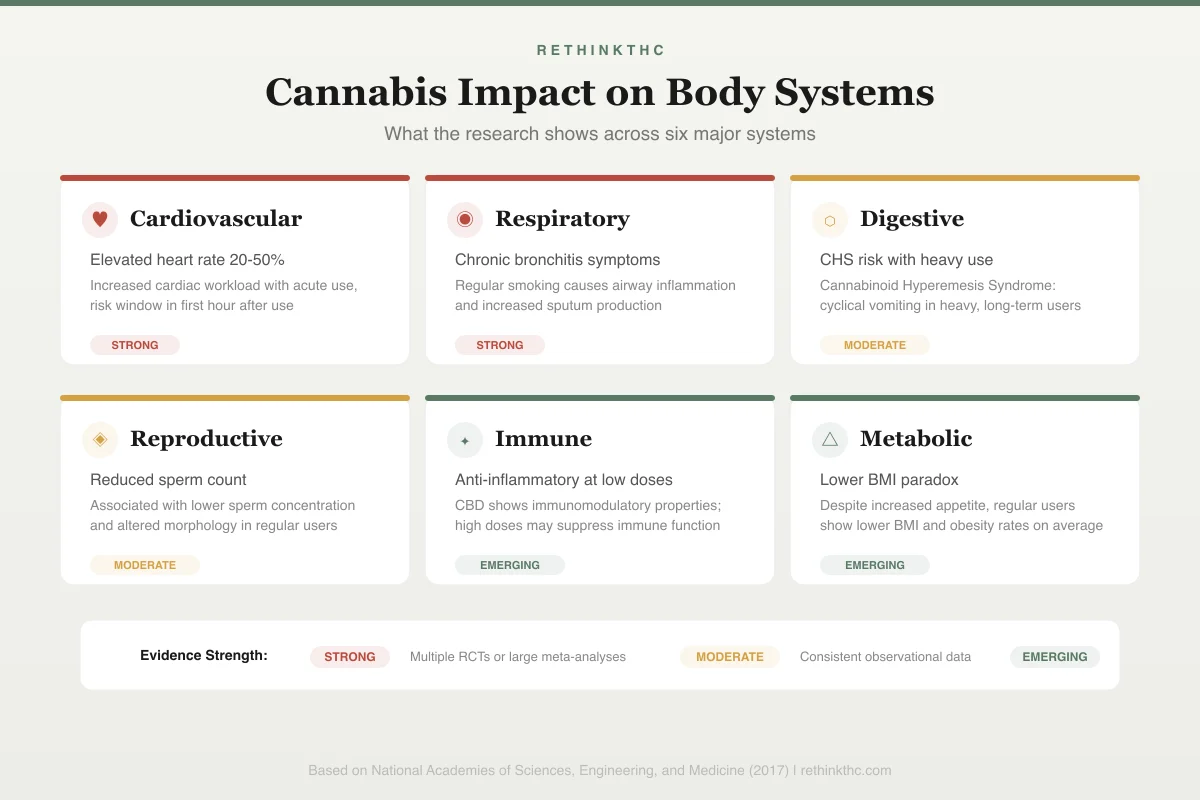
Impact on Body Systems
Cardiovascular
Elevated heart rate 20-50%
Increased cardiac workload with acute use, risk window in first hour
Strong evidenceRespiratory
Chronic bronchitis symptoms
Regular smoking causes airway inflammation and increased sputum
Strong evidenceDigestive
CHS risk with heavy use
Cannabinoid Hyperemesis Syndrome: cyclical vomiting in heavy users
Moderate evidenceReproductive
Reduced sperm count
Lower sperm concentration and altered morphology in regular users
Moderate evidenceImmune
Anti-inflammatory at low doses
CBD shows immunomodulatory properties; high doses may suppress
Emerging evidenceMetabolic
Lower BMI paradox
Despite increased appetite, regular users show lower BMI on average
Emerging evidenceBlood pressure follows a more complicated pattern. It may rise slightly while sitting and drop when standing, a phenomenon called orthostatic hypotension. This is why some people feel dizzy or lightheaded after using cannabis, particularly when they stand up quickly. Tolerance develops to these acute cardiovascular effects with regular use, so daily users typically experience less dramatic heart rate changes than occasional users.
