How to Sleep Without Weed: 12 Methods That Actually Work
Withdrawal & Recovery
0.5 mg
Low-dose melatonin at 0.5 to 1 mg works better than the 5 to 10 mg sold in stores, and withdrawal insomnia resolves within 2 to 4 weeks for most people.
Babson et al., Current Psychiatry Reports, 2017
Babson et al., Current Psychiatry Reports, 2017
View as imageIf you only read one thing
You will sleep normally again — most people do within 2 to 4 weeks. Right now, the three things that help most are: set a non-negotiable wake time (same time every day, even after terrible nights), get out of bed after 20 minutes if you're not sleeping, and take 0.5 to 1 mg of melatonin before bed — not the 5 to 10 mg sold in stores, which is way too much. If insomnia lasts past 4 weeks, CBT-I (a type of therapy for insomnia) beats every sleep medication for long-term results.
It is 3 AM. You have been staring at the ceiling for two hours. Your body is tired but your brain will not shut off. You used to smoke before bed and fall asleep in minutes. Now you are lying here wondering if you will ever sleep normally again without it.
You will. But right now, you need something more useful than "practice good sleep hygiene." You need specific techniques that address what is actually happening in your brain during cannabis withdrawal.
When you used cannabis regularly, THC replaced your brain's natural sleep-initiation process. It suppressed your arousal system and shortened the time it took to fall asleep, a dynamic explored in detail in our guide on cannabis and sleep. Now that the THC is gone, your brain has to relearn how to do that on its own. The result is a temporary period where falling asleep feels nearly impossible, staying asleep is a struggle, and what sleep you do get feels shallow and unrefreshing.
This is not permanent. Clinical research has found that sleep disruption from cannabis withdrawal typically resolves within 45 days, with most people seeing significant improvement by weeks 2 to 4. A comprehensive review by Babson and colleagues in Current Psychiatry Reports confirmed that sleep disturbance is the most persistent withdrawal symptom but follows a predictable recovery curve.[1] A systematic review of 39 human studies further documented that while cannabis is commonly used as a sleep aid, withdrawal consistently disrupts sleep architecture.[2]
Here are 12 methods that actually help. Not all of them will work for you, but several of them will.
Key Takeaways
