Does CBD Actually Work for Anxiety? What the Evidence Shows
Balanced Cannabis Science
300mg
A 2015 review found strong preclinical evidence for CBD across five anxiety disorders, but effective research doses of 300 to 600 mg are far higher than what most commercial CBD products actually deliver.
Blessing et al., Neurotherapeutics, 2015
Blessing et al., Neurotherapeutics, 2015
View as imageIf you only read one thing
CBD probably does something real for anxiety — animal studies are consistently positive, and the brain pathways make sense. But here's the catch: the research uses 300 to 600 mg doses, and your gummy has 25 mg. We don't have large human trials yet that prove it works for diagnosed anxiety disorders. It's not snake oil, but it's also not a proven treatment. If your anxiety is serious, therapy and established meds have far stronger evidence behind them. CBD might help alongside those, but not instead of them.
Millions of people take CBD for anxiety. It is one of the most commonly cited reasons for CBD use in consumer surveys, and the market for CBD products has grown into a multi-billion-dollar industry built largely on the promise of calm without a high. But when you look past the marketing and the anecdotes, the research picture is more complicated than either the CBD industry or its critics suggest.
The honest summary: the preclinical evidence for CBD and anxiety is genuinely promising. Animal studies and early human research show consistent anti-anxiety effects through plausible biological mechanisms. But the clinical evidence, meaning large, well-designed trials in people with diagnosed anxiety disorders, is still thin. This is not a reason to dismiss CBD. It is a reason to understand exactly what we know, what we do not, and what that means if you are considering CBD for your own anxiety.
Key Takeaways
- A 2015 review in Neurotherapeutics found strong preclinical evidence supporting CBD for generalized anxiety disorder, panic disorder, social anxiety disorder, OCD, and PTSD
- Most of that strong evidence comes from animal studies and small human pilots — not the large randomized controlled trials needed to call CBD a proven anxiety treatment
