10 Lower-Risk Cannabis Use Guidelines (Based on Published Research)
Harm Reduction & Moderation
10 Guidelines
The peer-reviewed Lower-Risk Cannabis Use Guidelines list age of initiation as the top risk factor, backed by the PNAS finding that persistent teen use was linked to an 8-point IQ drop that never fully recovered.
Fischer et al., American Journal of Public Health, 2017; Meier et al., PNAS, 2012
Fischer et al., American Journal of Public Health, 2017; Meier et al., PNAS, 2012
View as imageIf you only read one thing
A team of researchers published 10 evidence-based guidelines for reducing cannabis-related harm — not requiring you to quit, just making smarter choices. The three biggest levers: don't use daily, choose lower-THC products, and don't smoke it (vape or eat it instead). Starting after age 18 is also huge — teen use was linked to an IQ drop that never fully came back. You don't have to follow all 10. Each one you adopt cuts a specific, documented risk.
You already know cannabis is not risk-free. You have probably read conflicting advice that ranges from "it is basically medicine" to "it will ruin your life." What you may not have seen is a set of safer cannabis use guidelines that actually come from published research, not opinion columns or government scare campaigns.
That is exactly what exists. In 2017, a team led by Benedikt Fischer published the Lower-Risk Cannabis Use Guidelines (LRCUG) in the American Journal of Public Health, synthesizing the available evidence into 10 actionable recommendations for reducing cannabis-related health risks. These are specific, evidence-based recommendations designed not to eliminate cannabis use but to reduce the harms most strongly supported by scientific evidence. Think of them as harm reduction for cannabis, the same approach that public health has long applied to alcohol, sex, and driving.
Here are all 10, with the science behind each one.
Key Takeaways
- The Lower-Risk Cannabis Use Guidelines (LRCUG) are a peer-reviewed set of 10 evidence-based recommendations published in the American Journal of Public Health in 2017
- Waiting to use cannabis until at least age 16 — ideally 18 or later — significantly cuts the risk of lasting cognitive and developmental effects
- Choosing lower-THC products, avoiding synthetic cannabinoids, and skipping combustion methods are three of the most impactful changes a person can make
- Daily or near-daily use is the single strongest behavioral predictor of cannabis-related health problems
- These guidelines do not require quitting — they focus on reducing specific, well-documented risks while respecting personal choice
- The Meier et al. (2012, PNAS) Dunedin study found persistent adolescent cannabis use was linked to an average IQ drop of up to 8 points that did not fully recover after quitting, which is why age of initiation is one of the most consequential risk factors
1. Delay Cannabis Use Until Adulthood
