CBD vs THC: The Differences That Actually Matter
Balanced Cannabis Science
1 Bond
THC and CBD share the same molecular formula but one structural difference changes everything — THC binds directly to CB1 receptors producing a high and driving dependence, while CBD works indirectly with no high and no withdrawal.
ElSohly et al., Biological Psychiatry, 2016
ElSohly et al., Biological Psychiatry, 2016
View as imageIf you only read one thing
THC gets you high. CBD doesn't. That's the biggest difference, but it's not the only one. THC plugs directly into receptors in your brain that produce euphoria, impair memory, and — with regular use — drive tolerance and dependence. CBD works on the same system indirectly, doesn't cause a high, and doesn't appear to be addictive. The practical takeaway: if you're using cannabis for anxiety, sleep, or a medical reason, the THC-to-CBD ratio matters more than how much 'cannabis' you're taking.
CBD and THC are the two most discussed compounds in cannabis, and most people treat them as interchangeable parts of the same plant. They are not. These two molecules have different shapes, bind to different targets in your brain, produce different effects, carry different risks, and sit in very different legal categories. Confusing them leads to bad decisions, whether you are using cannabis recreationally, considering it medically, or trying to quit.
This article covers what actually differs between CBD and THC, what the research supports for each, and why the shifting ratio between them in modern cannabis products has changed the experience of using cannabis in ways most people do not realize.
Key Takeaways
- THC and CBD are both cannabinoids from the same plant, but THC plugs directly into CB1 receptors in the brain (producing a high) while CBD works on the endocannabinoid system indirectly (no high)
- A 2015 JAMA meta-analysis of 79 trials found moderate evidence for THC-based cannabinoids in chronic pain, and a separate 2015 review found promising early evidence for CBD in anxiety disorders
- Average THC potency in cannabis tripled between 1995 and 2014 while CBD content dropped, so most modern cannabis products are heavily THC-dominant
- The ratio of THC to CBD in a product may matter more than the amount of either one alone, though research on this "entourage effect" is still early
- Understanding the difference between these two compounds is essential for making informed decisions about cannabis use — whether medical or recreational
- CBD does not produce tolerance, dependence, or withdrawal, while THC drives all three — making this distinction critical for anyone worried about cannabis use disorder
Same Plant, Different Molecules