- Withdrawal insomnia is temporary and follows a predictable timeline — most people sleep normally within 2 to 4 weeks, and nearly everyone does by day 45
- Your wake time matters more than your bedtime when it comes to resetting your circadian rhythm after quitting
- Low-dose melatonin (0.5 to 1 mg) actually works better than the 5 to 10 mg doses sold in most stores
- CBT-I (cognitive behavioral therapy for insomnia) beats sleep medication for long-term results
- Watch out for common traps like using alcohol as a sleep aid, taking long naps, and staying in bed awake for hours
- Sleep is usually the last withdrawal symptom to go away, but it is also one of the most fully reversible — no lasting impairment has been documented after quitting
Methods at a Glance
| Method | Category | Best For | When to Use |
|---|---|---|---|
| Non-negotiable wake time | Circadian | Everyone; foundational habit | Start day 1 |
| 20-minute rule | Behavioral (CBT-I) | Lying awake unable to sleep | Nightly, as needed |
| Room temperature | Environmental | Night sweats; overheating | Every night |
| Screen cutoff | Environmental | Difficulty initiating sleep | 30–60 min before bed |
| Exercise | Physical | General sleep quality; anxiety | Morning or early afternoon |
| Magnesium glycinate | Supplement | Muscle tension; restlessness | 30–60 min before bed |
| Progressive muscle relaxation | Relaxation | Physical tension; racing body | In bed, lights off |
| 4-7-8 breathing | Relaxation | Anxiety-driven wakefulness | In bed, lights off |
| Brain dump journaling | Cognitive | Racing thoughts; worry loops | 5–10 min before bed |
| Caffeine cutoff | Behavioral | Afternoon/evening caffeine users | Before noon daily |
| Low-dose melatonin | Supplement | Circadian rhythm disruption | Short-term bridge (2–4 weeks) |
| CBT-I | Structured therapy | Persistent insomnia beyond 4 weeks | Gold standard treatment |
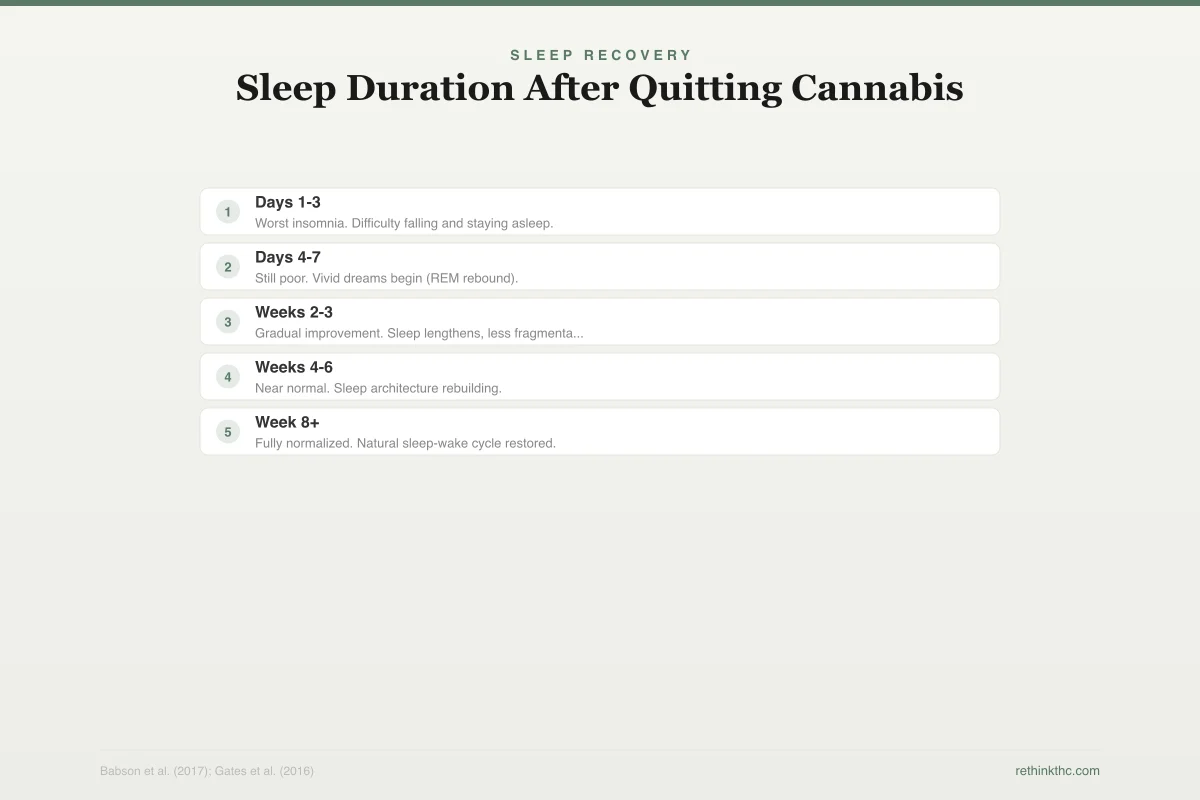
The timeline below shows when sleep typically recovers during withdrawal, so you can see where you are in the process and what improvement to expect next.
Sleep Recovery
Sleep Duration After Quitting Cannabis
Most people sleep normally within 2-4 weeks. Nearly everyone by day 45.
Worst insomnia. Difficulty falling and staying asleep.
Still poor. Vivid dreams begin (REM rebound).
Gradual improvement. Sleep lengthens, less fragmentation.
Near normal. Sleep architecture rebuilding.
Fully normalized. Natural sleep-wake cycle restored.
