Vaping vs Smoking vs Edibles: A Harm Reduction Guide
Harm Reduction & Moderation
No Combustion
Canada's Lower-Risk Cannabis Use Guidelines rank avoiding combustion as the top harm reduction strategy, since cannabis smoke contains over 100 of the same toxic byproducts found in tobacco smoke.
Fischer et al. (2019)
Fischer et al. (2019)
View as imageIf you only read one thing
If your main concern is your lungs, edibles and tinctures are the safest because nothing gets inhaled. If you want to inhale, a dry herb vaporizer is the best-studied alternative to smoking — it heats weed below the burning point and cuts out most of the toxic stuff. Smoking is the worst option for your lungs no matter how you do it, and bongs don't actually filter out the bad stuff. Vape cartridges are somewhere in between — regulated ones avoided the EVALI crisis, but we don't have long-term safety data yet.
You are not looking for someone to tell you cannabis is safe or dangerous. You are looking for the healthiest way to consume cannabis, because you already use it and you want to make smarter choices about how. That is a completely reasonable question, and the science actually has useful answers. Different consumption methods carry very different risk profiles depending on which organ system you are concerned about. Smoking, vaping oil cartridges, dry herb vaporizers, edibles, and tinctures each come with their own trade-offs. This guide breaks down what the research says about each one so you can make informed decisions based on your own priorities.
Key Takeaways
- Smoking joints, bowls, or bongs produces over 100 toxic byproducts including tar, carbon monoxide, and fine particulate matter — making combustion the most harmful delivery method for your lungs
- The 2019 EVALI outbreak hospitalized over 2,800 people and killed 68, and it was primarily linked to vitamin E acetate in unregulated THC cartridges — not regulated dispensary products
- Edibles carry zero respiratory risk but create dosing challenges because your liver converts THC into 11-hydroxy-THC — a stronger metabolite with a delayed onset of 30 minutes to 2 hours
- Canada's Lower-Risk Cannabis Use Guidelines (LRCUG) explicitly recommend avoiding combustion as a primary harm reduction strategy
- Dry herb vaporizers heat cannabis below the combustion point — around 180 to 210 degrees Celsius — which significantly cuts toxic byproduct exposure compared to smoking
- Tashkin's review confirmed cannabis smoke contains over 100 of the same toxic byproducts found in tobacco smoke, so how you consume is one of the highest-impact harm reduction choices you can make
Why How You Consume Matters as Much as How Much