The single most protective thing a young person can do is wait. The LRCUG recommend delaying use until at least age 16, with the stronger recommendation being to wait until 18 or later.
The checklist below summarizes all 10 guidelines at a glance, with the ones you can act on immediately highlighted.
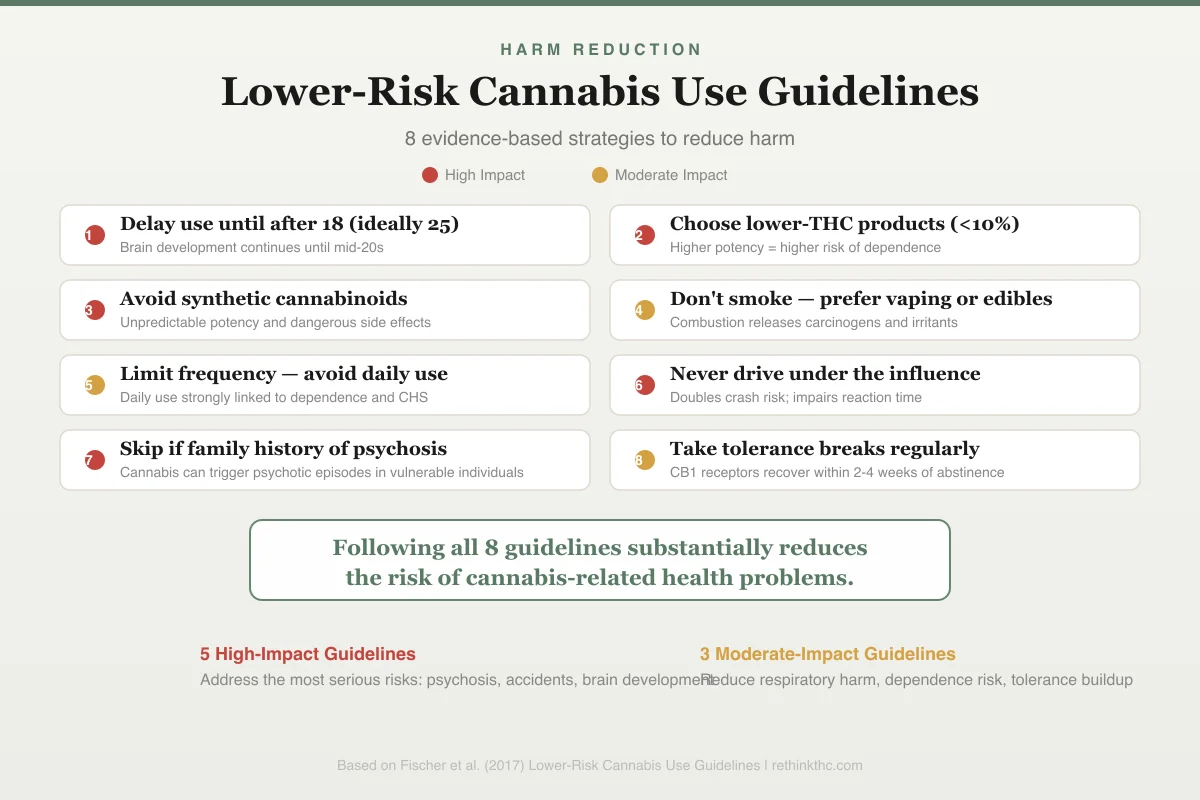
Harm Reduction
Lower-Risk Cannabis Use Guidelines
8 evidence-based strategies to reduce harm
Delay use until after 18 (ideally 25)
Brain development continues until mid-20s
Choose lower-THC products (<10%)
Higher potency = higher risk of dependence
Avoid synthetic cannabinoids
Unpredictable potency and dangerous side effects
Don't smoke — prefer vaping or edibles
Combustion releases carcinogens and irritants
Limit frequency — avoid daily use
Daily use strongly linked to dependence and CHS
Never drive under the influence
Doubles crash risk; impairs reaction time
Skip if family history of psychosis
Cannabis can trigger psychotic episodes in vulnerable individuals
Take tolerance breaks regularly
CB1 receptors recover within 2-4 weeks of abstinence
The reason is neurodevelopment. Your brain is not fully developed until your mid-20s, and the endocannabinoid system (the network of receptors that THC directly acts on) plays a critical role in how the brain wires itself during adolescence. A landmark study by Meier and colleagues, published in 2012 in the Proceedings of the National Academy of Sciences, followed over 1,000 people from birth to age 38 and found that persistent cannabis use starting in adolescence was associated with an average IQ decline of up to 8 points that did not fully recover after quitting.[1]
The developing brain is simply more vulnerable. If you are a parent or a young person weighing this decision, the research on cannabis and the developing brain goes deeper into why timing matters so much.
2. Choose Lower-THC Products
Not all cannabis is created equal. THC concentration has risen dramatically over the past two decades[7], and higher-potency products are consistently linked to greater risk.
A 2019 study by Di Forti and colleagues, published in The Lancet Psychiatry, found that daily use of high-potency cannabis (above 10% THC) was associated with a fivefold increase in the risk of a first episode of psychosis compared to never using.[2] Lower-potency products carried a fraction of that risk.
The LRCUG recommend choosing products with lower THC concentrations and considering products with higher CBD-to-THC ratios. CBD does not produce intoxication and appears to partially buffer some of THC's negative effects on anxiety and cognition. Microdosing cannabis is one practical way to apply this recommendation while still getting functional benefit from lower amounts. The steady climb in THC potency over time makes this recommendation more relevant now than when the guidelines were first published. And if you have ever wondered what the healthiest way to consume THC actually looks like from a harm reduction standpoint, the answer depends on balancing potency, delivery method, and frequency.