- Effective doses in research (typically 300 to 600 mg) are far higher than what most commercial CBD products actually deliver at their recommended serving sizes
- CBD and THC affect anxiety through completely different pathways, so using high-THC cannabis for anxiety is not the same thing as using CBD
- The CBD market has serious quality control problems — many products contain less CBD than the label says (or more THC than expected)
- CBD should not replace proven treatments like cognitive behavioral therapy or SSRIs, but it may play a role alongside them once large clinical trials confirm how well it works
What the Preclinical Evidence Shows
The most comprehensive review of CBD and anxiety was published by Blessing and colleagues in 2015 in Neurotherapeutics.[1] This review examined both animal studies and the limited human clinical data available at the time. Its findings were genuinely notable.
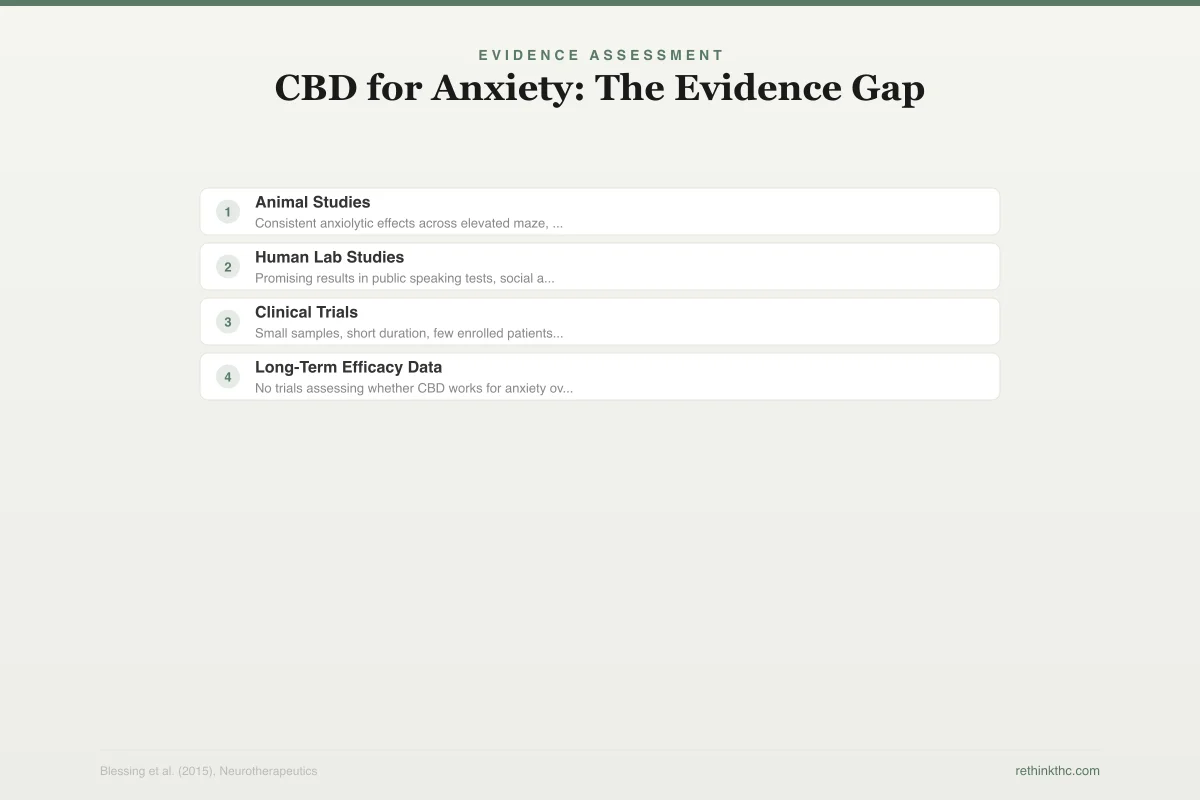
Evidence Assessment
CBD for Anxiety: The Evidence Gap
Strong preclinical signal, but clinical proof thins rapidly
Consistent anxiolytic effects across elevated maze, conflict, and PTSD models
Promising results in public speaking tests, social anxiety paradigms (small samples)
Small samples, short duration, few enrolled patients with diagnosed anxiety disorders
No trials assessing whether CBD works for anxiety over months or years of daily use
In animal models, CBD consistently reduced anxiety-like behaviors across multiple paradigms. Rats and mice given CBD showed less fear in elevated maze tests, less avoidance in conflict tests, and reduced physiological stress responses. These effects were observed across a range of anxiety-relevant models, including those that mimic generalized anxiety, panic, social anxiety, and post-traumatic stress.
The review concluded that preclinical evidence "strongly supports" CBD as a treatment for generalized anxiety disorder, panic disorder, social anxiety disorder, obsessive-compulsive disorder, and PTSD. That is a significant statement from a peer-reviewed journal. It means the biological plausibility is established. CBD does something real to anxiety-related circuits in the brain.
How CBD Appears to Work for Anxiety
Understanding the mechanism helps explain why the preclinical results are taken seriously by researchers.