Both THC (tetrahydrocannabinol) and CBD (cannabidiol) are cannabinoids, a class of chemical compounds found in the cannabis plant. The plant produces over 100 different cannabinoids, but THC and CBD are by far the most abundant and the most studied.
Head-to-Head
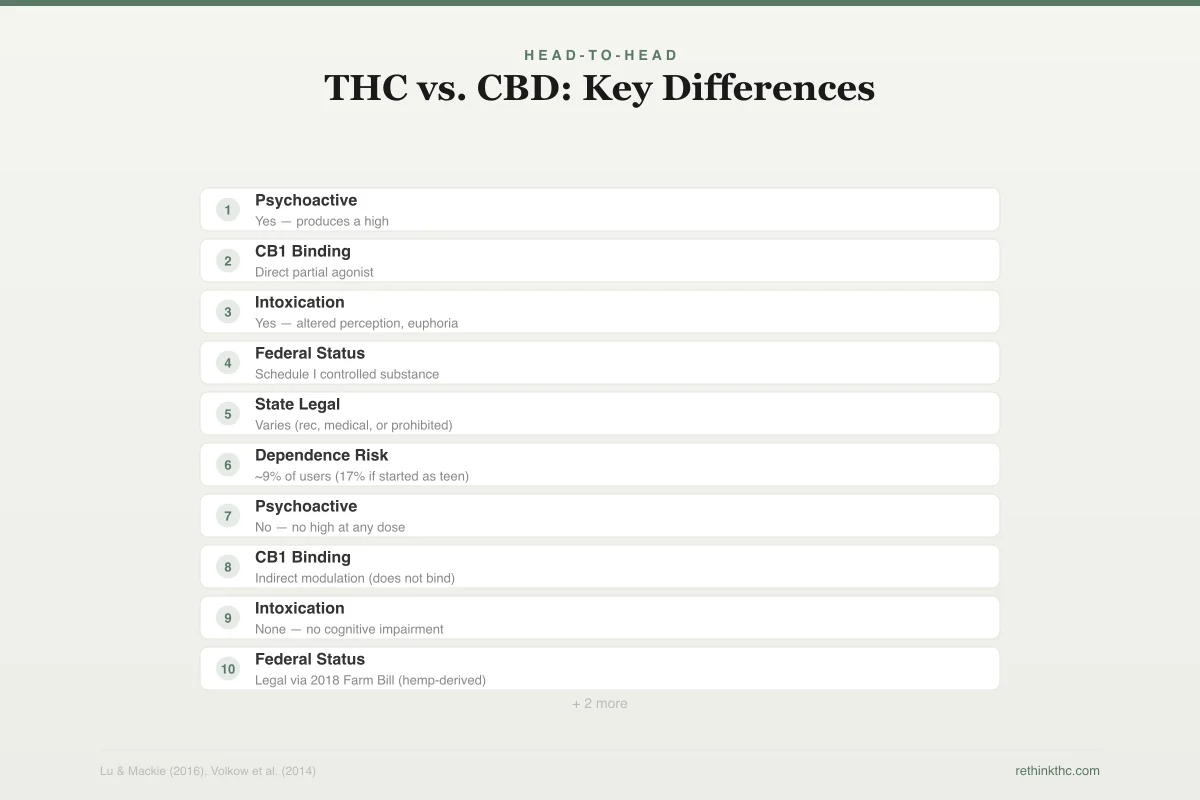
THC vs. CBD: Key Differences
Same molecular formula, fundamentally different effects
Tetrahydrocannabinol
Closed ring structure
Psychoactive
Yes — produces a high
CB1 Binding
Direct partial agonist
Intoxication
Yes — altered perception, euphoria
Federal Status
Schedule I controlled substance
State Legal
Varies (rec, medical, or prohibited)
Dependence Risk
~9% of users (17% if started as teen)
Cannabidiol
Open ring structure
Psychoactive
No — no high at any dose
CB1 Binding
Indirect modulation (does not bind)
Intoxication
None — no cognitive impairment
Federal Status
Legal via 2018 Farm Bill (hemp-derived)
State Legal
Widely available (stores, online)
Dependence Risk
No evidence of dependence
Here is what is surprising: THC and CBD have the exact same molecular formula. They are both made of 21 carbon atoms, 30 hydrogen atoms, and 2 oxygen atoms. The difference is in the arrangement. One small structural variation, a single ring in the molecule that is closed in THC and open in CBD, changes everything about how each compound interacts with your brain.
That single structural difference is the reason THC produces a high and CBD does not. It is also the reason they have different therapeutic profiles, different side effects, and different risk profiles.
| Feature | THC | CBD |
|---|---|---|
| Produces a high | Yes (CB1 receptor activation) | No |
| Pain relief | Moderate evidence (neuropathic, cancer) | Early-stage evidence |
| Anxiety effect | Increases at higher doses | May reduce (preclinical evidence) |
| Sleep effect | Sedating but suppresses REM | May reduce barriers to natural sleep |
| Tolerance | Develops within weeks | Does not appear to develop |
| Dependence risk | ~9% lifetime; up to 50% daily users | No apparent dependence risk |
| Cognitive impairment | Yes (memory, attention, coordination) | No at typical doses |
| Legal status (US federal) | Schedule I (state laws vary) | Legal if hemp-derived (<0.3% THC) |
| FDA-approved uses | Nausea (dronabinol, nabilone) | Epilepsy (Epidiolex) |
How Each Interacts With Your Brain
To understand why THC and CBD do different things, you need a basic understanding of the endocannabinoid system (ECS). This is a signaling network in your brain and body that regulates mood, pain, appetite, sleep, memory, and immune function. It was not discovered until the early 1990s, when researchers identified the first endogenous cannabinoid, anandamide, a molecule your body produces naturally that fits into the same receptors that THC targets.