The active compound is the same regardless of delivery method. THC is THC. But the vehicle that carries it into your body determines which organs take the hit and what additional chemicals come along for the ride.
Methods Compared
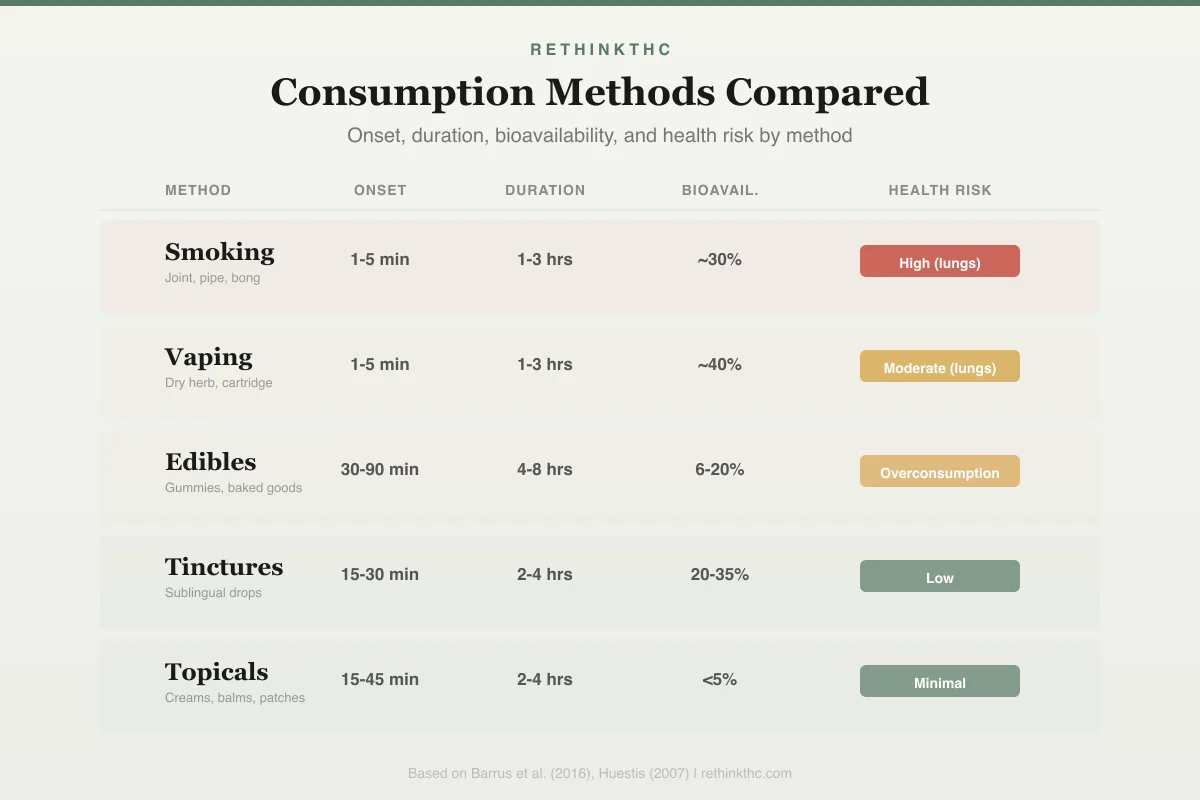
Cannabis Consumption Methods
Onset, duration, bioavailability, and health risk
Smoking
Joint, pipe, bong
Onset
1-5 min
Duration
1-3 hrs
Bioavail.
~30%
Vaping
Dry herb, cartridge
Onset
1-5 min
Duration
1-3 hrs
Bioavail.
~40%
Edibles
Gummies, baked goods
Onset
30-90 min
Duration
4-8 hrs
Bioavail.
6-20%
Tinctures
Sublingual drops
Onset
15-30 min
Duration
2-4 hrs
Bioavail.
20-35%
Topicals
Creams, balms, patches
Onset
15-45 min
Duration
2-4 hrs
Bioavail.
<5%
Canada's Lower-Risk Cannabis Use Guidelines (LRCUG), published by Fischer and colleagues in the American Journal of Public Health (a leading peer-reviewed public health journal), are among the most evidence-based harm reduction recommendations available for cannabis. Their number one delivery-method recommendation is straightforward: avoid combustion. Smoking anything, whether cannabis, tobacco, or any plant material, produces toxic byproducts that damage lung tissue. The risk is not unique to cannabis. It is inherent to fire.
This does not mean every alternative is perfectly safe. Each method shifts the risk to different systems. The goal of harm reduction is not eliminating all risk. It is understanding where the risks are so you can choose the trade-offs that make sense for your life.
Smoking: The Highest Respiratory Risk
Smoking remains the most common way people use cannabis worldwide, and it carries the highest burden of harm to your lungs. A review by Tashkin found that cannabis smoke contains over 100 of the same toxic combustion byproducts found in tobacco smoke.[1] That includes tar, carbon monoxide, hydrogen cyanide, ammonia, and fine particulate matter.
These byproducts cause chronic bronchial irritation, damage the cilia (tiny hair-like structures that sweep debris out of your airways), and trigger airway remodeling where mucus-producing cells multiply and bronchial walls thicken. The result is chronic bronchitis symptoms: persistent cough, wheezing, excess mucus, and shortness of breath. Regular cannabis smokers report these symptoms at two to three times the rate of non-smokers.
The good news, as covered in the lung recovery timeline after quitting, is that most smoking-related respiratory damage from cannabis is reversible. Unlike tobacco, cannabis smoking has not been consistently linked to emphysema or COPD in large longitudinal studies. But "reversible once you stop" is not the same as "harmless while you are doing it."