The bigger question is whether these repeated cardiovascular fluctuations translate into long-term risk. A 2014 review by Volkow and colleagues, published in the New England Journal of Medicine, noted that the risk of heart attack appeared elevated during the first hour after cannabis use. The proposed mechanism is straightforward: increased heart rate plus altered blood pressure plus potential effects on blood vessel function could, in someone with pre-existing cardiovascular vulnerability, tip the balance toward an acute event.
But the largest analysis of the available data tells a more nuanced story. A 2023 meta-analysis by Theerasuwipakorn and colleagues pooled data from 20 studies involving approximately 183 million patients, making it the largest analysis of cannabis and cardiovascular outcomes ever conducted.[1] The headline finding: cannabis use was not significantly associated with either heart attack or stroke in the overall analysis. The odds ratio for heart attack was 1.29, and for stroke 1.35, but neither reached statistical significance.
This does not prove cannabis is safe for the heart. It means that across the largest available dataset, the signal for cardiovascular harm is not strong or consistent enough to reach the threshold for statistical confidence. The difference between "not proven harmful" and "proven safe" matters. For a detailed breakdown of this research, including who faces the highest risk, see cannabis and cardiovascular health. For the broader picture of how cannabis interacts with heart health markers, see weed and heart health.
The practical takeaway: if you are young, healthy, and have no cardiovascular risk factors, the acute effects of cannabis on your heart are unlikely to cause problems. If you are over 40, have high blood pressure, coronary artery disease, or a history of cardiac events, the equation changes. These are not scare tactics. They are the same considerations that apply to any activity that acutely stresses the cardiovascular system.
Respiratory and Lung Health
Smoked cannabis and smoked tobacco deliver many of the same combustion byproducts: carbon monoxide, tar, particulate matter, and volatile organic compounds. This is a fact of chemistry, not of cannabis specifically. Anything you combust and inhale introduces these substances into your airways.
What makes cannabis and tobacco diverge is what the large-scale epidemiological data shows. A landmark 2012 study by Pletcher and colleagues, published in JAMA, followed over 5,000 adults for more than 20 years and found that moderate cannabis smoking (one joint per day for up to seven years) was not associated with adverse effects on lung function as measured by FEV1 (the amount of air you can forcefully exhale in one second) or FVC (total lung capacity). In fact, occasional cannabis users showed slightly better lung function than non-users, a finding the researchers attributed to the deep-inhalation technique used with cannabis acting as a form of lung exercise, not to any protective property of cannabis smoke.
Heavy, long-term cannabis smoking tells a different story. The same study noted that at higher levels of cumulative exposure, lung function began to decline. Regular cannabis smokers commonly develop chronic bronchitis symptoms: coughing, increased phlegm production, wheezing, and shortness of breath. A review by Tashkin confirmed that habitual cannabis smoking is associated with increased symptoms of chronic bronchitis[2] but found that the evidence for a link to COPD (chronic obstructive pulmonary disease) or lung cancer was inconsistent.
The lung cancer question is particularly interesting. Despite cannabis smoke containing many of the same carcinogens as tobacco smoke, large epidemiological studies have not established a clear, dose-dependent link between cannabis smoking and lung cancer. A 2015 meta-analysis by Huang and colleagues in the International Journal of Cancer found no significant association between long-term cannabis use and lung cancer risk after controlling for tobacco use. The reasons for this discrepancy are debated. Some researchers have proposed that THC and CBD may have anti-tumor properties that partially offset the carcinogenic effects of smoke, though this hypothesis remains speculative and should not be used to justify smoking as harmless.
The clearest harm reduction message from the respiratory research is about the delivery method, not the substance. Switching from smoked cannabis to edibles, tinctures, or dry herb vaporizers eliminates combustion byproducts entirely. If you are dealing with acne or skin issues related to weed use, delivery method may also play a role, since smoke exposure and hormonal shifts both affect skin health. For more on how your lungs recover after you stop smoking, see lung recovery after quitting weed. If you are experiencing the increased coughing that often follows quitting, that is typically a sign of healing. Your cilia (the tiny hair-like structures that sweep debris out of your airways) are coming back online. We cover what to expect in coughing up stuff after quitting weed.