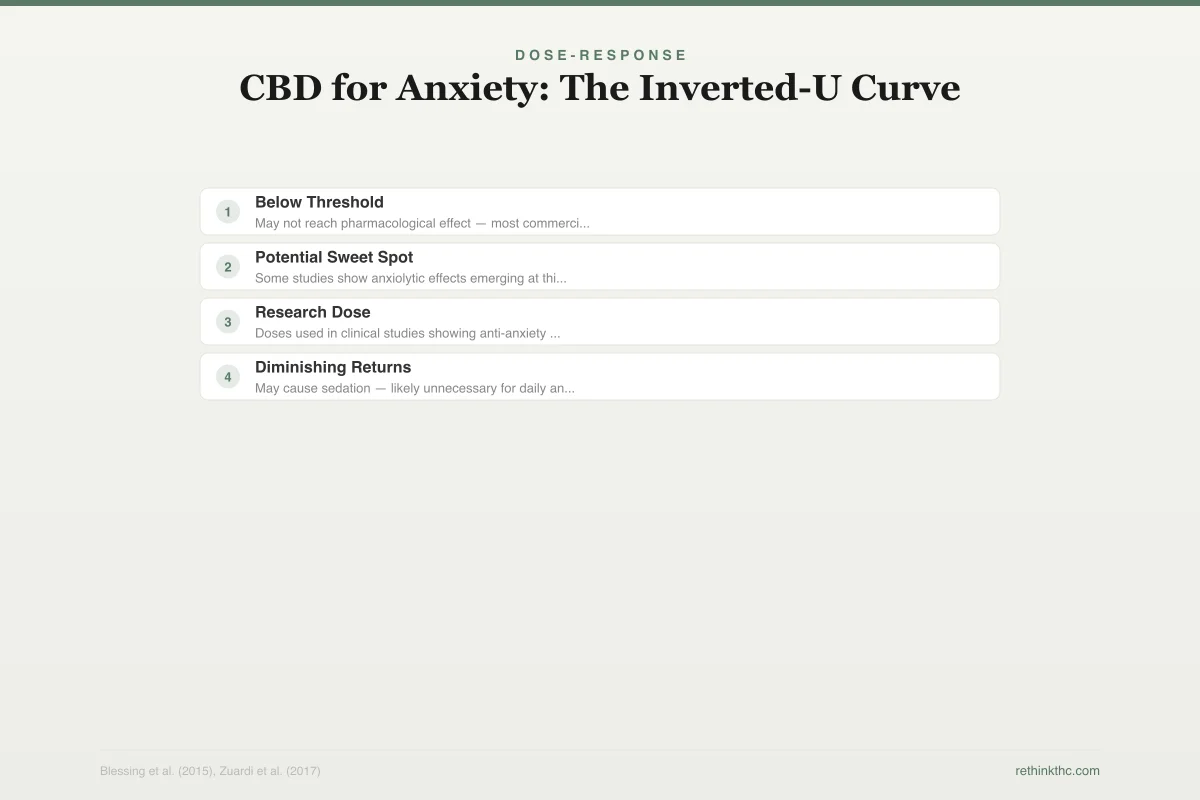
Dose-Response
CBD for Anxiety: The Inverted-U Curve
Too little may not work. Research doses are far above what most products deliver.
< 25 mg
Below Threshold
25–75 mg
Potential Sweet Spot
300–600 mg
Research Dose
> 600 mg
Diminishing Returns
May not reach pharmacological effect — most commercial products are in this range
Some studies show anxiolytic effects emerging at this range for daily use
Doses used in clinical studies showing anti-anxiety effects (single-dose designs)
May cause sedation — likely unnecessary for daily anti-anxiety use
Most commercial CBD products deliver 10–30 mg per serving — a fraction of the 300–600 mg doses that showed effects in research
CBD does not work the way THC does. THC binds directly to CB1 receptors in the brain, which is what produces the high and also what drives the biphasic anxiety effect (low doses calm, high doses panic). CBD takes a different route entirely.
Lu and Mackie's 2016 review of the endocannabinoid system in Biological Psychiatry describes how CBD modulates the system indirectly. Rather than binding to cannabinoid receptors, CBD appears to inhibit the enzyme (FAAH) that breaks down anandamide, your body's own endogenous cannabinoid. This effectively raises your natural anandamide levels, which may promote calm through your body's own regulatory system rather than by flooding it with an external compound.
CBD also interacts with serotonin 5-HT1A receptors, which are directly involved in anxiety regulation and are the same receptors targeted by a class of anti-anxiety medications called buspirone. This serotonin pathway may be responsible for much of CBD's acute anti-anxiety effects observed in preclinical studies.
This dual mechanism, boosting your endocannabinoid tone while modulating serotonin signaling, is pharmacologically interesting because it does not involve the CB1 activation that produces intoxication, cognitive impairment, or dependence. For more on the endocannabinoid system and how it relates to cannabis use, see does weed help anxiety.