Lu and Mackie published a comprehensive review of the endocannabinoid system in 2016 in Biological Psychiatry. Their review describes the two primary cannabinoid receptors: CB1 receptors, which are concentrated in the brain, and CB2 receptors, which are found primarily in immune cells and peripheral tissues. The ECS also includes endogenous cannabinoids (anandamide and 2-AG) and the enzymes that break them down. For a deeper exploration of how this system works, see the endocannabinoid system and withdrawal.
THC works by binding directly to CB1 receptors in the brain. It fits into these receptors like a key into a lock, mimicking anandamide but with much greater potency and duration. This direct binding is what produces the psychoactive effects: altered perception, euphoria, slowed time, impaired short-term memory, and increased appetite. It is also what drives tolerance and dependence, because chronic CB1 activation causes your brain to reduce the number and sensitivity of those receptors.
CBD does not bind directly to CB1 or CB2 receptors in any meaningful way. Instead, it modulates the endocannabinoid system indirectly. It appears to inhibit the enzyme (FAAH) that breaks down anandamide, effectively increasing your body's own endocannabinoid levels. It also interacts with serotonin receptors, TRPV1 pain receptors, and other signaling pathways outside the classical endocannabinoid system. This indirect mechanism is why CBD does not produce a high, does not impair cognition, and does not appear to carry the same dependence risk as THC.
Psychoactive vs. Non-Psychoactive
This is the distinction most people start with, and it is real. THC is psychoactive. CBD is not (or more precisely, CBD does not produce intoxication, though it may affect mood through other pathways).
Receptor Pharmacology
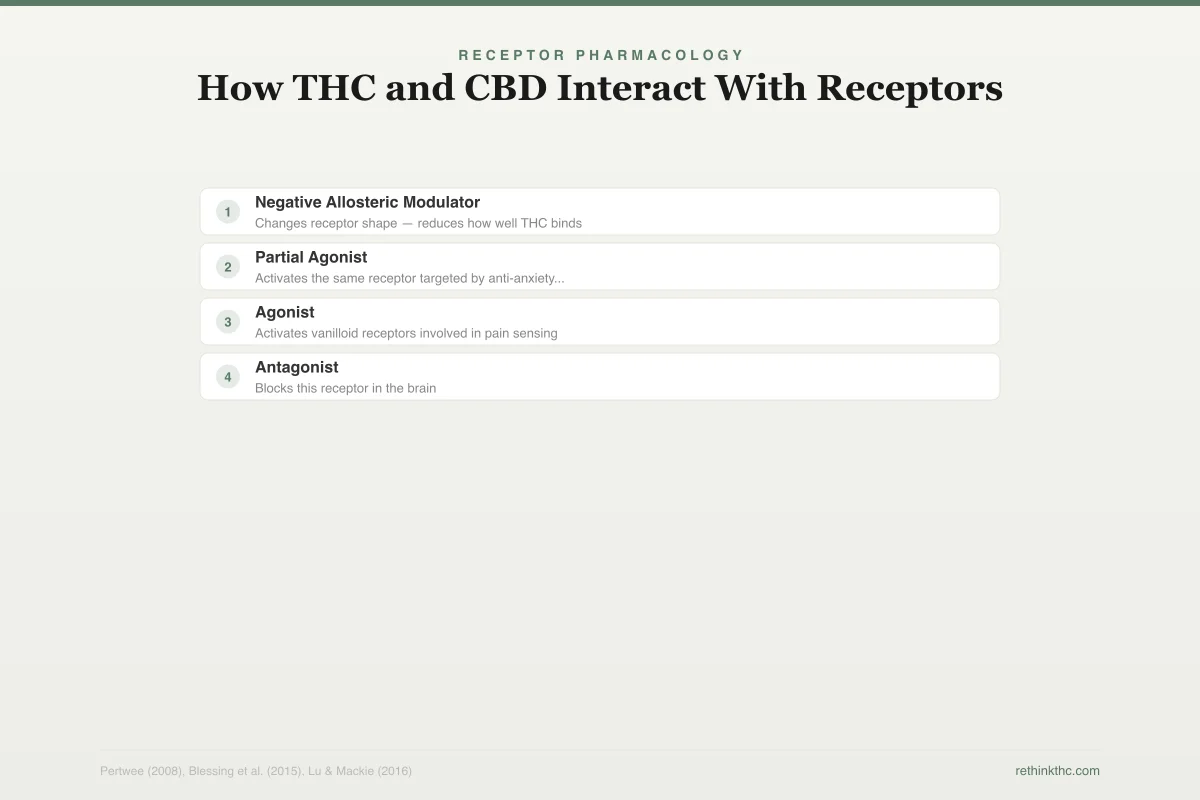
How THC and CBD Interact With Receptors
One compound, one receptor. The other works across multiple systems.