Joints vs. bongs vs. bowls. There is a common belief that bongs filter out toxins through water. Research does not support this. A NORML and MAPS study found that water pipes filter out some water-soluble THC while letting most particulate matter through, potentially resulting in a worse ratio of toxins to THC than an unfiltered joint. If you are wondering about the practical differences between rolling options, the blunts vs joints vs spliffs guide covers what sets them apart. For a broader side-by-side of inhalation devices, see the bongs vs vapes vs pipes comparison. But the delivery method within smoking matters far less than the fact of combustion itself.
Vaping Oil Cartridges: The EVALI Question
Oil-based THC vape cartridges became enormously popular in the late 2010s for the same reasons they accelerate dependence: they are discreet, convenient, potent, and produce almost no odor. If you are noticing that convenience has made your use harder to control, the vape pen addiction guide explains exactly why. And if you are using high-potency concentrates or dabs, the withdrawal experience can be significantly more intense than what flower users face.
The biggest safety event in vaping history was the EVALI crisis (e-cigarette or vaping product use-associated lung injury). In 2019, the CDC investigated an outbreak that ultimately hospitalized over 2,800 people and killed 68 across the United States. The primary cause was identified as vitamin E acetate, an oily thickening agent added to black-market THC cartridges to make diluted oil look full-strength. When heated and inhaled, vitamin E acetate coats lung tissue and triggers severe inflammatory damage.
Safety
CriticalUnregulated vape cartridges caused the EVALI crisis
Concern
The 2019 EVALI outbreak hospitalized over 2,800 people and killed 68 across the United States. The primary cause was vitamin E acetate, a thickening agent added to black-market THC cartridges to make diluted oil look full-strength.
What the research says
Regulated, lab-tested cartridges from licensed dispensaries were not implicated in the outbreak. The danger came from the unregulated supply chain, not from vaporizing cannabis oil itself.
Particularly relevant for: Anyone using THC vape cartridges purchased outside regulated dispensaries
What to do
Only purchase cartridges from licensed dispensaries with lab testing. If you cannot verify the source, the cartridge is not worth the risk.
CDC EVALI investigation (2019-2020)
The critical detail: EVALI was overwhelmingly linked to unregulated, illicit-market cartridges. Regulated, lab-tested products from licensed dispensaries were not implicated in the outbreak. This does not mean regulated cartridges are risk-free. It means the single largest documented vaping danger came from a supply chain problem, not from vaporizing cannabis oil itself. Understanding the difference between legal dispensary products and street weed is one of the most practical harm reduction steps you can take.
What we do not know yet. Vaping THC oil as a widespread practice is less than 15 years old. Long-term longitudinal studies on chronic cannabis vape use do not exist yet. The long-term pulmonary effects of inhaling vaporized cannabis oil, propylene glycol, and other carrier liquids remain genuinely unknown. Absence of evidence is not evidence of absence.
Contamination risk. Beyond EVALI, unregulated cartridges have been found to contain pesticide residues, heavy metals leached from cheap heating elements, and residual solvents from extraction. If you are buying cartridges outside the regulated market, the contaminated vape guide covers what to watch for and what the real risks are.
Dry Herb Vaporizers: The Middle Ground
Dry herb vaporizers heat cannabis flower to temperatures between 180 and 210 degrees Celsius, hot enough to vaporize cannabinoids and terpenes but below the combustion point (around 230 degrees Celsius). This is a fundamentally different process than burning.