The Gap Between Preclinical and Clinical Evidence
Here is where honesty becomes important. Strong preclinical evidence does not automatically translate to effective clinical treatment. The history of medicine is full of compounds that worked beautifully in animal models and then failed in human trials. CBD has not failed in human trials. It simply has not been tested thoroughly enough in the kinds of trials that would prove it works.
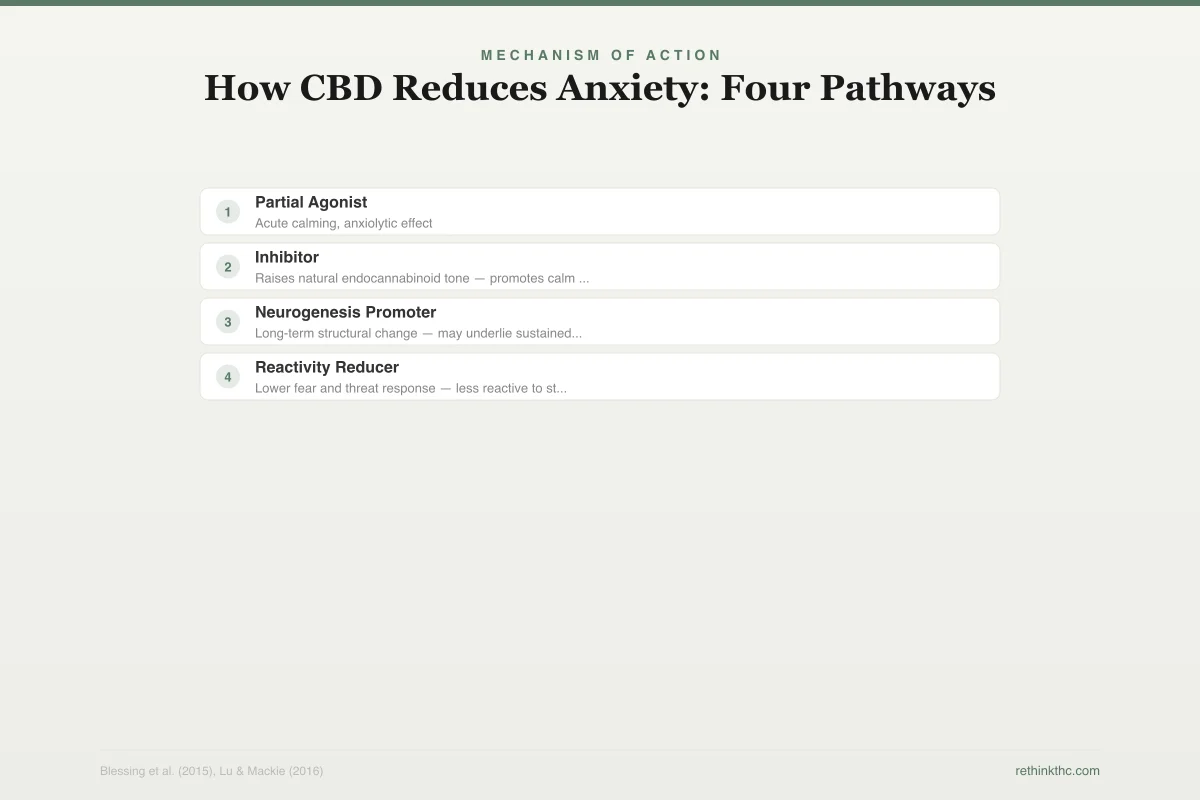
Mechanism of Action
How CBD Reduces Anxiety: Four Pathways
CBD acts through multiple independent mechanisms that converge on anxiety reduction
5-HT1A Receptor
Partial AgonistActivates serotonin receptors — same target as buspirone (anti-anxiety med)
Acute calming, anxiolytic effect
FAAH Enzyme
InhibitorBlocks the enzyme that breaks down anandamide (your body's own cannabinoid)
Raises natural endocannabinoid tone — promotes calm from within
Hippocampus
Neurogenesis PromoterPromotes growth of new neurons in the memory/emotion regulation center
Long-term structural change — may underlie sustained benefits
Amygdala
Reactivity ReducerReduces overactivation of the brain's threat-detection center
Lower fear and threat response — less reactive to stressors
The human studies that do exist are small. Most involve fewer than 100 participants. Many use single-dose designs (giving CBD once and measuring the immediate effect) rather than studying what happens when someone takes CBD daily for weeks or months. Few have enrolled people with formally diagnosed anxiety disorders. Most have short follow-up periods.