3. Avoid Synthetic Cannabinoids Entirely
This one is straightforward. Synthetic cannabinoids (sold under names like K2, Spice, or various branded labels) are not cannabis. They are lab-made chemicals sprayed onto plant material, designed to bind to the same receptors as THC but often with far greater potency and unpredictable effects.
The LRCUG classify synthetic cannabinoids as a clear "avoid" category. Public health agencies including the CDC have documented clusters of severe adverse events including seizures, kidney damage, psychosis, and death linked to synthetic cannabinoid use. These products are not regulated, not tested, and not safe. There is no "lower-risk" version of a synthetic cannabinoid.
If you use cannabis, use actual cannabis.
4. Avoid Smoking Combusted Cannabis (Choose Safer Methods)
Burning plant material and inhaling the smoke exposes your lungs to many of the same toxicants found in tobacco smoke, including tar, carbon monoxide, and volatile organic compounds. A 2022 review confirmed that habitual cannabis smoking is associated with chronic bronchitis symptoms and airway inflammation, though notably, cannabis smoke does not appear to cause COPD and probably does not cause lung cancer — a different respiratory profile from tobacco.[3]
The LRCUG recommend avoiding combustion entirely when possible. Vaporizers that heat cannabis to a temperature that releases cannabinoids without burning the plant matter reduce exposure to combustion byproducts. Edibles and oils eliminate inhalation risks altogether, though they come with their own considerations (slower onset, harder to dose, longer duration).
If you want a deeper comparison of delivery methods and their trade-offs, the article on the healthiest way to consume cannabis covers the options in detail. Consuming too much too quickly is one of the most common ways people end up greening out, which is the informal term for the acute adverse reaction to THC overconsumption.
5. Avoid Deep Inhalation and Breath-Holding
This one surprises people. Many cannabis users have been taught to inhale deeply and hold the smoke or vapor in their lungs to "get more out of it." The science does not support this practice.
Research has shown that holding smoke in your lungs for 10 or 20 seconds does not meaningfully increase THC absorption compared to holding for just a few seconds. The vast majority of THC is absorbed within the first few seconds of inhalation. What extended breath-holding does increase is exposure to tar and toxic gases.
The lightheadedness people associate with deeper hits is largely caused by oxygen deprivation, not a stronger high. The LRCUG recommend taking shallow puffs and breathing normally. You are not losing potency. You are just reducing the amount of harmful material your lungs absorb.
6. Limit Frequency of Use
This is arguably the most important behavioral recommendation in the entire framework. Frequency of use is the strongest predictor of cannabis-related problems, stronger than the amount used per session.
The LRCUG specifically recommend avoiding daily or near-daily use. A 2020 meta-analysis found that approximately 47 percent of regular cannabis users experience clinically significant withdrawal symptoms when they stop[6], with the risk scaling directly with frequency of use. Daily use is the pattern most strongly associated with dependence, cognitive impairment, and mental health complications.
Occasional use (once a week or less) carries substantially lower risk across nearly every outcome studied. If you are currently using daily and want practical strategies for pulling back, the guide on how to cut back on weed without quitting walks through specific, realistic approaches. A structured tolerance break is another option that can reset your CB1 receptors without requiring a permanent change, and the complete T-break guide covers the science and logistics in detail. Understanding the optimal tolerance break length can help you plan a reset that fits your situation. For a stark picture of what daily or near-constant use does to the body and brain over time, see what happens to your body when you are high 24/7 for months.
The pattern matters more than the amount. Using a small quantity every day is riskier than using a larger quantity once a week.
7. Never Drive Under the Influence of Cannabis
Cannabis impairs reaction time, divided attention, and lane tracking. These are not debatable findings. They are consistent across dozens of studies using driving simulators, on-road assessments, and crash-risk analyses.
The spectrum below shows how different use patterns map to different risk levels, from lowest-risk occasional use to highest-risk daily heavy use.
