Cannabis and Your Cardiovascular System: Heart Risk, Stroke, and What the Research Shows
Balanced Cannabis Science
20-100% Heart Rate Spike
Cannabis spikes heart rate by 20 to 100 percent immediately after use, yet a 2023 meta-analysis of 183 million patients found no significant overall link to heart attack or stroke.
Theerasuwipakorn et al., Systematic Review and Meta-Analysis, 2023
Theerasuwipakorn et al., Systematic Review and Meta-Analysis, 2023
View as imageIf you only read one thing
Cannabis makes your heart beat faster every time you use it — 20 to 100% faster in the first half hour. That sounds scary, but the largest study ever done on this (183 million patients) found no clear link between cannabis and heart attack or stroke. The honest answer is: it probably matters most for people who already have heart problems. If you're young and healthy, the acute spike is likely no more dangerous than a hard workout. If you have heart disease, it's a real concern worth discussing with your doctor.
Cannabis affects your cardiovascular system every time you use it. Your heart rate increases. Your blood pressure shifts. Blood vessels respond to cannabinoids in ways researchers are still mapping. For most healthy, younger users, these acute changes come and go without noticeable consequences. But the question of whether regular cannabis use increases the long-term risk of heart attack, stroke, or other cardiovascular events is one of the most actively debated topics in cannabis research. The answer, based on the current evidence, is genuinely complicated.
Key Takeaways
- Cannabis spikes your heart rate by 20 to 100% right after use, and your risk of a heart attack may be higher in the first hour
- A 2023 meta-analysis pooling 20 studies and 183 million patients found that cannabis was NOT significantly linked to heart attack or stroke overall
- The research on cannabis and cardiovascular risk is genuinely mixed — not settled in either direction
- People with existing heart conditions, older users, and those using high-potency products face the greatest potential risk
- Cannabis potency has roughly tripled since the mid-1990s, and most heart research was done with weaker products — so the data may underestimate risk from today's cannabis
- Smoking cannabis creates combustion byproducts like carbon monoxide and particulate matter that damage blood vessels on their own, which is why switching to non-smoked methods is a meaningful step for heart health
What Happens to Your Heart When You Use Cannabis
THC activates the sympathetic nervous system (your body's "fight or flight" response), which produces a rapid and measurable increase in heart rate. Most users experience an increase of 20 to 50 beats per minute, though some studies have documented increases as high as 100%. This effect typically peaks within 15 to 30 minutes and fades over the next 1 to 3 hours.
Cardiovascular System
Acute Cardiovascular Response to Cannabis
0 min
15 min
30 min
1 hr
2 hr
3 hr
Sympathetic activation begins
BP: Slight rise
Orthostatic hypotension risk highest
BP: Dropping
Parameters return to baseline
BP: Normal
20-50%
Heart rate increase
15 min
Time to peak
1-3 hr
Duration
Develops
Tolerance (chronic use)
Elevated Risk Population
Individuals with pre-existing cardiovascular conditions, those over 40, or with coronary artery disease face heightened risk during the acute cardiovascular stress window. Heart attack risk appears elevated in the first hour after use.
