Cannabis and Sleep: Does It Actually Help or Just Mask the Problem?
Balanced Cannabis Science
Worse Sleep
THC reduces the time it takes to fall asleep, but chronic use suppresses REM sleep and degrades overall sleep quality, and heavy users actually sleep worse by objective measures even when they believe cannabis is helping.
Bolla et al., Sleep, 2008
Bolla et al., Sleep, 2008
View as imageIf you only read one thing
Cannabis helps you fall asleep faster — that part is real. But it wrecks the quality of the sleep you actually get, especially the REM stage your brain needs for memory and emotional health. Within a few weeks of nightly use, tolerance kicks in and you need more for less benefit. When you try to stop, withdrawal creates the exact insomnia you were trying to fix. It feels like it works because falling asleep fast is the only part you can notice — the damage to your sleep architecture happens while you are unconscious.
Sleep is the most commonly cited reason people give for using cannabis, alongside pain. The logic seems straightforward: you smoke, you get drowsy, you fall asleep faster. And for many people, that experience is real and immediate. The problem is that the relationship between cannabis and sleep is far more complex than "it helps me fall asleep, so it helps me sleep."
The research tells a story with two distinct chapters. In the short term, THC does reduce the time it takes to fall asleep. In the long term, it degrades the quality of the sleep you get, builds tolerance that eliminates the initial benefit, and creates a withdrawal pattern that makes sleep significantly worse when you try to stop. Understanding both chapters is essential for making an honest assessment of whether cannabis is actually helping your sleep or just creating the illusion of help while making the underlying problem worse.
Key Takeaways
- THC helps you fall asleep faster (reduces sleep latency), but regular use disrupts sleep quality by suppressing REM sleep and reducing deep sleep
- CBD appears to affect sleep differently and may be beneficial without the tolerance, dependence, or sleep disruption that comes with THC
- Tolerance to THC's sleep-promoting effects builds within weeks, so the same dose stops working and people end up using more to get the same result
- When regular users quit, REM rebound produces vivid, often disturbing dreams and insomnia that can last 2 to 6 weeks or longer
- Falling asleep faster is not the same as sleeping well — and cannabis tends to help with the first at the expense of the second
- CBT-I (cognitive behavioral therapy for insomnia) is the gold standard for chronic insomnia and consistently beats medications in long-term studies without any dependence risk
What THC Does to Sleep Stages
To understand how cannabis affects sleep, you need a basic understanding of what healthy sleep looks like. Sleep is not a uniform state. It cycles through distinct stages, each serving different biological functions. The visual below shows how a healthy night cycles through these stages — and where THC disrupts the pattern.
Sleep Architecture
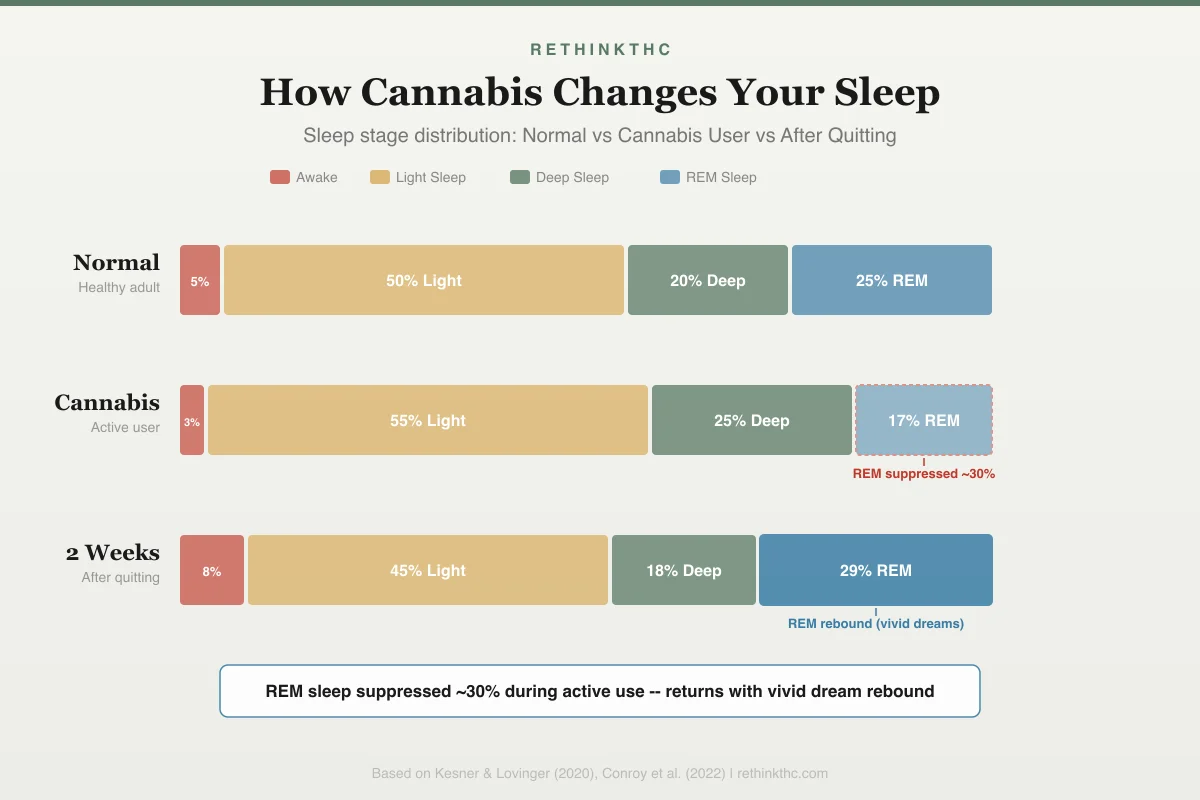
How Cannabis Changes Your Sleep
Sleep stage distribution across three conditions
REM sleep suppressed ~30% during active use -- returns with vivid dream rebound after quitting