As Blessing and colleagues noted in their review, "few studies have been conducted in clinical populations" with anxiety disorders. The evidence is promising in healthy volunteers and in experimental anxiety paradigms (where anxiety is induced in a lab setting). But the leap from "CBD reduced anxiety in 24 healthy adults who were given a stressful public speaking task" to "CBD is an effective long-term treatment for generalized anxiety disorder" is larger than most CBD marketing acknowledges.
This does not mean CBD does not work for anxiety. It means we do not yet have the definitive proof. The preclinical signal is strong enough that the research deserves to be completed, not dismissed. But it also should not be overstated.
| Anxiety Disorder | Preclinical Evidence | Human Clinical Evidence | Research Dose | Status |
|---|---|---|---|---|
| Generalized anxiety | Strong (multiple animal models) | Promising but limited (small studies) | 300-600 mg | Needs large RCTs |
| Social anxiety | Strong | Most human data (public speaking paradigm) | 300-600 mg | Most promising |
| Panic disorder | Strong | Very limited | 300 mg | Early stage |
| PTSD | Strong | Limited pilot data | 300-600 mg | Needs large RCTs |
| OCD | Moderate | Minimal | Unknown | Very early stage |
The Dose Problem
One of the least discussed issues in the CBD-for-anxiety conversation is dosing. The doses used in research studies that showed anti-anxiety effects are typically between 300 and 600 milligrams in a single dose.
Quality Control
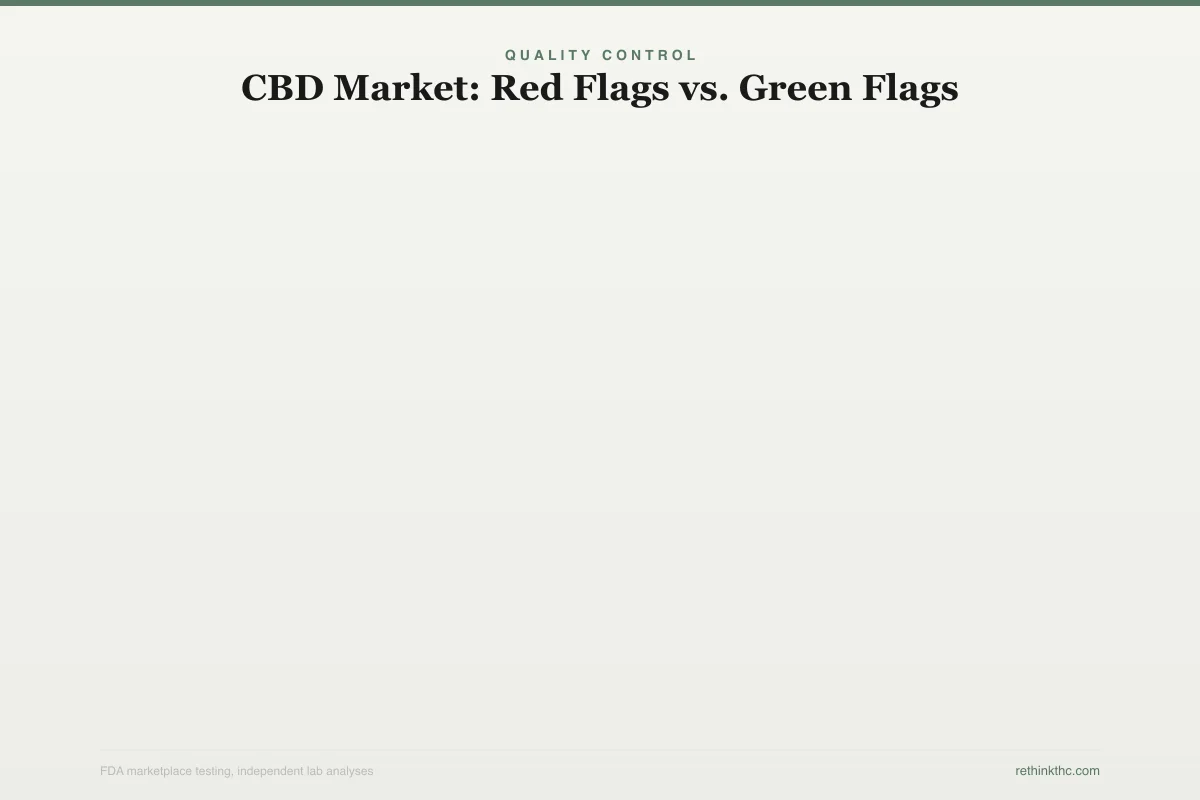
CBD Market: Red Flags vs. Green Flags
FDA testing revealed widespread quality issues in CBD products
Red Flags (FDA Findings)
26% had less CBD than labeled
You may be taking a fraction of the dose you think
43% had more THC than expected
Could trigger anxiety — the opposite of your goal
Heavy metals detected in some products
Lead, arsenic, cadmium from contaminated hemp soil
Pesticide contamination found
Unregulated growing practices in some supply chains
No third-party testing provided
No way to verify what is actually in the product
What to Look For
Third-party COA (Certificate of Analysis)
Independent lab verification of contents
US-grown hemp from licensed farms
Subject to state agricultural regulations
CO2 extraction method
Cleaner extraction, no residual solvents
Clear labeling: full-spectrum vs. isolate
Transparency about what you are getting
Batch-specific test results available
Each production batch independently tested