Direct Binding — Single Target
THC fits into CB1 like a key into a lock — directly activates the receptor
Psychoactive effects, pain modulation, appetite, impaired memory
Indirect Action — Multiple Targets
Changes receptor shape — reduces how well THC binds
May buffer THC's negative effects (anxiety, paranoia)
Activates the same receptor targeted by anti-anxiety medication buspirone
Anxiolytic (anti-anxiety) effects
Activates vanilloid receptors involved in pain sensing
Pain modulation, anti-inflammatory
Blocks this receptor in the brain
Seizure reduction, neuroprotection
When someone says cannabis "gets you high," they are talking about THC activating CB1 receptors in the brain. The intensity of that high depends on the dose, the delivery method, your tolerance, and your individual biology. But the mechanism is always THC binding to CB1.
CBD does not produce that experience at any dose. You can take very large amounts of CBD and you will not feel intoxicated, impaired, or euphoric. This is not a matter of degree. It is a fundamentally different pharmacological action because CBD does not activate CB1 receptors the way THC does.
This distinction matters practically. If you are using a cannabis product for potential therapeutic benefit and want to remain clear-headed, the THC content is what determines impairment. If you are concerned about dependence, THC is the compound that drives the tolerance, withdrawal, and compulsive use patterns associated with cannabis use disorder. Volkow and colleagues, in a 2014 review published in the New England Journal of Medicine, estimated that approximately 9% of cannabis users develop dependence over their lifetime, with higher rates among adolescent-onset and daily users. That dependence risk is attributed to THC, not CBD.
The Medical Evidence: Different Compounds, Different Applications
The research base for THC and CBD points in different therapeutic directions.
THC: Pain, Nausea, Spasticity
A landmark 2015 meta-analysis by Whiting and colleagues, published in JAMA, reviewed 79 randomized controlled trials involving 6,462 participants. The review found moderate-quality evidence that cannabinoids (primarily THC-based pharmaceutical products) are associated with improvement in chronic pain, chemotherapy-induced nausea and vomiting, and spasticity associated with multiple sclerosis.
Three FDA-approved medications are based on THC or synthetic THC: dronabinol and nabilone (for nausea) and nabiximols (a THC/CBD spray approved for spasticity in countries outside the US). The evidence for these applications is real, though the studies used pharmaceutical products with precise dosing, not dispensary cannabis. For a detailed review of this evidence, see the proven medical benefits of cannabis.
CBD: Anxiety, Epilepsy
The evidence for CBD points toward a different set of conditions. Blessing and colleagues published a 2015 review in Neurotherapeutics[1] examining CBD's potential for anxiety disorders. The review found substantial preclinical evidence (animal studies and early human studies) supporting CBD as a treatment for generalized anxiety disorder, panic disorder, social anxiety disorder, obsessive-compulsive disorder, and PTSD.
The preclinical evidence is genuinely promising. But "preclinical" means most of it comes from animal models and small human pilot studies. Large, long-term clinical trials in people with diagnosed anxiety disorders are still largely missing from the literature. The signal is real. The confirmation is pending.