Respiratory Harm
Respiratory Risk by Consumption Method
Descending risk from combustion to zero-inhalation methods
Combustion (Joint/Pipe)
HIGHVape Cartridge (Oil)
MODERATEDry Herb Vaporizer
LOW–MODEdibles / Tinctures
NONE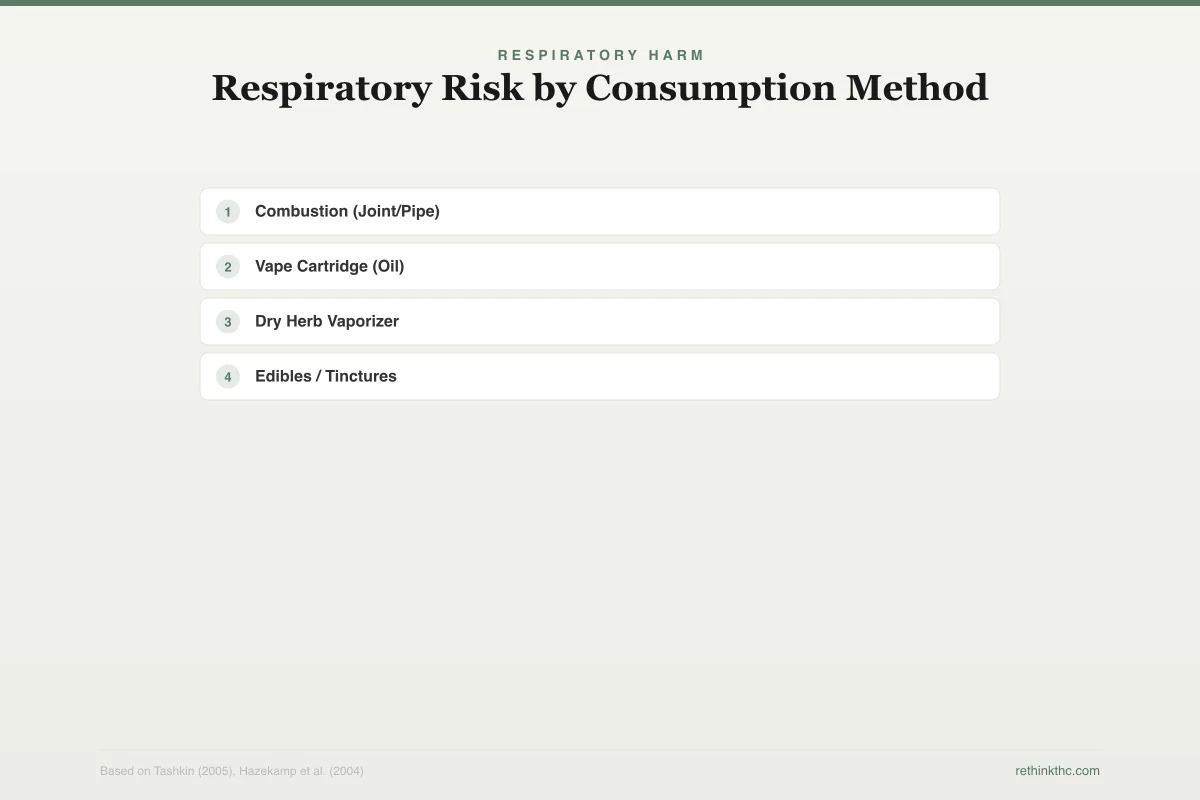
A 2004 study by Hazekamp and colleagues, published in the Journal of Pharmaceutical Sciences (a peer-reviewed pharmacology journal), found that vapor produced by a dry herb vaporizer contained significantly fewer toxic byproducts than smoke. Levels of carbon monoxide, tar, and several known carcinogens were dramatically reduced or absent in vapor compared to combusted cannabis.
A 2007 study by Abrams and colleagues, published in Clinical Pharmacology and Therapeutics, confirmed that vaporizing cannabis delivered comparable levels of THC to smoking while producing substantially lower carbon monoxide levels in exhaled breath. Participants reported fewer respiratory symptoms when using a vaporizer compared to smoking.
Dry herb vaporizers vs. oil cartridges. These are different products with different risk profiles. Dry herb vaporizers use whole flower, which means no carrier liquids, no cutting agents, and no vitamin E acetate risk. The supply chain is simpler: if you can verify the flower, you know what you are vaporizing. Oil cartridges involve extraction, dilution, and additives that introduce additional variables. For a detailed breakdown of device types, the dry herb vape vs oil vape vs disposable guide compares the hardware side by side.
For lung health specifically, dry herb vaporizers represent one of the most evidence-supported alternatives to smoking. They are the method most directly recommended by harm reduction researchers as a substitute for combustion.
Edibles: Zero Lung Risk, Different Challenges
Edibles eliminate respiratory risk entirely. Nothing is inhaled. For anyone whose primary concern is lung health, edibles are the safest option available. But they introduce a completely different set of challenges.
When you eat cannabis, THC passes through your digestive system and into your liver, where it is converted into 11-hydroxy-THC through first-pass metabolism. This metabolite is more potent than regular THC, crosses the blood-brain barrier more efficiently, and lasts significantly longer. This is why edibles produce a heavier, more intense, longer-lasting experience than smoking the same amount of THC. The edibles withdrawal guide covers how this different metabolic pathway affects your body when you stop.