Appetite, Metabolism, and Weight
The munchies are real, measurable, and well understood. THC activates CB1 receptors in the hypothalamus, the brain region that regulates hunger, producing a genuine increase in appetite hormones and a reduction in satiety signals. THC also enhances the smell and taste of food through increased activity in the olfactory bulb. This is not subjective. It is a documented biological cascade that makes food more appealing at a neurochemical level.
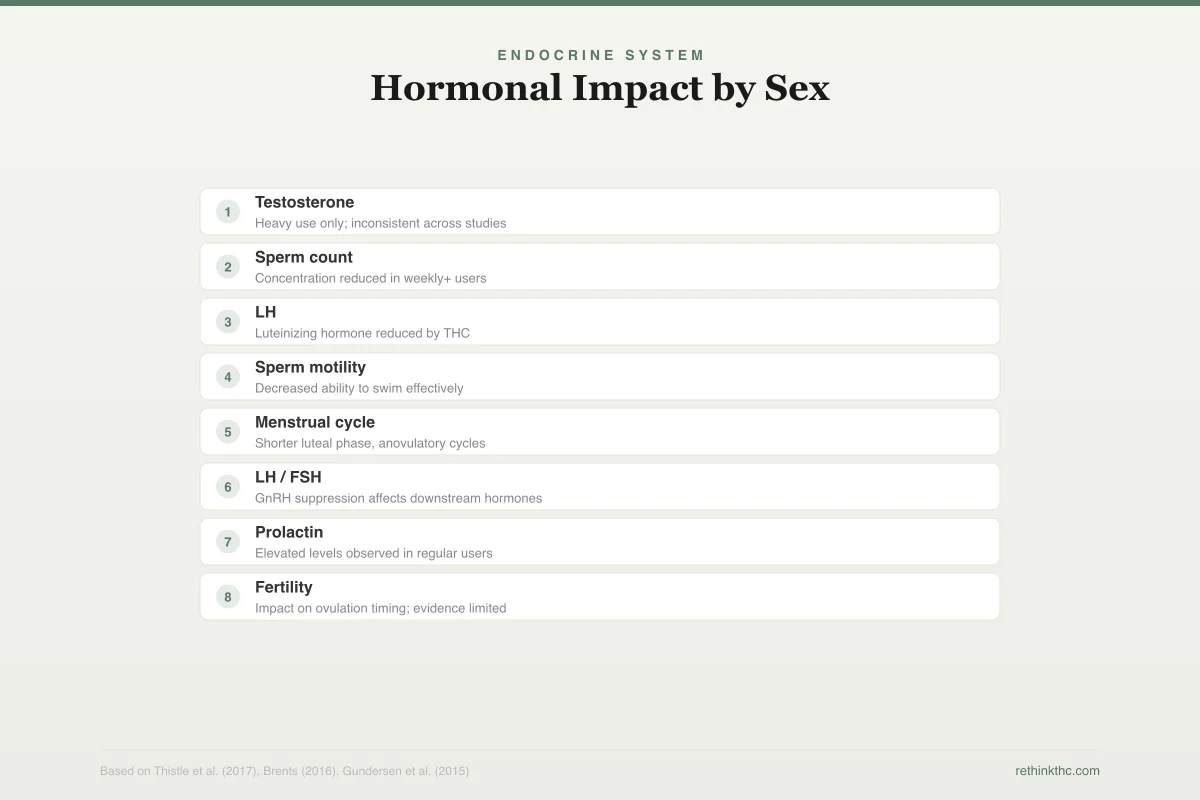
Endocrine System
Hormonal Impact by Sex
Male
Testosterone
-15-20%Heavy use only; inconsistent across studies
Sperm count
-28%Concentration reduced in weekly+ users
LH
SuppressedLuteinizing hormone reduced by THC
Sperm motility
ReducedDecreased ability to swim effectively
Female
Menstrual cycle
DisruptedShorter luteal phase, anovulatory cycles
LH / FSH
AlteredGnRH suppression affects downstream hormones
Prolactin
IncreasedElevated levels observed in regular users
Fertility
UnclearImpact on ovulation timing; evidence limited
Reversibility
Most hormonal and reproductive effects appear reversible after cessation. Male testosterone and sperm parameters generally normalize within 3-6 months of stopping. Female cycle regularity typically returns within a few months, though individual timelines vary.