1. Set a Non-Negotiable Wake Time
This is the single most important thing you can do, and it is also the hardest. Pick a wake time and get out of bed at that time every single day, even if you slept terribly. Even if you did not sleep at all. Even on weekends.
Your circadian rhythm, the internal clock that governs your sleep-wake cycle, anchors itself primarily to when you wake up, not when you go to bed. Sleeping in after a bad night feels like recovery, but it actually shifts your circadian rhythm later and makes the next night worse. Research from the American Psychological Association's sleep guidelines confirms that a consistent wake time is the foundation of every evidence-based insomnia treatment.
Set an alarm. Put your phone across the room so you have to stand up to turn it off. Then stay up. Your body will eventually start getting sleepy at an appropriate time in the evening, but only if you give it a consistent anchor point in the morning.
2. The 20-Minute Rule
If you have been lying in bed for about 20 minutes and you are not asleep, get up. Go to another room. Do something quiet and boring in dim light: read a physical book, listen to a calm podcast, fold laundry. When you feel sleepy again, go back to bed. Repeat as many times as necessary.
This is not a random suggestion. It is the core principle of stimulus control therapy, one of the primary components of CBT-I (cognitive behavioral therapy for insomnia). A 2022 study found that CBT-I not only improved sleep and reduced depression scores in cannabis users, but 80 percent of participants also reduced their cannabis use at three months.[3] The logic is straightforward: if you lie in bed awake and frustrated night after night, your brain starts associating your bed with wakefulness and stress instead of sleep. Breaking that association is critical, especially during withdrawal when your anxiety system is already running hot.
The goal is simple. Bed equals sleep. If bed does not equal sleep right now, remove yourself from the equation until it does.
3. Drop Your Room Temperature
Your core body temperature needs to drop by about 2 to 3 degrees Fahrenheit for sleep to initiate. This is a fundamental biological requirement, not a preference. When your body cannot cool down, your brain cannot transition into the first stage of sleep. Here is how the key environmental and behavioral techniques work together.
Evidence-Based Sleep Strategies
Top 6 Techniques Ranked by Evidence
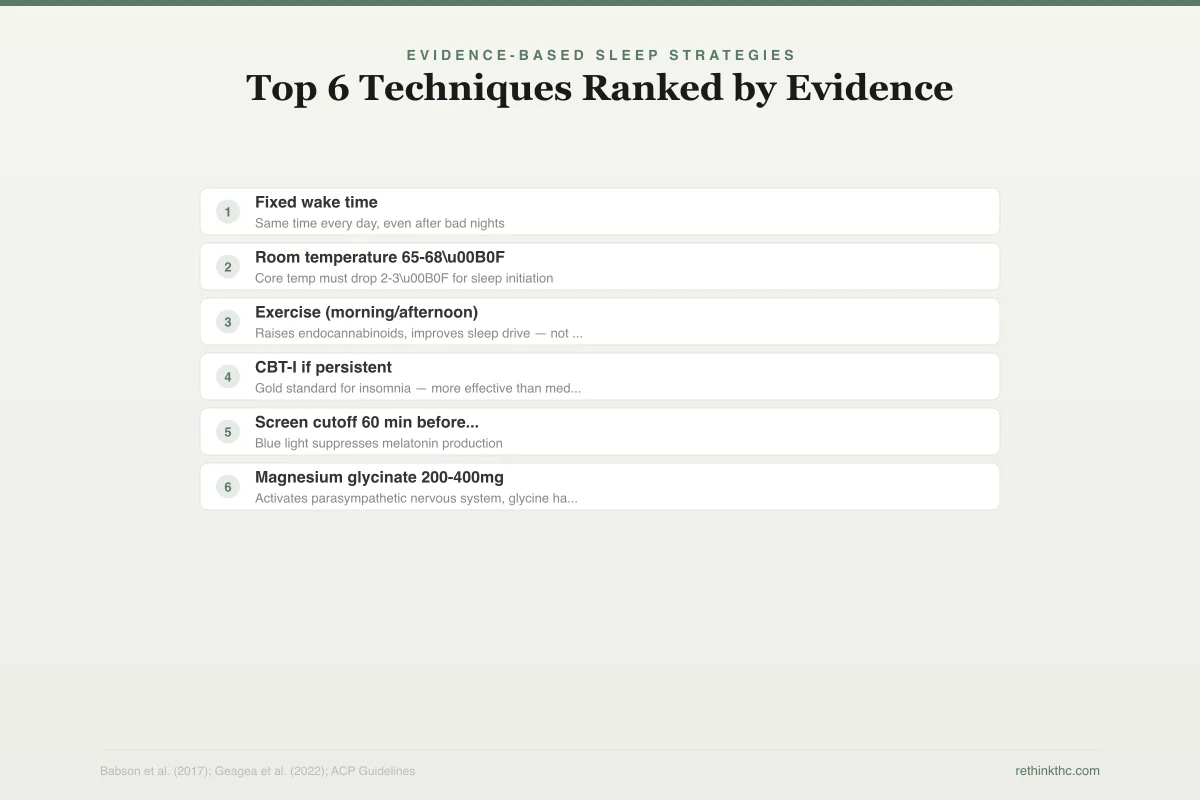
Not all sleep advice is equal. These are ranked by research support for withdrawal insomnia.
Fixed wake time
StrongSame time every day, even after bad nights
Room temperature 65-68°F
StrongCore temp must drop 2-3°F for sleep initiation
Exercise (morning/afternoon)