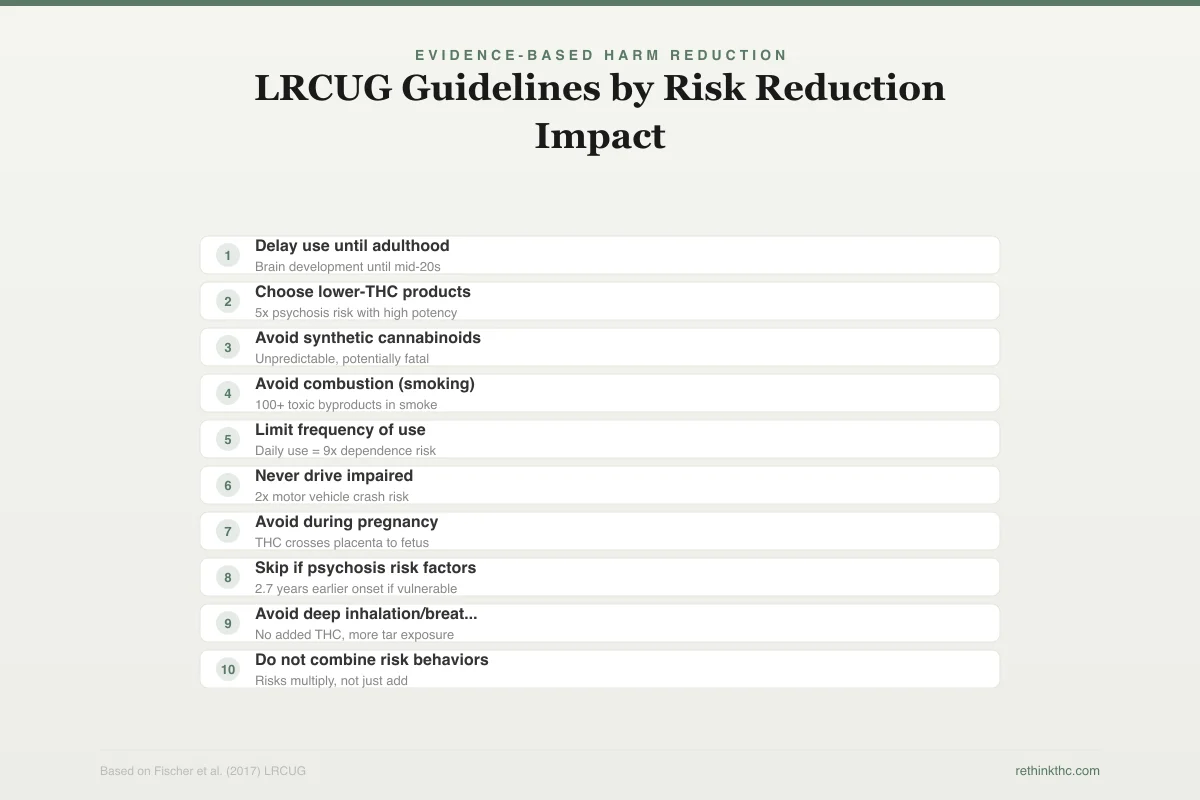
Evidence-Based Harm Reduction
LRCUG Guidelines by Risk Reduction Impact
10 recommendations ranked by impact and evidence quality
Impact:
Evidence:
Delay use until adulthood
Brain development until mid-20s
Choose lower-THC products
5x psychosis risk with high potency
Avoid synthetic cannabinoids
Unpredictable, potentially fatal
Avoid combustion (smoking)
100+ toxic byproducts in smoke
Limit frequency of use
Daily use = 9x dependence risk
Never drive impaired
2x motor vehicle crash risk
Avoid during pregnancy
THC crosses placenta to fetus
Skip if psychosis risk factors
2.7 years earlier onset if vulnerable
Avoid deep inhalation/breath-holding
No added THC, more tar exposure
Do not combine risk behaviors
Risks multiply, not just add
A 2012 meta-analysis by Asbridge and colleagues, published in the BMJ, found that recent cannabis use was associated with a roughly twofold increase in the risk of a motor vehicle collision.[4] The impairment is most pronounced in the first three to four hours after use, though some residual effects can persist longer, especially with edibles or high doses.