Look at the label of a typical commercial CBD product. A common tincture might contain 30 milligrams per serving. A gummy might contain 10 to 25 milligrams. That is a fraction of the doses that produced results in clinical research. Someone taking 25 milligrams of CBD per day and expecting the same anti-anxiety effects seen with 600 milligrams in a controlled study is comparing different things entirely.
This dose gap raises a real question. Are the millions of people reporting anxiety relief from low-dose CBD experiencing a genuine pharmacological effect, a placebo response, or something in between? We do not have a definitive answer. It is possible that lower doses work for some people through mechanisms not yet fully understood. It is also possible that expectation and ritual play a significant role at those dose levels. The research has not yet sorted this out.
The Quality Control Problem
Beyond dosing, the CBD market has a well-documented quality control problem. Multiple independent analyses have found that many CBD products do not contain what their labels claim. Some contain significantly less CBD than advertised. Some contain more THC than labeled (which is legally and pharmacologically relevant). Some contain contaminants.
This matters for anyone trying to use CBD therapeutically. If you are taking a product that contains half the CBD it claims, you are effectively running an experiment on yourself with an unknown dose of an unknown substance. And if the product contains undisclosed THC, you may be inadvertently using a compound that can worsen anxiety at higher doses, the opposite of what you intended.
For anyone comparing their personal experience with CBD to the research literature, this variability is an important confound. Your experience with Brand A at 30 milligrams per serving may tell you nothing about what Brand B at the same listed dose would do, because the actual CBD content could be dramatically different.
CBD vs. THC for Anxiety: Different Tools, Different Effects
The distinction between CBD and THC is critical in the anxiety context. A 2009 review by Crippa and colleagues in Human Psychopharmacology[2] documented that anxiety and panic attacks are among the most common acute adverse effects of cannabis use. But that finding applies primarily to THC, not CBD.
THC has a well-established biphasic relationship with anxiety: calming at low doses, anxiety-producing at higher doses. CBD does not show this pattern. In the studies reviewed by Blessing and colleagues, CBD reduced anxiety without producing the opposite effect at higher doses. There is no "too much CBD causes panic" finding in the literature.