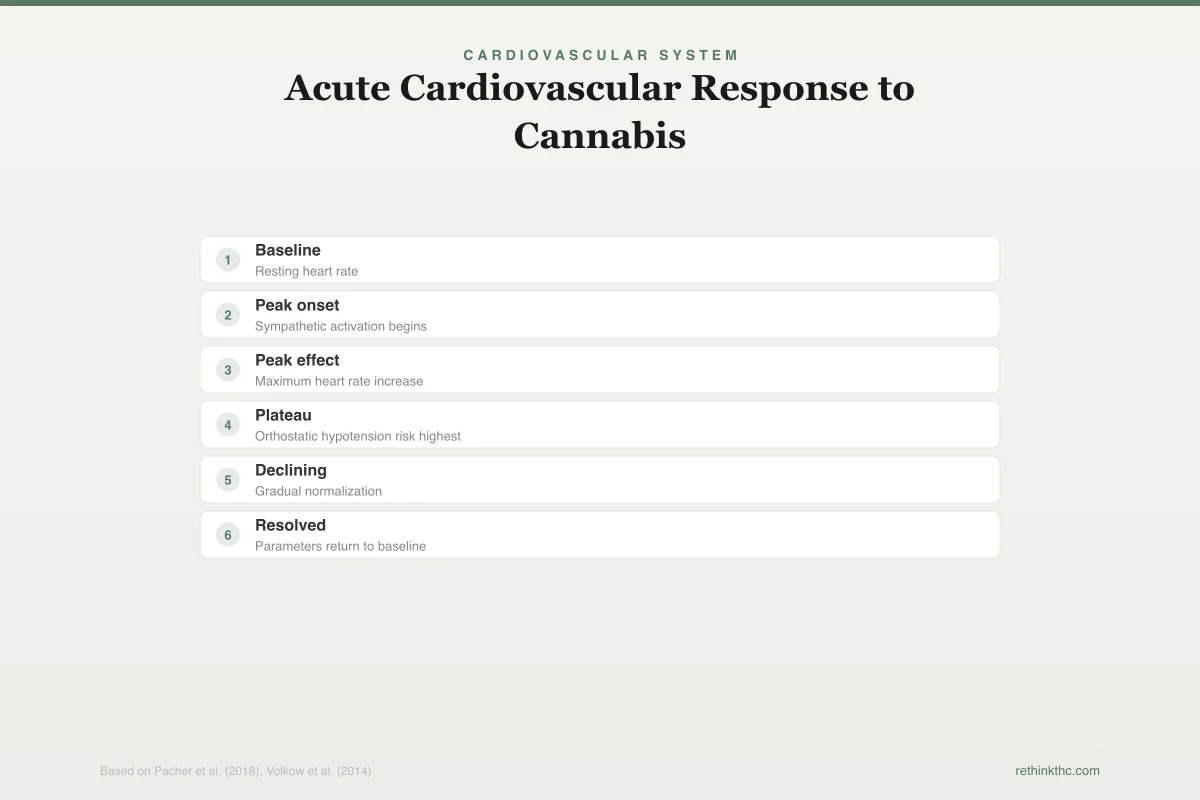
Blood pressure follows a more complex pattern. In the short term, blood pressure may rise slightly while sitting and drop when standing, a phenomenon called orthostatic hypotension (a sudden blood pressure drop when you change position). This is part of why some people feel dizzy or lightheaded when they stand up after using cannabis. Over time, with repeated use, the cardiovascular system develops tolerance to these acute effects, and chronic users typically show a smaller heart rate response than new users.
Cannabis also affects the endothelium (the lining of blood vessels), and some research suggests it may promote inflammation within blood vessel walls. The endocannabinoid system includes CB1 and CB2 receptors distributed throughout cardiovascular tissue, meaning the heart and blood vessels are directly responsive to both the body's own endocannabinoids and external cannabinoids like THC and CBD.
For a healthy 25-year-old, a temporary increase in heart rate is unlikely to cause problems. Your cardiovascular system has the reserve capacity to handle it. But if you already have narrowed coronary arteries, an irregular heartbeat, uncontrolled high blood pressure, or other cardiovascular vulnerabilities, the math changes.
The Volkow 2014 Review: Heart Attack Risk in the First Hour
One of the most widely cited findings on cannabis and heart health comes from a 2014 review by Volkow and colleagues, published in the New England Journal of Medicine. This was a comprehensive review of the adverse health effects of cannabis, covering addiction risk, cognitive effects, mental health, and cardiovascular outcomes.
On the cardiovascular front, the review noted that the risk of myocardial infarction (heart attack) appeared to be elevated during the first hour after cannabis use. The proposed mechanism is straightforward: the combination of increased heart rate, altered blood pressure, and potential effects on blood vessel function could, in someone with pre-existing cardiovascular vulnerability, tip the balance toward an acute event.
This finding gets a lot of attention, and it should. But several important qualifications are necessary. The evidence came primarily from case reports and small studies, not large randomized trials. The people who experienced cardiac events after cannabis use typically had pre-existing risk factors. And the risk elevation was described as occurring within a narrow time window (the first hour), not as a persistent, ongoing risk from chronic use.
To put it in context: exercise also temporarily increases heart rate and blood pressure, and the risk of heart attack is similarly elevated during and immediately after vigorous physical activity. That does not make exercise dangerous for most people. It does mean that people with significant cardiovascular disease need to be cautious about activities that acutely stress the heart, and cannabis use is one of those activities.
The 2023 Meta-Analysis: No Significant Link in Pooled Data
The most important recent contribution to this question is a 2023 meta-analysis by Theerasuwipakorn and colleagues.[1] This was not a single study or a narrative review. It was a systematic pooling of data from 20 studies involving approximately 183 million patients, making it the largest analysis of cannabis and cardiovascular outcomes to date.