The LRCUG recommend not driving for at least six hours after inhalation. For edibles, the window should be longer because of delayed onset and extended duration. Combining cannabis with alcohol before driving multiplies the impairment beyond what either substance causes alone.
This is one of the clearest, least ambiguous findings in cannabis research. Do not drive high. Beyond the health risks, the legal consequences are significant and vary widely by state. Our complete guide to cannabis law and your rights covers DUI laws, per se THC limits, and what happens if you are pulled over.
8. Avoid Cannabis Use During Pregnancy
The endocannabinoid system is deeply involved in fetal brain development. THC crosses the placenta and can reach the developing fetus, and emerging evidence suggests this exposure may affect neurodevelopmental outcomes.
Research has consistently linked prenatal cannabis exposure to lower birth weight, increased likelihood of neonatal intensive care admission, and subtle but measurable effects on attention, problem-solving, and behavior in children exposed in utero.
The LRCUG recommend avoiding cannabis use during pregnancy and breastfeeding. While the evidence base is still developing (ethical constraints make randomized trials impossible), the precautionary principle applies. The potential risks to a developing fetus are not worth the benefits of use during a finite period.
9. Avoid Cannabis Use with Personal or Family History of Psychosis
Not everyone faces the same level of risk from cannabis. People with a personal history of psychotic symptoms or a first-degree family member (parent or sibling) with a psychotic disorder like schizophrenia are at substantially elevated risk of cannabis-triggered psychotic episodes.
The Di Forti 2019 Lancet Psychiatry study found that the association between high-potency cannabis and psychosis was particularly strong in populations with genetic vulnerability.[2] Multiple studies have found that cannabis use is associated with earlier onset of psychotic symptoms, potentially by several years, with the risk increasing substantially in those with genetic vulnerability.
The LRCUG recommend that people with these risk factors avoid cannabis entirely. This is the one recommendation in the framework that leans toward abstinence rather than moderation, and the evidence supports that position. For a full breakdown of the research, see the article on cannabis-induced psychosis.
Safety
CriticalPsychosis risk with family history
Concern
People with a personal history of psychotic symptoms or a first-degree family member with schizophrenia face substantially elevated risk from cannabis use. Daily high-potency use was linked to nearly 5 times the odds of a first psychotic episode in the general population — the risk is even higher for those with genetic vulnerability.
What the research says
This is the one guideline where the recommendation is abstinence, not moderation. The Di Forti 2019 study found that if high-potency cannabis were unavailable, up to 50% of first-episode psychosis cases in high-prevalence cities could be prevented.
Particularly relevant for: Anyone with a personal or family history of psychosis or schizophrenia
What to do
If you have a parent or sibling with a psychotic disorder, the safest choice is to avoid cannabis entirely. If you experience unusual perceptual changes, paranoia, or disordered thinking after using cannabis, stop use and talk to a mental health professional.
Di Forti et al. (2019), The Lancet Psychiatry
10. Do Not Combine Risk Behaviors
Each of the previous nine recommendations addresses a single risk factor. The final guideline addresses the reality that risks compound.
Using high-potency cannabis daily, through combustion, with deep inhalation, and then driving afterward is not simply adding risks together. It is multiplying them. The LRCUG emphasize that combining multiple risk behaviors dramatically increases the probability of negative outcomes.
If you have ever experienced the rapid onset of nausea, dizziness, and disorientation after combining cannabis with alcohol, you may have been greening out. Knowing how to avoid greening out through proper dosing and pacing is one of the most practical applications of this guideline. If someone around you is going through it, understanding how to help someone who is greening out can make the difference between a managed episode and an unnecessary emergency room visit.
A 2009 study by Ramaekers and colleagues, published in the Journal of Psychopharmacology, demonstrated that the combination of cannabis and alcohol produced impairment greater than either substance alone[5], with pronounced effects on tracking, reaction time, and divided attention.
The practical takeaway: if you are not ready to follow all 10 guidelines, start with the ones that overlap with your current behavior. Reducing even two or three compounding risks makes a measurable difference.