This means that using whole-plant cannabis (which is primarily THC) for anxiety is a fundamentally different proposition than using isolated CBD. The two should not be conflated, though they frequently are. If you are interested in the broader question of cannabis and anxiety, see weed and anxiety, the full picture. For a detailed comparison of these two compounds, see CBD vs THC, the differences that actually matter.
What We Know and What We Do Not
What the evidence supports:
- CBD has consistent anti-anxiety effects in animal models across multiple anxiety paradigms
- The biological mechanisms are plausible and involve serotonin and endocannabinoid pathways
- Small human studies show promising acute anti-anxiety effects, particularly in experimental stress paradigms
- CBD does not produce intoxication, cognitive impairment, or the biphasic anxiety response seen with THC
What the evidence does not yet support:
- That CBD is a proven, effective long-term treatment for diagnosed anxiety disorders
- That the low doses found in most commercial products produce the same effects seen in clinical research
- That all CBD products deliver what they claim on the label
- That CBD is a substitute for evidence-based anxiety treatments like cognitive behavioral therapy or established medications
What we genuinely do not know:
- The optimal dose, frequency, and duration of CBD for anxiety in clinical populations
- Whether CBD's acute effects in lab settings translate to meaningful long-term symptom reduction
- How individual differences in genetics, baseline anxiety, and endocannabinoid tone affect response to CBD
- Whether CBD works differently for different anxiety disorders (generalized anxiety vs. social anxiety vs. PTSD)
Practical Considerations
If you are considering CBD for anxiety, here are things worth knowing.
The preclinical evidence is real, not fabricated or trivial. CBD is not snake oil. But the clinical evidence is not yet strong enough to say with confidence that it works for diagnosed anxiety disorders in the way that established treatments (therapy, SSRIs) have been proven to work.
If you do try CBD, source matters. Look for products that provide third-party certificates of analysis showing actual cannabinoid content. Be skeptical of health claims on labels. And be aware that the dose in most commercial products is far below what was studied in clinical research.
CBD is not a substitute for professional help if your anxiety is significantly impairing your life. It is reasonable to explore CBD as part of a broader approach, but not as a replacement for treatments with stronger evidence behind them. For more on evidence-based approaches to anxiety and cannabis, see the medical benefits of cannabis.
When to Seek Professional Help
If anxiety is interfering with your daily functioning, relationships, or quality of life, professional evaluation is warranted regardless of whether you are using CBD. Effective, well-studied treatments for anxiety disorders exist, including cognitive behavioral therapy and several classes of medication with large clinical trial support.
If you are using cannabis (THC products) to manage anxiety and finding that you need increasing amounts or cannot stop without significant rebound anxiety, that pattern suggests dependence and is worth discussing with a provider.
The SAMHSA National Helpline is available 24/7 at 1-800-662-4357. It is free, confidential, and provides referrals to local treatment facilities, support groups, and community-based organizations.
The Bottom Line
A 2015 review in Neurotherapeutics found substantial preclinical evidence supporting CBD for generalized anxiety disorder, panic disorder, social anxiety disorder, OCD, and PTSD. CBD appears to work by boosting natural anandamide levels and modulating serotonin receptors, without producing intoxication or dependence. However, the clinical evidence remains thin: most human studies are small, use single doses, and do not enroll people with diagnosed anxiety disorders. Research doses (300 to 600 mg) far exceed typical commercial products (10 to 30 mg per serving), raising questions about whether low-dose CBD produces meaningful pharmacological effects. The CBD market also has quality control problems, with many products containing different cannabinoid levels than labeled. CBD is not snake oil, but it is also not yet proven to the standard of established anxiety treatments.
Sources & References
- 1RTHC-00924·Blessing, Esther M. et al. (2015). “CBD and Anxiety in 2015: Promising Signals, Mostly From Single Doses.” Neurotherapeutics.Study breakdown →PubMed →↩
- 2RTHC-00349·Crippa, Jose Alexandre S. et al. (2009). “Cannabis both calms and panics — the biphasic dose-response explains why the same drug produces opposite anxiety effects.” Human Psychopharmacology: Clinical and Experimental.Study breakdown →PubMed →↩