StrongRaises endocannabinoids, improves sleep drive — not within 3hrs of bed
CBT-I if persistent
StrongGold standard for insomnia — more effective than medication long-term
Screen cutoff 60 min before bed
ModerateBlue light suppresses melatonin production
Magnesium glycinate 200-400mg
ModerateActivates parasympathetic nervous system, glycine has calming properties
Set your bedroom to 65 to 68 degrees Fahrenheit. If you do not have air conditioning, use a fan pointed at your upper body. During cannabis withdrawal, night sweats are common because your autonomic nervous system is recalibrating.[4] A cooler room counteracts this directly.
Here is a useful trick: take a warm shower 60 to 90 minutes before bed. This sounds counterintuitive, but the warm water brings blood to the surface of your skin. When you step out, that blood rapidly cools, dropping your core temperature faster than it would drop naturally. Sleep researchers call this the "warm bath effect," and a 2019 meta-analysis in Sleep Medicine Reviews found it consistently improved both sleep onset and sleep quality.
4. Cut Screens 30 to 60 Minutes Before Bed
Your phone, laptop, and TV emit blue-spectrum light that directly suppresses melatonin production. Melatonin is the hormone your brain releases to signal that it is time to sleep. Blue light tells your brain it is still daytime.
During withdrawal, this matters more than usual. Your melatonin system is already disrupted because THC was partially handling the sleep-initiation job that melatonin is supposed to do. Adding blue light on top of a system that is already struggling to produce adequate melatonin at the right time makes falling asleep significantly harder.
If cutting screens entirely feels impossible, use night mode on your devices and dim the brightness as low as it goes. But the physical act of putting the phone in another room removes the temptation to scroll, which is what actually keeps most people awake.
5. Exercise, but Get the Timing Right
Regular exercise is one of the most consistently supported interventions for improving sleep quality. A 2015 meta-analysis in the Journal of Behavioral Medicine found that people who exercised regularly fell asleep faster, slept longer, and rated their sleep quality higher than non-exercisers.
But timing matters, especially during withdrawal. Exercise raises your core body temperature and cortisol (a stress hormone) for several hours afterward. Both need to come back down before sleep can happen. Morning or early afternoon exercise gives your body time to cool down and for cortisol to return to baseline. High-intensity exercise within 3 hours of bedtime can delay sleep onset and make an already difficult night worse.
If you can only exercise in the evening, keep it light. A walk works. Save the intense sessions for earlier in the day.