The dosing problem. Onset from edibles takes 30 minutes to 2 hours, sometimes longer depending on stomach contents and individual metabolism. This delay is responsible for the most common edible-related emergency room visits: someone takes a dose, feels nothing after 45 minutes, takes more, and then both doses hit simultaneously. A study by Monte and colleagues, published in the Annals of Internal Medicine, documented the increase in cannabis-related ER visits in Colorado after legalization[2], with edibles disproportionately represented relative to their market share.
The psychological dimension. The intensity and unpredictability of edibles also contributes to a distinct pattern when people try to quit. Because 11-hydroxy-THC is more potent and longer-lasting, the brain adapts differently than it does to smoked cannabis, and edible addiction involves withdrawal patterns that differ from other consumption methods. In rare cases, high-dose edible use has also been linked to acute psychotic episodes and emergency room visits.
Start low, go slow. Most harm reduction guidelines recommend starting at 2.5 to 5 milligrams of THC for edibles and waiting at least two hours before considering a second dose. This is not cautious advice for beginners. It is practical guidance based on how unpredictable edible absorption can be even for experienced users. If you make edibles at home, the homemade vs store-bought edibles safety guide covers the additional dosing and contamination risks of DIY preparation. And once you have edibles on hand, how to store edibles for shelf life and potency explains how to keep them effective and safe. It is also worth knowing that THC drinks and edibles are processed differently by your body, with beverages offering a somewhat faster and more predictable onset than solid edibles.
Liver considerations. Because edibles are processed entirely through the liver, chronic heavy edible use puts more metabolic load on the liver than inhalation methods. For most healthy adults, this is not a significant concern. For people with liver conditions or those taking medications metabolized by the same enzyme pathways (particularly CYP3A4 and CYP2C9), it is worth discussing with a doctor.
Tinctures and Sublingual Products
Tinctures (cannabis dissolved in alcohol or oil, applied under the tongue) offer a partial bypass of first-pass liver metabolism. Some THC absorbs through the mucous membranes under your tongue directly into the bloodstream, while the rest is swallowed and processed through the liver like an edible. This creates a hybrid onset: faster than edibles (15 to 30 minutes for sublingual absorption) but slower than inhalation.
Tinctures carry no respiratory risk and allow more precise dosing than most edibles because they are measured in drops or milliliters rather than estimated from a food product. For people who want to avoid both combustion and the unpredictable onset of edibles, tinctures offer a reasonable middle ground. Other non-inhalation options, including THC patches, suppositories, and topicals, work through different absorption pathways and may suit people looking for localized or extended-release effects.
Ranking Methods by Organ System
Lungs. Edibles and tinctures carry zero respiratory risk. Dry herb vaporizers carry significantly reduced risk. Oil cartridges (regulated) carry uncertain long-term risk. Smoking carries the highest documented respiratory risk.