What makes the weight and metabolism picture complicated is the paradox that large population studies consistently reveal: despite the appetite-stimulating effects of THC, cannabis users as a group tend to have lower BMI and lower rates of obesity than non-users. A 2011 study by Le Strat and Bhatt, published in the American Journal of Epidemiology, analyzed two large national surveys totaling over 50,000 participants and found that the obesity rate among cannabis users was roughly one-third lower than among non-users, even after adjusting for confounders.
Several hypotheses have been proposed to explain this paradox. One is that chronic THC exposure downregulates CB1 receptors over time, effectively recalibrating the appetite system to a lower set point. Another is behavioral: regular cannabis users may substitute cannabis for alcohol or high-calorie comfort behaviors. A third possibility is that the relationship is confounded by factors like age, since cannabis users skew younger and younger people tend to have lower BMI regardless of cannabis use.
When you quit cannabis, the appetite system goes through a measurable recalibration. Most people experience a significant drop in appetite during the first week, followed by gradual recovery as CB1 receptors normalize over roughly 14 to 28 days. Some people experience weight gain after quitting, typically not because metabolism slows but because they replace the oral habit of smoking with eating or use food to manage emotions that cannabis previously suppressed. For the full breakdown of what happens to your appetite and weight when you stop, see quitting weed and appetite changes.
Hormonal Effects: Testosterone, Estrogen, and Cortisol
Cannabis interacts with your endocrine system through CB1 and CB2 receptors in the hypothalamus, pituitary gland, and gonads. These interactions affect the production and regulation of several major hormones, though the magnitude and clinical significance of these effects remain subjects of active research.
Testosterone and Male Reproductive Health
The question of whether cannabis lowers testosterone has been studied for over 50 years, and the answer is genuinely mixed. Some studies have found that chronic cannabis use is associated with modestly lower testosterone levels, while others have found no significant difference between users and non-users. A 2017 meta-analysis by Thistle and colleagues, published in the Journal of Urology, found that the evidence for a clinically meaningful effect of cannabis on testosterone was inconsistent across studies.
What the research does show more consistently is that cannabis affects sperm. Multiple studies have documented associations between regular cannabis use and reduced sperm count, decreased sperm motility (the ability of sperm to swim effectively), and altered sperm morphology (shape). A 2015 study by Gundersen and colleagues, published in the American Journal of Epidemiology, found that men who used cannabis more than once per week had a 28% lower sperm concentration than those who did not use it. The clinical significance of this finding depends on whether the reduction is enough to affect fertility in a given individual, which varies. For a full review of this research, see weed and testosterone and weed and fertility.
The encouraging finding: most hormonal and reproductive effects appear to be reversible after cessation. Testosterone levels and sperm parameters generally normalize within weeks to months of stopping cannabis use, though the timeline varies by individual and duration of prior use.
Female Hormones and Reproductive Health
Cannabis affects the female reproductive system through similar endocannabinoid pathways. CB1 receptors are present in the ovaries, uterus, and hypothalamic-pituitary-ovarian axis. Research has linked regular cannabis use to disrupted menstrual cycles, altered luteinizing hormone (LH) levels, and potential effects on ovulation timing.
A 2021 review in the Journal of the Endocrine Society noted that THC can suppress the release of gonadotropin-releasing hormone (GnRH) from the hypothalamus, which in turn affects the downstream hormones that regulate the menstrual cycle. Women who use cannabis regularly may experience shorter luteal phases, anovulatory cycles (cycles without ovulation), or changes in menstrual flow, though these findings come from relatively small studies and individual variation is substantial.
Safety
CriticalCannabis during pregnancy
Concern
The American College of Obstetricians and Gynecologists recommends against all cannabis use during pregnancy and breastfeeding. THC crosses the placenta and has been linked to lower birth weight and potential neurodevelopmental effects in children.