The strongest clinical evidence for CBD comes from epilepsy. Epidiolex, a purified CBD medication, was FDA-approved in 2018 for two rare seizure disorders (Dravet syndrome and Lennox-Gastaut syndrome) based on large randomized controlled trials showing significant seizure reduction. For a deeper look at CBD and anxiety specifically, see CBD for anxiety, what the research shows.
Side Effect Profiles
THC and CBD also differ meaningfully in their side effects.
Side Effect Comparison
THC vs. CBD: Side Effect Profiles
THC carries significantly more side effects than CBD
8 known side effects
4 known side effects
No tolerance, dependence, or withdrawal documented
THC side effects include impaired short-term memory, impaired coordination, anxiety and paranoia (especially at higher doses), increased heart rate, dry mouth, and red eyes. With chronic use, THC is associated with tolerance, dependence, withdrawal symptoms, and cognitive effects that may persist after cessation (particularly in people who began using in adolescence). A 2009 review by Crippa and colleagues in Human Psychopharmacology[2] documented that anxiety and panic attacks are among the most common acute adverse reactions to cannabis, driven by THC's dose-dependent effects.
CBD side effects are generally milder. Reported side effects include fatigue, diarrhea, changes in appetite, and potential interactions with other medications (CBD inhibits certain liver enzymes involved in drug metabolism). CBD does not appear to produce tolerance, dependence, or withdrawal. It does not impair cognition or coordination at typical doses.
This difference in side effect profiles is one reason some researchers and clinicians are more interested in CBD as a therapeutic agent. The risk-benefit calculation looks different when the compound does not produce intoxication or dependence.
Legal Status
The legal landscape for THC and CBD is different, though both are complicated.
THC remains a Schedule I controlled substance at the federal level in the United States. State laws vary widely, with some states permitting recreational THC use, others allowing only medical use, and some maintaining full prohibition. The federal-state conflict creates an unstable legal environment.
CBD derived from hemp (cannabis plants containing less than 0.3% THC) was federally legalized by the 2018 Farm Bill. This is why you can buy CBD products in grocery stores, gas stations, and online retailers in most states. However, the FDA has not approved CBD as a dietary supplement or food additive, creating regulatory gray areas. And CBD derived from marijuana (cannabis plants above 0.3% THC) remains federally controlled regardless of the CBD content.
The Potency Shift: Why the Ratio Matters
Perhaps the most practically important difference between THC and CBD in 2026 is not the pharmacology. It is the market reality.
Ratio Spectrum
THC:CBD Ratio Guide
The ratio between THC and CBD may matter more than the amount of either alone
Anti-inflammatory, anti-anxiety, no psychoactivity
Best for: Anxiety, inflammation, daily function
Calming, slight body relaxation
Best for: Anxiety with mild pain, stress
Therapeutic, manageable psychoactivity
Best for: General pain, MS spasticity (Sativex ratio)
Pain relief, appetite, nausea reduction
Best for: Neuropathic pain, chemo nausea
Maximum psychoactive, strong pain relief
Best for: Most dispensary products (unintentionally)
ElSohly and colleagues published a landmark analysis in 2016 in Biological Psychiatry[3] documenting that the average THC content in seized cannabis samples roughly tripled between 1995 and 2014, rising from about 4% to about 12%. At the same time, CBD content decreased. The THC-to-CBD ratio shifted dramatically, from roughly 14:1 in 1995 to roughly 80:1 by 2014.
This is a fundamental change in what cannabis is. A plant that once delivered moderate THC alongside meaningful CBD now delivers high THC with negligible CBD. Concentrates and vape cartridges have pushed this even further, with THC levels often exceeding 80% and CBD content near zero.
Why does this matter? Because there is growing evidence that CBD may buffer some of THC's negative effects, particularly anxiety and cognitive impairment. When cannabis contained a more balanced ratio of THC to CBD, the experience may have been different from what most people encounter today. Modern cannabis is, in many practical ways, a different substance than what existed a generation ago.