Toxicant Comparison
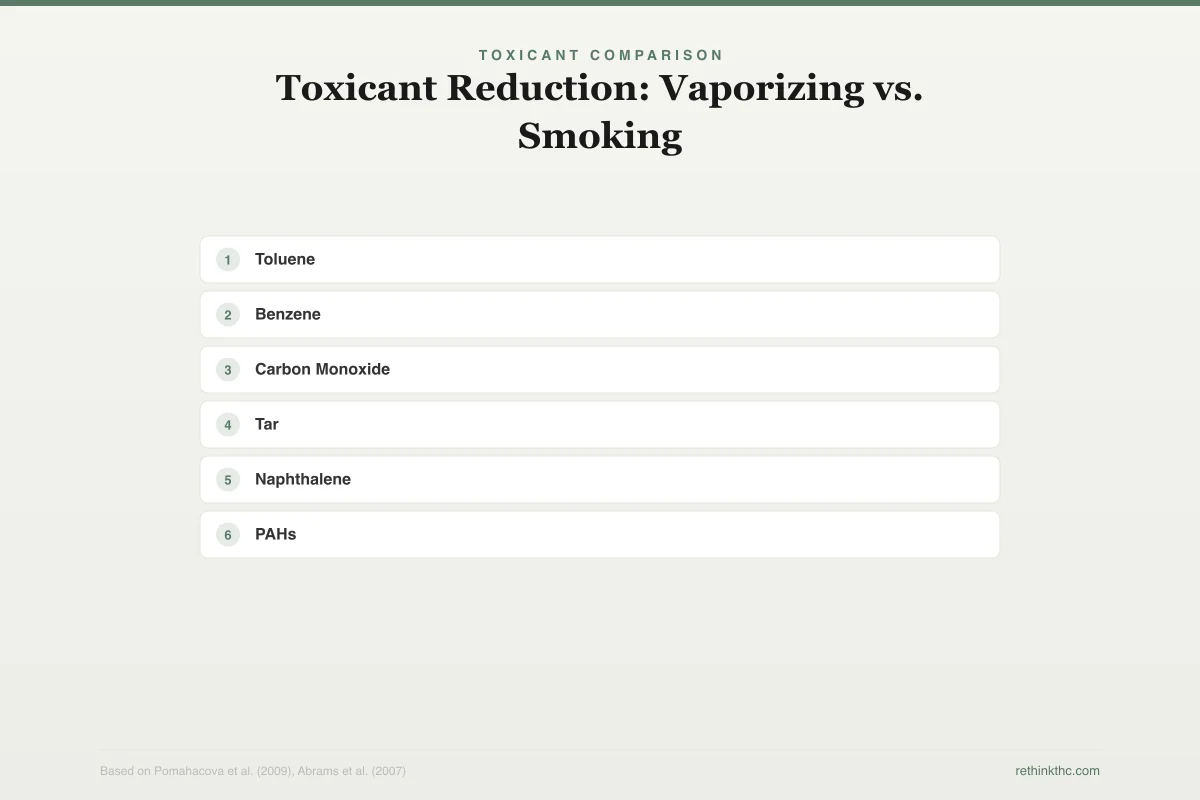
Toxicant Reduction: Vaporizing vs. Smoking
Percentage reduction when switching from combustion to dry herb vaporizer
Toluene
-97%
Benzene
-96%
Carbon Monoxide
-95%
Tar
-95%
Naphthalene
-90%
PAHs
-90%
Dry herb vaporization eliminates 90-97% of harmful combustion byproducts
Heart. THC increases heart rate regardless of delivery method, typically by 20 to 50 beats per minute for one to three hours after use. A 2001 study by Mittleman and colleagues, published in Circulation (the leading cardiology journal from the American Heart Association), found that the risk of heart attack was elevated in the hour following cannabis use. This cardiovascular effect is driven by THC itself, not by the delivery method. No consumption method eliminates cardiac risk from THC.
Liver. Edibles place the greatest metabolic load on the liver due to first-pass metabolism. Inhalation methods largely bypass the liver. For most people, this difference is clinically insignificant. For those with hepatic conditions, it matters.
Brain and dependence. Delivery methods that produce faster onset and higher peak THC levels (smoking, vaping concentrates) are associated with more rapid tolerance development. High-potency vape cartridges (70 to 90% THC) deliver the largest THC loads per use, and ultra-potent products like moon rocks push THC exposure even further. The dab and concentrate withdrawal guide covers how potency drives dependence risk. It is also worth noting that the common belief that sativa and indica strains produce meaningfully different effects is largely a myth; the THC and terpene content matters far more than the strain label. For a deeper understanding of what THC purity and potency labels actually mean and how to read them, that guide breaks down the numbers behind the marketing.