What the research says
This is one area where the medical consensus is clear and not ambiguous. The potential risks to fetal development outweigh any benefit.
Particularly relevant for: Pregnant or breastfeeding women, women planning pregnancy
What to do
If you are pregnant, trying to conceive, or breastfeeding, stop cannabis use. Discuss alternative approaches for any symptoms you were managing with cannabis with your OB-GYN.
ACOG Committee Opinion No. 722; reviewed evidence on prenatal THC exposure
During pregnancy, the stakes are different. The American College of Obstetricians and Gynecologists (ACOG) recommends against cannabis use during pregnancy and breastfeeding, citing evidence linking prenatal THC exposure to lower birth weight and potential neurodevelopmental effects in children. If you are on hormonal contraception, the interaction between THC and synthetic hormones adds another variable — see THC and birth control for what the research shows. For women navigating the hormonal recovery after stopping cannabis, see quitting weed and female hormones.
Cortisol and the Stress Response
THC interacts with the hypothalamic-pituitary-adrenal (HPA) axis, the system that controls your stress response and cortisol production. Acute cannabis use can transiently increase cortisol levels, while chronic use appears to blunt the HPA axis response over time, leading to a dysregulated stress response in heavy users. A 2017 study by Cuttler and colleagues, published in Psychoneuroendocrinology, found that chronic cannabis users showed a blunted cortisol response to acute stress compared to non-users, suggesting that long-term use may impair the body's ability to mount a normal stress response.
This matters because cortisol is not just a stress hormone. It regulates inflammation, blood sugar, sleep-wake cycles, and immune function. For neurological conditions like Parkinson's disease, where tremor and sleep disruption intersect with the endocannabinoid system, the hormonal and neurological effects of cannabis overlap in ways that require careful consideration. A dysregulated HPA axis affects your entire physiology, not just how you handle stressful situations. For a closer look at the cortisol connection, see weed, cortisol, and stress hormones.
Immune System Effects
The relationship between cannabis and immunity is one of the least resolved areas of cannabis research, partly because the endocannabinoid system plays a complex, bidirectional role in immune regulation. CB2 receptors are densely expressed on immune cells, including T cells, B cells, macrophages, and natural killer cells. When THC and CBD bind to these receptors, they modulate immune function in ways that can be either immunosuppressive or anti-inflammatory, depending on the context.
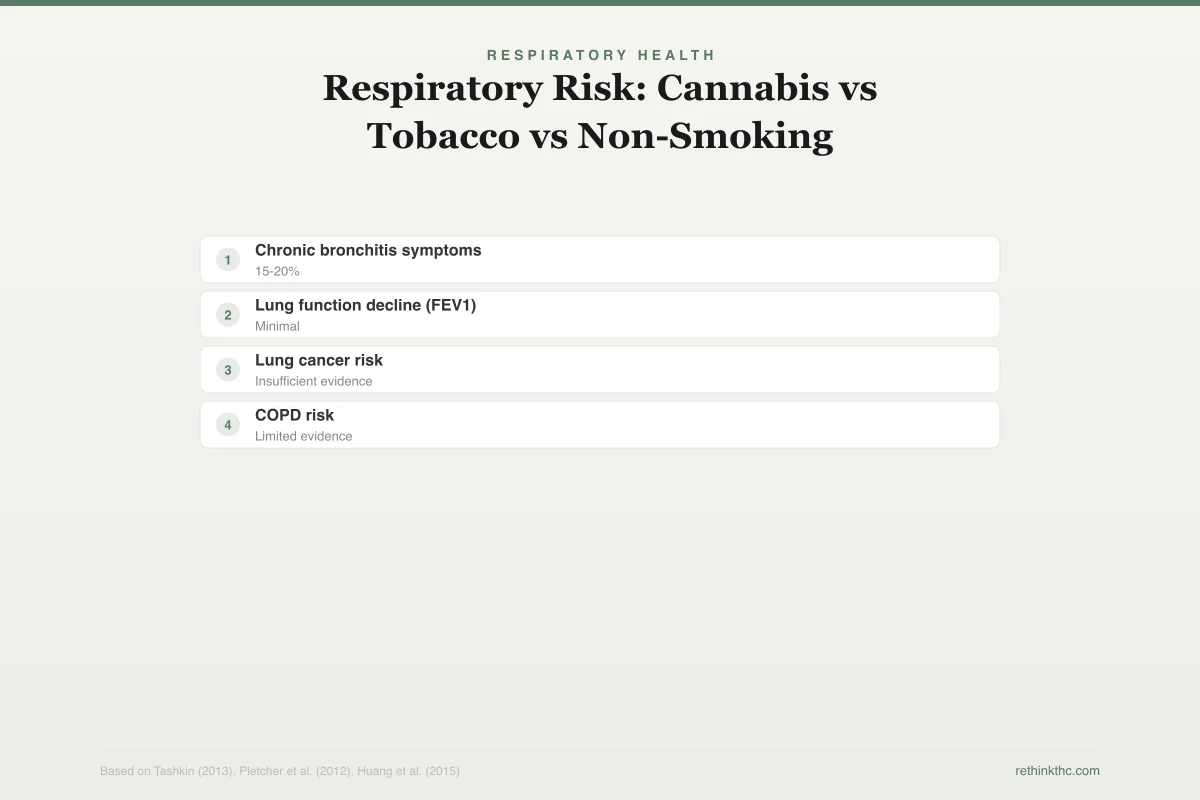
Respiratory Health
Respiratory Risk: Cannabis vs Tobacco vs Non-Smoking
Chronic bronchitis symptoms
Lung function decline (FEV1)
Lung cancer risk
COPD risk
Key finding: Despite sharing many combustion byproducts, cannabis smoking has not shown the same dose-dependent links to lung cancer or COPD as tobacco. Switching to non-combustion methods (edibles, vaporizers) eliminates respiratory risk entirely.