6. Magnesium Glycinate
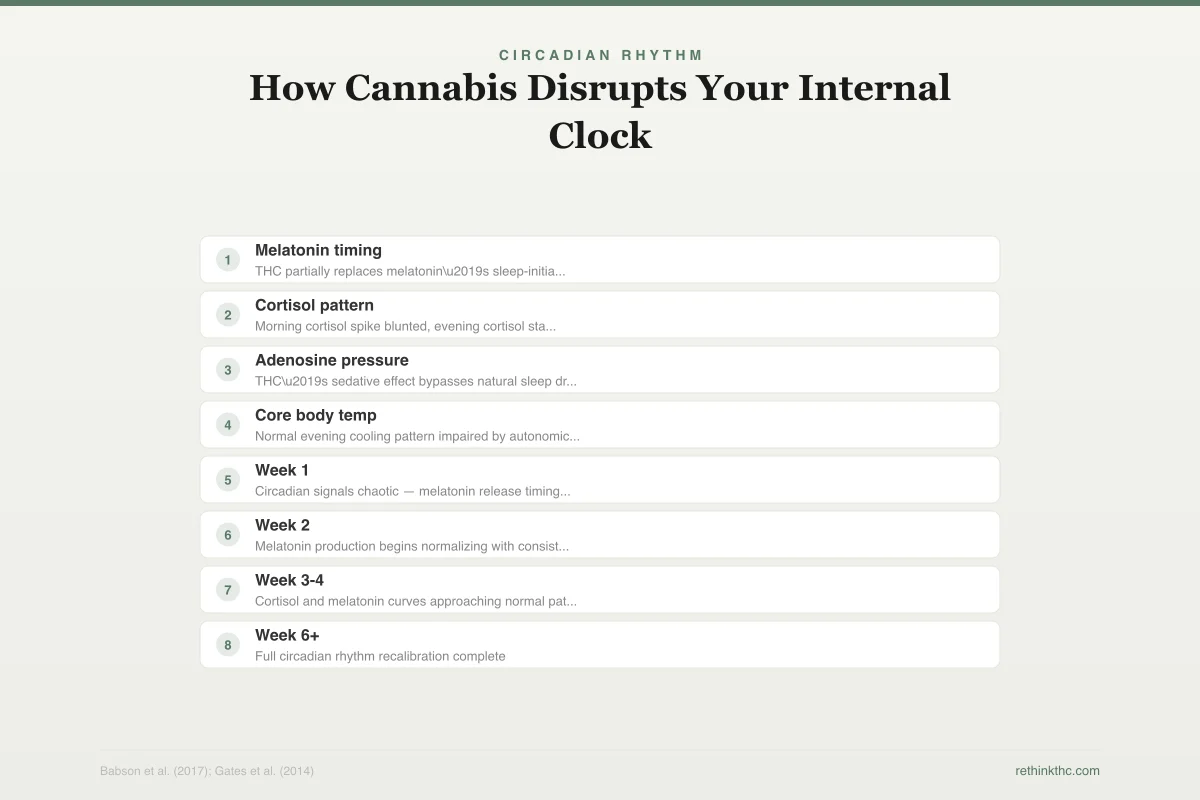
Magnesium plays a role in activating the parasympathetic nervous system, the branch of your nervous system responsible for the "rest and digest" state. Magnesium glycinate specifically is the form best absorbed for sleep purposes, and the glycine component itself has calming properties. The diagram below shows how cannabis withdrawal disrupts your circadian rhythm and where supplements fit into the recovery process.
Circadian Rhythm
How Cannabis Disrupts Your Internal Clock
Your circadian system recalibrates over 2-4 weeks after quitting.