This ratio shift is relevant to the question of whether cannabis "helps" or "hurts" anxiety. The answer may partly depend on which era of cannabis you are talking about. A product with 5% THC and 5% CBD might produce a very different anxiety response than one with 25% THC and 0.1% CBD. For more on how cannabis relates to anxiety, see does weed help anxiety.
The Entourage Effect: Theory vs. Evidence
You may have heard of the entourage effect, the idea that cannabinoids work better together than in isolation. The theory suggests that THC, CBD, and other cannabinoids (plus terpenes and flavonoids in the plant) interact synergistically, with each compound modulating the effects of the others.
This is a reasonable hypothesis. CBD does appear to modulate some of THC's effects in controlled settings. And whole-plant extracts sometimes behave differently than isolated compounds in preclinical research.
But the entourage effect remains more theory than established science. Large clinical trials directly comparing whole-plant cannabis to isolated cannabinoids for the same condition are rare. The concept is often invoked by the cannabis industry to market whole-plant products as inherently superior to isolates, but the evidence does not yet support that broad claim. If you are shopping for CBD products, understanding the difference between full-spectrum, broad-spectrum, and isolate formulations helps you evaluate what you are actually buying. It is a promising research direction, not a settled conclusion.
What This Means Practically
If you are a current cannabis user, the THC-vs-CBD distinction affects you directly.
If you are using cannabis and experiencing anxiety, paranoia, or cognitive fog, those effects are driven by THC. A CBD-dominant product would not produce those experiences. Knowing which compound is responsible for which effect helps you make more informed choices about what you use, how much, and why.
If you are considering cannabis for a medical condition, the evidence base is different for each compound. THC has the stronger evidence for pain and nausea. CBD has the more promising (though less proven) evidence for anxiety and certain seizure disorders. Using a high-THC product for anxiety is pharmacologically counterproductive at most doses.
If you are trying to quit or cut back, understanding that dependence is driven by THC, not CBD, helps clarify what you are actually dealing with. Withdrawal symptoms, tolerance escalation, and compulsive use patterns are all features of chronic THC exposure.
When to Seek Professional Help
If you are using cannabis (THC or CBD) for a medical condition, a healthcare provider knowledgeable about cannabinoid medicine can help you evaluate the evidence for your specific situation and monitor for side effects or dependence.
If you are finding it difficult to control your cannabis use, using more than you intend, or experiencing withdrawal symptoms when you stop, those are signs of cannabis use disorder. This is a recognized medical condition with effective treatments.
The SAMHSA National Helpline is available 24/7 at 1-800-662-4357. It is free, confidential, and provides referrals to local treatment facilities, support groups, and community-based organizations.
The Bottom Line
THC and CBD share the same molecular formula but differ in one structural detail that changes everything about how they interact with your brain. THC binds directly to CB1 receptors, producing psychoactive effects, tolerance, and dependence. CBD modulates the endocannabinoid system indirectly without producing a high or carrying dependence risk. A 2015 JAMA review found moderate evidence for THC in chronic pain and nausea, while a separate 2015 review found promising preclinical evidence for CBD in anxiety disorders. Average THC potency in cannabis tripled between 1995 and 2014 while CBD content dropped, shifting the THC-to-CBD ratio from roughly 14:1 to 80:1. This means modern cannabis is a fundamentally different product than what existed a generation ago, with implications for both therapeutic potential and side effects.
Sources & References
- 1RTHC-00924·Blessing, Esther M. et al. (2015). “CBD and Anxiety in 2015: Promising Signals, Mostly From Single Doses.” Neurotherapeutics.Study breakdown →PubMed →↩
- 2RTHC-00349·Crippa, Jose Alexandre S. et al. (2009). “Cannabis both calms and panics — the biphasic dose-response explains why the same drug produces opposite anxiety effects.” Human Psychopharmacology: Clinical and Experimental.Study breakdown →PubMed →↩
- 3RTHC-01144·ElSohly, Mahmoud A. et al. (2016). “U.S. Cannabis Potency Tripled Over Two Decades While CBD Nearly Vanished.” Biological Psychiatry.Study breakdown →PubMed →↩