Light sleep (Stages 1 and 2) is the transition into deeper sleep. Slow-wave sleep (Stage 3, also called deep sleep) is when your body does most of its physical repair, immune system maintenance, and growth hormone release. REM sleep (rapid eye movement) is when most dreaming occurs and is critical for emotional processing, memory consolidation, and learning.
A healthy night of sleep cycles through these stages multiple times, with more deep sleep in the first half of the night and more REM sleep in the second half. Disrupting this architecture, even if total sleep time stays the same, degrades sleep quality in ways that affect mood, cognition, and physical health.
Babson and colleagues published a comprehensive review of cannabis and sleep in 2017 in Current Psychiatry Reports.[1] The review examined the existing literature on how cannabis affects sleep and found a consistent pattern: THC decreases sleep latency (helps you fall asleep faster) when used acutely, but impairs long-term sleep quality with chronic use.
Specifically, THC suppresses REM sleep.[1] This is why many cannabis users report that they "do not dream" or rarely remember dreams. They are not failing to dream. Their REM sleep is being shortened and fragmented, reducing the amount of time spent in the stage where most vivid dreaming occurs. This REM suppression is one of the most consistently documented effects of THC on sleep architecture.
THC also affects deep sleep, though the findings are more variable.[1] Some studies show a mild increase in slow-wave sleep acutely (which may contribute to the feeling of "good sleep"), while chronic use appears to reduce deep sleep over time. For a detailed breakdown of how each sleep stage is affected, including the dose-response relationship and how different products alter the pattern, see cannabis and sleep architecture.
| Sleep Metric | Acute THC Effect | Chronic THC Effect | After Quitting |
|---|---|---|---|
| Sleep latency | Decreased (fall asleep faster) | Tolerance develops; latency returns to baseline | Increased (insomnia peaks days 2-5) |
| REM sleep | Suppressed | Chronically suppressed | REM rebound (vivid/disturbing dreams) |
| Deep sleep | Mildly increased (some studies) | Reduced over time | Gradually normalizes over weeks 2-4 |
| Sleep efficiency | Slightly improved | Worse than non-users | Worst in week 1, improves by week 4 |
| Subjective quality | "Slept great" | "Need it to sleep" | "Cannot sleep at all" then gradual recovery |
Why It Feels Like It Works (When the Data Says It Does Not)
This is the paradox at the center of the cannabis-and-sleep question, and understanding it changes how you evaluate your own experience.
Bolla and colleagues published a study in 2008 in Sleep that examined sleep quality in heavy cannabis users using polysomnography — objective lab measurement.[2] Heavy cannabis users showed lower total sleep time, less slow-wave sleep, worse sleep efficiency (the ratio of time asleep to time in bed), and longer sleep onset latency compared to controls. The people using cannabis the most were sleeping the worst by every objective measure, even though many of them believed cannabis was helping their sleep.
This disconnect between what you experience and what is actually happening has a straightforward explanation. Sleep latency is the only sleep metric you can consciously evaluate. You know how long it took to fall asleep. That experience is available to your awareness. You cannot evaluate REM duration, deep sleep quality, sleep efficiency, or architecture from inside the experience. Those metrics are invisible to the sleeper.