The headline findings challenge the assumption that cannabis is clearly harmful to the heart. In the pooled analysis, cannabis use was not significantly associated with either acute myocardial infarction (heart attack) or stroke. The odds ratio for heart attack was 1.29, meaning cannabis users showed a 29% higher rate, but this result did not reach statistical significance, meaning the researchers could not rule out that the difference was due to chance. The odds ratio for stroke was 1.35, also not statistically significant.
This does not prove that cannabis is safe for the heart. It means that when you combine data from the largest available studies, covering millions of patients, the signal for cardiovascular harm is not strong or consistent enough to reach the threshold for statistical confidence. The difference between "not proven harmful" and "proven safe" is important. The data is noisy, the studies used different methods, and confounding variables (like tobacco co-use, which is extremely common among cannabis users) are difficult to fully separate out.
What the Theerasuwipakorn meta-analysis does tell us is that if cannabis increases cardiovascular risk, the effect is probably modest in the general population and may be concentrated in specific high-risk subgroups rather than applying broadly to all users.
Why the Research Is So Mixed
Several factors explain why cannabis cardiovascular research has produced conflicting results.
Tobacco confounding. Many cannabis users also smoke tobacco, which is one of the strongest established risk factors for heart disease and stroke. Separating the cardiovascular effects of cannabis from the cardiovascular effects of co-used tobacco is extremely difficult, and not all studies have done this adequately.
Smoking as a delivery method. Combustion produces carbon monoxide, particulate matter, and other byproducts that are harmful to blood vessels regardless of whether the material being burned is cannabis or tobacco. Studies that examine smoked cannabis are measuring the combined effect of THC plus combustion byproducts. Research on edibles or vaporized cannabis might show different cardiovascular profiles, but this data is limited.
Study design limitations. Most cardiovascular cannabis research is observational, meaning researchers look at associations in existing data rather than randomly assigning people to use or not use cannabis. Observational studies can identify correlations but cannot definitively establish causation. People who use cannabis may differ from non-users in diet, exercise, stress levels, healthcare utilization, and dozens of other factors that affect heart health.
Potency changes. A 2016 analysis by ElSohly and colleagues, published in Biological Psychiatry,[2] showed that average THC content roughly tripled between 1995 and 2014, rising from about 4% to about 12%. Most of the cardiovascular research was conducted during or before this potency escalation. Whether higher-potency products carry different cardiovascular risks is largely unstudied. This is especially relevant given that today's concentrates and high-potency products deliver far more THC per session than the cannabis used in earlier research.
Who Is at Higher Risk
While the overall population-level data does not show a clear signal, certain groups likely face elevated cardiovascular risk from cannabis use.
People with existing heart conditions. If you have coronary artery disease, heart failure, a history of heart attack, or arrhythmias (irregular heartbeat), the acute effects of cannabis on heart rate and blood pressure carry more significance. A healthy heart can absorb a temporary increase in workload. A compromised heart may not.
Older users. Cardiovascular risk accumulates with age, and older adults are more likely to have subclinical (not yet diagnosed) heart disease. The growing population of older cannabis users, including many who are returning to cannabis after decades away, faces a different risk profile than younger users.
Heavy, daily users. While tolerance develops to some of cannabis's cardiovascular effects, chronic heavy use means repeated cycles of cardiovascular stimulation. Whether this cumulative stress contributes to long-term vascular changes is not well established, but it is biologically plausible.
People who combine cannabis with stimulants. Using cannabis alongside cocaine, amphetamines, or high doses of caffeine compounds the cardiovascular stress. The combination of a stimulant-driven heart rate increase with cannabis-related cardiovascular changes creates a higher-risk scenario than either substance alone.
Safety
ModerateIf you have an existing heart condition
Concern
While population-level data doesn't show a clear link between cannabis and cardiac events, the acute effects (20-100% heart rate increase, blood pressure changes, potential vessel inflammation) carry real significance for people with coronary artery disease, arrhythmias, heart failure, or uncontrolled hypertension.
What the research says
The risk appears concentrated in the first hour after use and in people with pre-existing cardiovascular vulnerability. For most healthy young users, the acute spike is comparable to exercise. For at-risk populations, it's a meaningful additional stressor.