Practical Harm Reduction Steps
If you currently smoke and are not ready to quit cannabis entirely, the single most impactful change you can make is switching away from combustion. The LRCUG and most harm reduction researchers agree on this point. Here are practical options ranked by respiratory harm reduction:
- Switch to edibles or tinctures (eliminates respiratory risk entirely)
- Switch to a dry herb vaporizer (dramatically reduces respiratory toxins)
- If you continue smoking, avoid deep inhalation and prolonged breath-holding, which do not increase THC absorption but do increase particulate deposition in lung tissue
- If using oil cartridges, buy only from regulated, lab-tested sources to avoid EVALI-associated contaminants
- Store your cannabis properly to prevent degradation and mold — if you are unsure whether flower has gone bad, learn how to tell if weed is moldy and understand that cannabis does expire and loses potency over time
- If flower gets damp, the what happens if weed gets wet guide explains why moisture compromises both safety and quality
- Regardless of method, lower-potency products and less frequent use reduce harm across all organ systems
No consumption method makes cannabis risk-free. The goal is not perfection. It is making choices that reduce the most serious harms while being honest about where risks remain. If you are not sure which method fits your priorities, the what consumption method is right for you quiz or the cannabis consumption method quiz can help you narrow it down. And if you are shopping at a dispensary for the first time, the how to read a dispensary menu guide walks you through what all those labels and numbers actually mean.
When to Seek Professional Help
If you are experiencing persistent respiratory symptoms like chronic cough, wheezing, shortness of breath, or chest pain, talk to a healthcare provider regardless of what you are using or how you are using it. If your cannabis use has become difficult to control, if you have tried to cut back and could not, or if use is interfering with your work, relationships, or mental health, professional support can help.
You can reach the SAMHSA National Helpline at 1-800-662-4357. It is free, confidential, available 24/7, and provides referrals for treatment and support services. You do not need to be in crisis to call.
Making Informed Choices
There is no perfectly safe way to use any psychoactive substance. But there are meaningfully safer ways, and the differences between them are well-documented. The research is clear that combustion is the highest-harm delivery method for your lungs, that the EVALI crisis was driven by unregulated supply chains rather than vaporization itself, and that edibles trade respiratory safety for dosing unpredictability and liver metabolism. Every method has trade-offs. The fact that you are researching those trade-offs means you are already making better decisions than most. Use the information, adjust as it makes sense for your situation, and revisit your choices as the science continues to develop.
The Bottom Line
Different cannabis consumption methods carry fundamentally different risk profiles by organ system. Canada's LRCUG (Fischer et al., American Journal of Public Health) make avoiding combustion their primary delivery-method recommendation. Smoking is the highest respiratory risk: Tashkin's review found cannabis smoke contains 100+ toxic byproducts identical to tobacco smoke (tar, carbon monoxide, hydrogen cyanide), causing chronic bronchitis symptoms at 2-3x non-smoker rates — bongs do not meaningfully filter toxins (NORML/MAPS study). Oil cartridge vaping eliminates combustion byproducts but carries EVALI risk from unregulated products (2,800+ hospitalizations, 68 deaths in 2019, primarily from vitamin E acetate in black-market cartridges — regulated dispensary products were not implicated). Dry herb vaporizers (180-210°C, below 230°C combustion point) are the most evidence-supported inhalation alternative: Hazekamp et al. (2004, Journal of Pharmaceutical Sciences) found dramatically reduced toxic byproducts; Abrams et al. (2007, Clinical Pharmacology and Therapeutics) confirmed comparable THC delivery with lower carbon monoxide. Edibles eliminate all respiratory risk but introduce 11-hydroxy-THC (more potent liver metabolite) with delayed 30-120 min onset causing dosing errors — Monte et al. (Annals of Internal Medicine) documented disproportionate edible-related ER visits in Colorado. Tinctures offer a hybrid: partial sublingual bypass of liver metabolism, faster onset (15-30 min), precise dosing. By organ system: lungs (edibles/tinctures safest → dry herb vaporizer → regulated oil carts → smoking worst), heart (THC increases HR 20-50 bpm regardless of method — Mittleman et al. 2001, Circulation), liver (edibles highest load), dependence (faster onset/higher peak THC = faster tolerance, concentrates highest risk).
Sources & References
- 1RTHC-00207·Tashkin, D P (2005). “Marijuana Smoking Causes Airway Inflammation and Cell Changes But Evidence for COPD and Lung Cancer Remains Limited.” Monaldi archives for chest disease = Archivio Monaldi per le malattie del torace.Study breakdown →PubMed →↩
- 2RTHC-02190·Monte, Andrew A et al. (2019). “Edible cannabis caused more psychiatric and cardiovascular ER visits than expected based on sales volume.” Annals of internal medicine.Study breakdown →PubMed →↩