During regular use
THC partially replaces melatonin’s sleep-initiation role
Morning cortisol spike blunted, evening cortisol stays elevated
THC’s sedative effect bypasses natural sleep drive buildup
Normal evening cooling pattern impaired by autonomic changes
Recovery timeline
Circadian signals chaotic — melatonin release timing off, cortisol irregular
Melatonin production begins normalizing with consistent wake times
Cortisol and melatonin curves approaching normal pattern
Full circadian rhythm recalibration complete
A 2012 study in the Journal of Research in Medical Sciences found that magnesium supplementation improved subjective measures of insomnia in elderly adults. The evidence is not overwhelming, but it is promising, the mechanism is plausible, and the risk profile is very low. A typical dose is 200 to 400 mg taken 30 to 60 minutes before bed.
This is not a sleeping pill. It is a mineral that many people are mildly deficient in, and correcting that deficiency can remove one barrier to sleep. Think of it as giving your nervous system a nutrient it may be missing, not as sedation.
7. Progressive Muscle Relaxation
Your body stores tension in ways you do not notice until you actively release it. Progressive muscle relaxation (PMR) is a technique that systematically works through every major muscle group, tensing and then releasing each one.
Here is how to do it. Lie in bed with the lights off. Start with your feet. Curl your toes tightly for 5 seconds, then release completely for 15 seconds. Notice the difference between tension and relaxation. Move to your calves. Tense for 5 seconds, release for 15. Continue up through your thighs, glutes, abdomen, hands, arms, shoulders, neck, and face.
PMR activates your parasympathetic nervous system, shifting your body out of the fight-or-flight state that withdrawal often triggers. It also gives your brain something structured to focus on instead of the loop of "I cannot sleep, why am I not sleeping, I need to sleep." A full cycle takes about 10 to 15 minutes.
8. 4-7-8 Breathing
Inhale through your nose for 4 seconds. Hold for 7 seconds. Exhale slowly through your mouth for 8 seconds. Repeat four times.
The extended exhale is the key. Long exhalation activates your vagus nerve, the primary nerve of the parasympathetic nervous system. Vagus nerve activation slows your heart rate, lowers blood pressure, and signals your brain to shift out of alertness mode. During withdrawal, your sympathetic nervous system (the fight-or-flight branch) tends to run hotter than normal. This breathing pattern directly counteracts that.
You will probably feel slightly lightheaded the first few times. That is normal and passes quickly. Do it lying in bed with the lights off. If four cycles do not make you sleepy, do four more.
9. Brain Dump Journaling Before Bed
If racing thoughts are the main thing keeping you awake, get them out of your head and onto paper. Not a formal journal entry. A brain dump. Spend 5 to 10 minutes before bed writing down everything that is on your mind: worries, tasks, unresolved conversations, random thoughts. No structure needed.
Before we move on to caffeine and melatonin, here is how the evidence stacks up for the most common sleep supplements people reach for during withdrawal.
Supplement Evidence
Supplements for Withdrawal Insomnia
Ranked by evidence strength. None are magic bullets — use alongside sleep hygiene.
Activates parasympathetic system. Low risk. Many people are mildly deficient.
Timing signal, not a sedative. Most store doses (5-10 mg) are too high.
Found in tea. May reduce anxiety that interferes with sleep.
Mixed results in clinical trials. May take 2+ weeks to show effect.
Some evidence for anxiety-related insomnia. Optimal dose not established.
Very low risk. Ritual of warm beverage may matter as much as the compound.
None of these replace good sleep hygiene. A consistent wake time + cool dark room will outperform any supplement alone.
A 2018 study published in the Journal of Experimental Psychology found that participants who wrote a to-do list before bed fell asleep significantly faster than those who wrote about completed tasks. The act of externalizing future concerns reduced the cognitive arousal that was keeping them awake.
Keep a notebook and pen on your nightstand. When the thoughts start spinning, write them down. You are not solving anything. You are telling your brain that these items have been captured and do not need to be held in active memory right now.
10. Cut Caffeine After Noon
Caffeine has a half-life of 5 to 6 hours. That means if you drink a cup of coffee at 3 PM, half of that caffeine is still active in your brain at 9 PM. A quarter of it is still there at 3 AM.