How These Guidelines Differ from Abstinence-Only Messaging
Traditional drug education tends to treat any use as equally dangerous. The LRCUG take a fundamentally different approach. They acknowledge that millions of people use cannabis and will continue to do so regardless of legal status or public messaging. Given that reality, providing evidence-based strategies to reduce harm is more effective than repeating "just say no."
This is the same logic behind seatbelt laws (we did not ban cars), condom distribution (we did not ban sex), and moderate drinking guidelines (we did not ban alcohol). Public health works best when it meets people where they are. In fact, some researchers are studying whether cannabis itself can serve as harm reduction for people transitioning away from more dangerous substances like opioids or alcohol, and there is a growing body of evidence around using weed to quit opioids specifically.
The LRCUG have been endorsed or adapted by public health agencies in Canada, where they were originally developed, and have influenced cannabis policy frameworks in multiple countries. They represent the scientific consensus on what the modifiable risk factors actually are.
When to Seek Professional Help
Following harm reduction guidelines is a strong starting point. But if you find that you cannot follow them despite wanting to, that gap between intention and behavior is worth paying attention to. If you have tried to cut back repeatedly without success, the how to quit weed guide covers the full process, and talking to a professional can help you understand what is driving the pattern.
Consider reaching out to a professional if you have tried to cut back or change your patterns repeatedly without success, if your cannabis use is interfering with work, relationships, or responsibilities, or if you are using primarily to manage anxiety, depression, or other mental health symptoms.
The SAMHSA National Helpline at 1-800-662-4357 is free, confidential, available 24/7, and can connect you with local treatment and support resources. You do not need to be in crisis to call.
Moving Forward with Better Information
These 10 guidelines are not about perfection. They are about giving you the information to make choices that are actually informed by evidence rather than by cultural myths, marketing, or outdated scare tactics.
You do not have to follow all 10 to benefit. Each one you adopt reduces a specific, documented risk. Start with the ones that are most relevant to your situation, and build from there. If you want a time-limited experiment to see how these changes feel, Sober October for weed offers a structured framework for taking a temporary break. If sleep is the main reason you use, be aware that using weed to sleep every night carries its own set of long-term consequences that the research documents clearly. The goal is not to judge your choices. It is to make sure your choices are based on what the science actually shows.
The Bottom Line
These are 10 evidence-based guidelines for reducing cannabis-related harm without requiring abstinence. You do not have to follow all 10 to benefit — each one you adopt reduces a specific, documented risk. The biggest levers are limiting how often you use, choosing lower-potency products, avoiding combustion, and delaying use until adulthood. They follow the same public health logic as moderate drinking guidelines or seatbelt laws: not a demand to stop, but a way to make informed decisions about the risks you are actually taking.
Sources & References
- 1RTHC-00591·Meier, Madeline H. et al. (2012). “From Teen Years to 38: Heavy, Long-Term Cannabis Use Tracked With Lower Cognitive Scores.” Proceedings of the National Academy of Sciences (PNAS).Study breakdown →PubMed →↩
- 2RTHC-02010·Di Forti, Marta et al. (2019). “Daily High-Potency Cannabis Use and Psychosis Risk: The Largest European Study Drew a Direct Line.” The Lancet Psychiatry.Study breakdown →PubMed →↩
- 3RTHC-03941·Joshi, Manish et al. (2022). “Marijuana causes bronchitis but probably does not cause COPD or lung cancer.” The Medical clinics of North America.Study breakdown →PubMed →↩
- 4RTHC-00540·Asbridge, Mark et al. (2012). “Meta-analysis: cannabis use nearly doubles motor vehicle crash risk.” BMJ (Clinical research ed.).Study breakdown →PubMed →↩
- 5RTHC-00385·Ramaekers, J G et al. (2009). “Heavy Cannabis Users Showed Much Less Cognitive Impairment from THC Than Occasional Users.” Journal of psychopharmacology (Oxford.Study breakdown →PubMed →↩
- 6RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩
- 7RTHC-01144·ElSohly, Mahmoud A. et al. (2016). “U.S. Cannabis Potency Tripled Over Two Decades While CBD Nearly Vanished.” Biological Psychiatry.Study breakdown →PubMed →↩