Particularly relevant for: People with known heart disease, uncontrolled high blood pressure, arrhythmias, or those over 40 with cardiovascular risk factors
What to do
Talk to your cardiologist before using cannabis in any form. If you experience chest pain, palpitations, sudden weakness, or difficulty speaking during or after use, call 911 immediately.
Volkow et al. (2014), New England Journal of Medicine
Practical Harm Reduction for Heart Health
If you use cannabis and want to minimize cardiovascular risk, several evidence-informed strategies can help.
Know your baseline. If you are over 40, have a family history of heart disease, or have risk factors like high blood pressure, high cholesterol, or diabetes, get a cardiovascular checkup. Knowing your baseline health allows you to make more informed decisions about cannabis use.
Avoid combining cannabis with tobacco. The cardiovascular harms of tobacco are well established. Smoking methods that involve tobacco (like spliffs or blunts) add proven cardiovascular risk on top of whatever risk cannabis itself carries.
Consider non-smoked methods. Edibles and tinctures eliminate the combustion byproducts that damage blood vessels. They still produce the THC-related cardiovascular effects (heart rate increase, blood pressure changes), but they remove the carbon monoxide and particulate matter exposure.
Be cautious with high-potency products. Higher THC doses produce more pronounced acute cardiovascular effects. Lower-potency options and slower titration reduce the cardiovascular spike.
Do not ignore symptoms. Chest pain, pressure, shortness of breath, palpitations, or sudden dizziness during or after cannabis use warrant medical attention, especially if you have cardiovascular risk factors. Cannabis can mask pain perception, so take any cardiac-type symptoms seriously even if you feel calm.
The Bottom Line on Cannabis and Heart Health
The honest summary of the current research is this: cannabis acutely stresses the cardiovascular system, and there is reason to believe this matters more for people who already have heart disease or significant risk factors. For a broader look at how cannabis affects your body across all major systems — lungs, hormones, immunity, metabolism, and more — see cannabis and your body: what the research shows. But the largest pooled analysis of the available data, covering 183 million patients across 20 studies, did not find a statistically significant association between cannabis use and heart attack or stroke in the general population.
This is a topic where the science is genuinely unsettled. Anyone who tells you cannabis is definitely dangerous for your heart is overstating the evidence. Anyone who tells you it is definitely safe is also overstating the evidence. The most responsible position is somewhere in between: be aware of the acute effects, know your own risk factors, and make choices accordingly.
When to Seek Professional Help
If you experience chest pain, heart palpitations, shortness of breath, sudden weakness or numbness on one side of your body, difficulty speaking, or severe headache during or after cannabis use, seek emergency medical attention. These could be signs of a cardiac event or stroke, and prompt treatment dramatically improves outcomes.
If you have a known heart condition and are using or considering using cannabis, talk to your cardiologist. Many providers are increasingly open to honest conversations about cannabis use, and they can help you weigh the risks based on your specific cardiovascular profile.
If you are finding it difficult to reduce or stop cannabis use despite wanting to, support is available. Understanding the signs of cannabis use disorder is a good starting point, and a tolerance break can help reset your relationship with cannabis.
SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day, 7 days a week. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
The Bottom Line
Cannabis acutely increases heart rate by 20 to 100% and may elevate heart attack risk in the first hour after use, particularly in people with pre-existing cardiovascular conditions. However, the largest pooled analysis to date, a 2023 meta-analysis of 20 studies covering 183 million patients, found no statistically significant association between cannabis use and heart attack or stroke in the general population. The research is genuinely mixed due to tobacco confounding, combustion byproducts, study design limitations, and the tripling of cannabis potency since the mid-1990s. Higher-risk groups include people with existing heart conditions, older users, heavy daily users, and those combining cannabis with stimulants. Harm reduction strategies include knowing your cardiovascular baseline, avoiding tobacco co-use, choosing non-smoked methods, and using lower-potency products.
Sources & References
- 1RTHC-04980·Theerasuwipakorn, Nonthikorn (2023). “Cannabis and Heart Attack/Stroke Risk: A 183-Million-Patient Meta-Analysis Finds Stroke Risk but Not Heart Attack Risk.” Toxicology Reports.Study breakdown →PubMed →↩
- 2RTHC-01144·ElSohly, Mahmoud A. et al. (2016). “U.S. Cannabis Potency Tripled Over Two Decades While CBD Nearly Vanished.” Biological Psychiatry.Study breakdown →PubMed →↩