During withdrawal, this matters more than it did when you were using cannabis. THC has mild sedative properties that partially offset caffeine's stimulant effects. Without that counterbalance, caffeine hits harder and lasts longer in terms of its impact on your ability to fall asleep. Many people who had no problem drinking afternoon coffee while using cannabis find that the same habit now costs them hours of sleep.
The noon cutoff is a starting point. If your sleep is severely disrupted, try moving it to 10 AM or cutting caffeine entirely for a few weeks. You can reintroduce it once your sleep stabilizes.
11. Low-Dose Melatonin, Short Term
Most melatonin supplements sold in stores are dramatically overdosed. Bottles commonly contain 5 to 10 mg per serving, but research suggests the effective dose for sleep onset is 0.5 to 1 mg. Higher doses can actually disrupt your sleep architecture and leave you groggy the next morning.
Melatonin is not a sedative. It is a timing signal. It tells your brain that nighttime has arrived and it is time to prepare for sleep. Taking it 30 to 60 minutes before your target bedtime at a low dose mimics your brain's natural melatonin release pattern. Taking a massive dose three hours before bed does not help more. It just overwhelms the system.
The evidence for melatonin is moderate. The American Academy of Sleep Medicine notes that it has limited support for chronic insomnia but can be helpful for circadian rhythm disruption, which is exactly what happens during cannabis withdrawal. Use it for a few weeks as a bridge while your brain's natural melatonin production comes back online. It is not a long-term solution.
12. CBT-I: The Gold Standard
Cognitive behavioral therapy for insomnia (CBT-I) is the single most effective treatment for insomnia, period. It is more effective than sleeping pills for long-term outcomes, and it does not carry any dependency risk. The American College of Physicians recommends it as the first-line treatment for chronic insomnia in adults, ahead of any medication.
CBT-I combines several of the techniques in this article (stimulus control, sleep restriction, cognitive restructuring) into a structured program, typically delivered over 4 to 8 sessions. It works by breaking the mental and behavioral patterns that perpetuate insomnia after the original trigger (in your case, withdrawal) has passed.
You do not necessarily need a therapist to access it. The VA developed a free app called CBT-i Coach, and Insomnia Coach is another free option. Both walk you through the core CBT-I protocol. If your insomnia is severe or you have a co-occurring condition like anxiety or depression, working with a trained CBT-I provider is more effective than self-guided programs.
What Not to Do
Some of the most common responses to withdrawal insomnia make it worse.
Alcohol. Alcohol is a sedative, so it does help you fall asleep faster. But it fragments your sleep architecture, suppresses REM sleep (the same thing THC was doing), and causes rebound wakefulness in the second half of the night. You are trading one sleep-disrupting substance for another.[5]
Benadryl (diphenhydramine) long-term. Antihistamines cause drowsiness, but they reduce sleep quality, impair next-day cognitive function, and lose their effectiveness within days as tolerance builds. They are not designed for ongoing use as a sleep aid.
Staying in bed for hours awake. This feels productive ("at least I am resting") but it trains your brain to associate bed with wakefulness. Get up after 20 minutes. Every minute you spend lying awake in bed makes the next night harder.
Napping excessively. A short nap (20 minutes or less) before 2 PM is fine. Anything longer or later in the day reduces your sleep drive, the biological pressure that builds throughout the day and makes you sleepy at night. During withdrawal, you need every ounce of sleep drive you can accumulate.
This Is Temporary
Withdrawal insomnia feels permanent when you are in it. It is not. The research is consistent: sleep quality improves steadily after the first week, with most people sleeping normally within 2 to 4 weeks.[6] Even heavy, long-term users typically see full sleep recovery by day 45. Your brain built a sleep system that worked before cannabis, and it is rebuilding that system now. The withdrawal timeline is predictable even when the experience feels chaotic.