THC improves the one metric you notice — how fast you fall asleep — while degrading the metrics you cannot notice: REM time, deep sleep proportion, and overall architecture. When you wake up and think "I slept great," what you actually mean is "I fell asleep fast and do not remember waking up." Both of those things can be true while the restorative value of the sleep you got was objectively poor.
A 2025 meta-analysis by Mao and colleagues examined 102 observational studies and found that current recreational cannabis use was associated with poorer sleep quality, more insomnia symptoms, and a later chronotype compared to non-use, with stronger associations in men and younger users.[8] Interestingly, 19 experimental studies found no associations between cannabis use and sleep quality or duration — suggesting that controlled lab conditions may eliminate the real-world variables (stress, routine disruption, anxiety) that self-medicating users are also addressing when they use cannabis for sleep.
The comparison to alcohol is instructive. Both substances reduce sleep latency. Both degrade sleep architecture. Both build tolerance. Both create a withdrawal rebound that makes the problem worse. The mechanism differs — GABA for alcohol, CB1 for cannabis — but the trap is structurally identical. You feel like it helps because you fall asleep fast. The data shows it does not help because the sleep you get is worse.
This is why user testimonials about cannabis and sleep are unreliable. Not because people are lying, but because the metric they are evaluating (how fast they fell asleep) is not the metric that determines whether sleep is actually restorative. You cannot rate sleep quality from within the experience. You can only rate sleep onset.
Feeling like you slept is not the same as having slept well. Cannabis can improve the former while degrading the latter.
CBD, Dose, and the Strain Question
CBD and THC are often discussed together, but their effects on sleep are meaningfully different, and the emerging nuances matter for anyone trying to make informed choices.
The Babson 2017 review noted that CBD may have therapeutic potential for insomnia without the sleep architecture disruption caused by THC.[1] CBD does not suppress REM sleep. It does not produce the sedative "knockout" effect that THC does. Instead, preliminary evidence suggests it may reduce anxiety and promote calmness in a way that facilitates natural sleep onset.
This distinction matters because the mechanism is different. THC essentially forces sedation by acting on CB1 receptors in brain regions involved in wakefulness and sleep regulation. CBD appears to reduce barriers to sleep — primarily anxiety and hyperarousal — without directly suppressing sleep stages. The result is that CBD-assisted sleep may more closely resemble natural sleep architecture. CBD is not a sedative. It is an anxiety reducer that happens to help sleep when anxiety is the barrier.
The Dose Question
The sleep architecture effects of THC are dose-dependent in ways that matter practically. At very low doses (under 5 milligrams), THC may reduce sleep latency with minimal architecture disruption. At typical recreational doses — 15 milligrams or more, which is where most flower and most edibles land — REM suppression is consistent. The therapeutic window for sleep is narrow, and most people overshoot it without knowing it.
This creates a problem that dose escalation makes worse, not better. As tolerance builds, people increase the dose to regain the sleep-onset benefit, which pushes them further into the range where architecture disruption is most pronounced. You end up using more of the thing that is making your sleep worse in order to preserve the one benefit — faster onset — that tolerance is eroding anyway.
The Indica Question
The popular belief that "indica equals sleep" is genetically unreliable. Indica and sativa are botanical classification categories that poorly predict chemical composition. What drives the sedating quality of a given strain is its chemical profile — primarily terpenes like myrcene and linalool — not whether it was classified as indica or sativa. Terpene content varies batch to batch, grower to grower, and is rarely tested or labeled with any precision at dispensaries.
This means the strain that "put you to sleep" last month may have a different terpene profile than the same strain name from a different grower. Relying on strain names for consistent sleep effects is unreliable in a way that pharmaceutical sleep products are not — and this inconsistency is another reason cannabis makes a poor long-term sleep strategy.
However, the evidence for CBD and sleep is still in its early stages. The Babson review noted that while the preclinical evidence is promising, large-scale clinical trials are limited. And most commercially available cannabis products are THC-dominant, meaning people who are using "cannabis for sleep" are primarily using THC, not CBD. For a deeper analysis of the evidence, dosing considerations, and who CBD for sleep works best for, see CBD for sleep.
How Consumption Method Affects Sleep
Not all cannabis use affects sleep equally. The method of consumption changes the pharmacokinetics — how THC reaches the brain, how long it stays active, and how much of the night it influences.