A 2020 review by Nichols and Kaplan, published in the Journal of Neuroimmune Pharmacology, summarized the evidence as showing that cannabinoids generally have immunosuppressive and anti-inflammatory properties. In conditions where inflammation is the problem, such as autoimmune diseases or chronic inflammatory conditions like arthritis, Crohn's disease, or IBS, this could theoretically be beneficial. In contexts where you need a robust immune response, such as fighting an infection or recovering from surgery, immunosuppression could be harmful.
The clinical evidence for cannabis meaningfully impairing immune function in otherwise healthy people is limited. Large epidemiological studies have not found that cannabis users are significantly more susceptible to infections compared to non-users. However, the research base is thin enough that definitive conclusions are premature.
One area where the immune implications are clearer is in HIV/AIDS patients. Cannabis has been studied as an appetite stimulant and anti-nausea agent in this population, and some research suggests that cannabinoids do not worsen HIV viral load or immune status as measured by CD4 counts. However, this is a specific clinical context with specific populations and should not be generalized to broad claims about cannabis and immunity.
Sex Differences in Cannabis Response
Men and women do not experience cannabis the same way, and the differences go beyond hormonal effects. Research has documented sex-based differences in how quickly tolerance develops, how severe withdrawal symptoms are, and how cannabinoids are metabolized.
Women tend to develop tolerance to THC's effects faster than men. A 2014 study by Cooper and Haney, published in Drug and Alcohol Dependence, found that women required fewer exposures to develop tolerance to many of THC's subjective and cardiovascular effects. Women also report different withdrawal symptom profiles. Research consistently shows that women experience more severe withdrawal symptoms than men, particularly in the domains of irritability, sleep disruption, and gastrointestinal distress.
Part of this difference is hormonal. Estrogen and progesterone interact with the endocannabinoid system, and fluctuations across the menstrual cycle can influence both the effects of cannabis and the severity of withdrawal. This means that the timing of quitting within a menstrual cycle may affect how the first few weeks feel, though the research on this specific question is still early.
Body composition also plays a role. THC is lipophilic, meaning it dissolves in fat and is stored in adipose tissue. Because women generally have a higher body fat percentage than men, THC can accumulate to a greater degree and take longer to fully clear the body. This has implications for drug testing timelines, withdrawal duration, and the subjective experience of cessation. For more on sex-specific differences, see the detailed guides on withdrawal in women and withdrawal in men.