If you want to understand why your dreams are so intense during this period, that is a separate but related process called REM rebound. And if you are dealing with withdrawal insomnia alongside other symptoms, know that sleep is typically the last symptom to resolve and the first to test your commitment to staying quit.
You slept before weed. You will sleep after it. Right now, your job is to give your brain every possible advantage while it figures out how to do this on its own again.
Safety
ModerateSleep deprivation compounds every other symptom
Concern
Severe, prolonged insomnia during withdrawal can worsen anxiety, depression, irritability, and cognitive function. Sleep deprivation also increases relapse risk because exhaustion makes everything harder to cope with.
What the research says
Most withdrawal insomnia resolves by weeks 2-4, with nearly everyone sleeping normally by day 45. If insomnia persists beyond 6 weeks or you cannot function at work or in daily life, that's beyond typical withdrawal and warrants professional evaluation.
Particularly relevant for: Anyone experiencing severe sleep disruption beyond the first month of quitting
What to do
If you're past week 6 and still not sleeping, or if insomnia is accompanied by severe anxiety, depression, or thoughts of self-harm, see a healthcare provider. CBT-I with a trained clinician is the most effective next step. SAMHSA: 1-800-662-4357.
Babson et al. (2017), Current Psychiatry Reports
When to Seek Professional Help
If insomnia persists beyond 6 weeks, if you are unable to function at work or in daily life due to sleep deprivation, or if you are experiencing severe anxiety, depression, or thoughts of self-harm alongside the insomnia, talk to a healthcare provider. Sleep deprivation compounds every other withdrawal symptom and can become a standalone problem if it is not addressed.
A doctor can evaluate whether CBT-I, short-term sleep medication, or treatment for a co-occurring condition is appropriate. You do not have to do this alone, and asking for help with sleep is not a failure. It is a practical decision.
If you need immediate support, SAMHSA's National Helpline is available 24/7 at 1-800-662-4357. It is free, confidential, and available in English and Spanish.
The Bottom Line
Cannabis withdrawal insomnia is the most persistent quit symptom, but it follows a predictable timeline: worst during week one, steadily improving through weeks two to four, and resolving for nearly everyone by day 45. The most effective single intervention is setting a non-negotiable wake time to anchor your circadian rhythm. CBT-I (cognitive behavioral therapy for insomnia) outperforms sleep medication for long-term results, and several of its core techniques — stimulus control, sleep restriction, and cognitive restructuring — can be applied immediately without a therapist. Low-dose melatonin (0.5 to 1 mg) works as a short-term timing signal while your brain's natural production recovers. Avoid alcohol, antihistamines, and excessive napping, all of which worsen sleep architecture during withdrawal.
Sources & References
- 1RTHC-01329·Babson, Kimberly A et al. (2017). “Why Quitting Cannabis Wrecks Your Sleep — and Why It Gets Better.” Current psychiatry reports.Study breakdown →PubMed →↩
- 2RTHC-00797·Gates, Peter J. et al. (2014). “39 Studies Later, the Evidence That Cannabis Helps You Sleep Is Weaker Than You Think.” Sleep Medicine Reviews.Study breakdown →PubMed →↩
- 3RTHC-03863·Geagea, Luna et al. (2022). “Cognitive behavioral therapy for insomnia improved sleep, mood, and reduced cannabis use.” Sleep medicine.Study breakdown →PubMed →↩
- 4RTHC-00820·Lee, Dayong et al. (2014). “Cannabis withdrawal symptoms peaked in days 0-3 but sleep problems got worse over time.” The American journal on addictions.Study breakdown →PubMed →↩
- 5RTHC-00788·Conroy, Deirdre A et al. (2014). “Sleep problems and substance use disorders fuel each other in both directions.” Current psychiatry reports.Study breakdown →PubMed →↩
- 6RTHC-01161·Gates, Peter et al. (2016). “Systematic Review Confirms Cannabis Withdrawal Disrupts Sleep, but Specific Mechanisms Remain Unclear.” Substance abuse.Study breakdown →PubMed →↩