Practical Harm Reduction for Physical Health
If you use cannabis and want to minimize the physical health risks, the research points to several evidence-based strategies. These are not moral prescriptions. They are practical risk-reduction measures drawn from the published literature, including the Lower-Risk Cannabis Use Guidelines (LRCUG) developed by Fischer and colleagues and endorsed by public health organizations in multiple countries.
Choose your delivery method carefully. Smoking is the highest-risk method for respiratory health. Edibles eliminate respiratory risk entirely but carry a higher risk of overconsumption due to delayed onset. Dry herb vaporizers reduce (though may not eliminate) combustion byproducts. For a full comparison of methods by harm profile, see healthiest way to consume cannabis.
Use lower-potency products. Higher THC concentrations produce more pronounced acute effects on heart rate, blood pressure, and hormone disruption. The LRCUG specifically recommends choosing products with lower THC content and avoiding synthetic cannabinoids entirely. For the full set of evidence-based recommendations, see safer cannabis use guidelines.
Monitor your frequency. Many of the physical health effects discussed in this article, from hormonal disruption to respiratory irritation to cardiovascular stress, are dose-dependent and cumulative. Daily use carries a different risk profile than occasional use. This is not unique to cannabis. It is true of alcohol, caffeine, and most substances that interact with your physiology. If you use cannabis around physical activity, the body-level effects matter in specific ways — whether that is exercise and THC, running, weightlifting, or even golf.
Know your individual risk factors. If you have cardiovascular disease, respiratory conditions, hormonal imbalances, or are trying to conceive, the risk-benefit calculation is different for you than for someone without those factors. The same applies if you are using cannabis to manage a specific condition like fibromyalgia, migraines, endometriosis pain, menstrual cramps, or carpal tunnel and nerve pain — the physical effects discussed in this article layer on top of whatever condition-specific risks exist. This is where honest conversations with healthcare providers matter. An increasing number of physicians are willing to have nonjudgmental discussions about cannabis use if you bring it up.
Understand how cannabis affects motor function and reaction time. The same cardiovascular and neurological effects that cannabis produces in your body also affect your ability to drive safely. For the science on impairment, including how it compares to alcohol, see weed DUI and driving impairment laws.
Pay attention to what your body tells you. Persistent coughing, chest tightness, heart palpitations, menstrual irregularities, digestive changes, or sexual dysfunction that correlates with cannabis use are worth taking seriously. These symptoms are data, and ignoring them because you do not want to hear the answer is not a harm reduction strategy.
What We Know and What We Do Not
The physical health research on cannabis is better than it was a decade ago and worse than it needs to be. Federal scheduling restrictions have limited the quantity and quality of clinical trials. Most of what we know comes from observational studies, which can identify associations but cannot prove causation. The cannabis products studied in most research bear little resemblance to the high-potency concentrates and edibles that dominate today's market.
What the evidence does support: cannabis acutely stresses the cardiovascular system, smoked cannabis irritates the airways, THC alters hormonal signaling and can affect fertility, and the immune effects are real but complex. What it does not support: the claim that cannabis is categorically dangerous to your physical health, or the opposite claim that it is categorically safe.
The most honest position is that cannabis, like many substances that interact with your biology, carries real physical effects that vary enormously depending on the person, the product, the dose, the frequency, and the delivery method. Understanding those variables puts you in a better position to make decisions that account for your own body, your own health profile, and your own priorities.
When to Seek Professional Help
If you experience chest pain, heart palpitations, difficulty breathing, sudden numbness or weakness, severe digestive symptoms, or any other acute physical symptoms during or after cannabis use, seek medical attention. These symptoms deserve evaluation regardless of their cause.
If you are finding it difficult to reduce or stop cannabis use despite wanting to, that is also worth addressing. Understanding the signs of cannabis use disorder is a good starting point, and the physical health considerations discussed in this article are often part of what motivates change.
SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day, 7 days a week. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
The Bottom Line
Comprehensive pillar covering cannabis physical health effects system by system. Cardiovascular: THC activates sympathetic nervous system → HR increase 20-50+ bpm, orthostatic hypotension; Volkow 2014 NEJM noted elevated heart attack risk in first hour post-use. BUT Theerasuwipakorn 2023 meta-analysis (20 studies, 183M patients) found cannabis NOT significantly associated with MI or stroke overall (OR 1.29/1.35, neither reached significance). Respiratory: Pletcher 2012 JAMA (5,000+ adults, 20 years) — moderate smoking not associated with adverse FEV1/FVC; heavy use → decline + chronic bronchitis symptoms. Tashkin review: bronchitis association confirmed but inconsistent COPD/lung cancer evidence despite shared carcinogens with tobacco. Appetite/weight: THC activates hypothalamic CB1 → appetite increase; paradoxically, population studies show lower BMI in users (Le Strat 2011, 50K+ participants). Hormones: mixed testosterone evidence; more consistent sperm effects (Gundersen 2015: 28% lower concentration with weekly+ use); female cycle disruption via GnRH suppression; cortisol/HPA axis blunting (Cuttler 2017). Most hormonal effects reversible. Immune: CB2 on immune cells → generally immunosuppressive/anti-inflammatory; no clear clinical impairment in healthy users. Sex differences: women develop tolerance faster, worse withdrawal, longer THC storage. Harm reduction: delivery method, lower potency, frequency monitoring, individual risk factors.
Sources & References
- 1RTHC-04980·Theerasuwipakorn, Nonthikorn (2023). “Cannabis and Heart Attack/Stroke Risk: A 183-Million-Patient Meta-Analysis Finds Stroke Risk but Not Heart Attack Risk.” Toxicology Reports.Study breakdown →PubMed →↩
- 2RTHC-00207·Tashkin, D P (2005). “Marijuana Smoking Causes Airway Inflammation and Cell Changes But Evidence for COPD and Lung Cancer Remains Limited.” Monaldi archives for chest disease = Archivio Monaldi per le malattie del torace.Study breakdown →PubMed →↩
What the Research Shows
This section synthesizes 213 peer-reviewed studies on Cannabis and Cardiovascular Health. Stronger evidence means more consistency across study types.
Largest-ever meta-analysis (183M patients) found cannabis use significantly associated with stroke risk but not heart attack risk — though observational data can't prove causation
Strong EvidenceMeta-analysis of 81 million participants found cannabis use associated with 71% higher atrial arrhythmia risk, with concurrent drug use and legal country status further increasing risk
Strong EvidenceMeta-analysis of 100+ million participants plus genetic analysis confirms cannabis use disorder is causally linked to stroke, particularly large artery stroke
Strong EvidenceWhere Scientists Disagree
Areas where research shows conflicting results or ongoing scientific debate.
A 1978 medical review identified cannabis as promising for glaucoma and asthma but flagged cardiovascular risks during exercise and preliminary concerns about lung and immune effects
Moderate EvidenceA major 1986 pharmacological review found cannabis's greatest health concern was its impact on youth development, while finding no proven brain damage and limited physical dependence in adults
Moderate EvidenceReview finding cannabis increases heart rate with rapid tolerance development, poses minimal risk for young healthy users but significant risks for people with existing cardiovascular disease
Moderate EvidenceReview comparing cardiovascular effects of five substance classes, finding cannabis posed fewer heart risks than opiates, amphetamines, or alcohol, though cognitive effects were noted
Moderate EvidenceWhat We Still Don't Know
- Only 7 randomized controlled trials exist out of 213 studies — most evidence is observational or from reviews.
- Long-term prospective studies tracking outcomes over 5+ years are largely absent from the literature.
- Research on diverse populations (different ages, ethnicities, and medical backgrounds) remains limited.
Evidence Breakdown
Distribution of study types in this research area. Higher-tier evidence (meta-analyses, RCTs) provides stronger conclusions.
Research Timeline
How our understanding of this topic has evolved.
Pre-2000
6 studies published. Includes 2 RCTs.
2000–2009
9 studies published. Predominantly observational and review studies.
2010–2014
13 studies published. Predominantly observational and review studies.
2015–2019
43 studies published. Includes 1 RCTs, 1 strong-evidence studies.
2020–present
142 studies published. Includes 7 meta-analyses, 4 RCTs, 20 strong-evidence studies.