Inhalation (smoking and vaping) produces rapid onset and relatively short duration. THC blood levels peak within 10 to 30 minutes and decline substantially over 2 to 3 hours.[5] This means sleep architecture in the first half of the night is most affected, while the second half — where most REM sleep normally concentrates — may be partially spared if THC levels have dropped sufficiently by then.
Edibles follow a fundamentally different path. THC is metabolized by the liver into 11-hydroxy-THC, which crosses the blood-brain barrier more efficiently and has a longer half-life. Peak effects occur 2 to 3 hours after ingestion, and elevated metabolite levels can persist for 6 to 8 hours.[5] The result is that sleep architecture disruption extends across the entire night rather than primarily affecting the first half. Edibles also carry the highest risk of overconsumption due to the delayed and variable onset, which can produce overwhelming experiences including severe anxiety — the opposite of sleep promotion. For detailed guidance on dosing, timing, and managing the onset problem, see edibles for sleep.
CBD-to-THC ratio products are increasingly available and may offer a better balance for sleep. Early evidence and clinical observation suggest that products with higher CBD:THC ratios provide some relaxation with potentially less REM suppression and lower anxiety risk than THC-dominant products. The CBD component may partially counteract THC's sleep architecture disruption while preserving the calming effect.
The method choice is not trivial — it shapes not just the sleep experience on any given night but the tolerance trajectory, the severity of eventual withdrawal, and the degree of circadian disruption over time.
Cannabis and Your Circadian Rhythm
Beyond sleep stages, cannabis disrupts something more fundamental: when your body wants to sleep and wake. The endocannabinoid system is directly involved in circadian rhythm regulation. Preclinical research has identified CB1 receptors in the suprachiasmatic nucleus (SCN), the brain's master clock, and endocannabinoid levels naturally fluctuate across the 24-hour cycle as part of the timing signal.
The chart below illustrates the core tradeoff: faster sleep onset versus degraded sleep quality over time.
The Sleep Paradox
Falling Asleep Faster vs. Sleeping Well
Cannabis improves one metric at the expense of the other
Sleep Latency
Time to fall asleep
Falls asleep 15-30 minutes faster on average
Sleep Quality
Deep sleep + REM time
REM suppressed ~30%, deep sleep reduced with chronic use
Feeling like you slept is not the same as sleeping well -- cannabis optimizes falling asleep while undermining the restorative stages your body needs
Daily cannabis use overrides these natural fluctuations with constant exogenous THC, degrading the circadian signal. Early evidence suggests THC may also suppress melatonin secretion, weakening the hormonal cue that tells your brain nighttime has arrived. Some researchers have observed that morning cannabis use may blunt the cortisol awakening response — the natural cortisol surge that calibrates daytime alertness and anchors the entire circadian cycle.
The observable result is delayed sleep phase. Clinicians report that chronic cannabis users tend to develop a delayed sleep phase, drifting toward later bedtimes and a late-morning or midday wake time. When professional or social obligations require earlier schedules, the result is chronic sleep debt — not from inability to sleep, but from a biological clock that is out of sync with the external schedule. This circadian misalignment has downstream effects on metabolism, mood regulation, immune function, and cognitive performance that extend well beyond subjective tiredness.
Importantly, stopping cannabis does not automatically reset the circadian clock. Active re-entrainment through consistent wake time, timed light exposure, and regular meal timing is required, typically over 2 to 4 weeks. The full mechanism and recovery protocol are covered in weed and circadian rhythm.
The Tolerance Problem
Even if you accept that THC helps you fall asleep in the short term, there is a structural problem that undermines it as a long-term sleep solution: tolerance.
Your brain adapts to regular THC exposure by reducing the number and sensitivity of CB1 receptors. Hirvonen and colleagues demonstrated this in a 2012 study published in Molecular Psychiatry using brain imaging.[3] The study showed that CB1 receptor density was significantly reduced in chronic cannabis users compared to controls, with the degree of reduction correlating with years of use.
This receptor downregulation is the biological basis of tolerance. When CB1 receptors are less available and less sensitive, the same dose of THC produces less effect. For sleep specifically, this means the dose that reliably knocked you out in month one may barely make you drowsy by month four.
The typical response is dose escalation. You use a bit more. Then a bit more. Eventually, you may find that even large doses produce only marginal sleep benefit while the side effects (next-day grogginess, cognitive impairment, dependence) continue to increase. This is a losing trajectory that worsens over time rather than improving.
What Happens When You Stop: REM Rebound and Insomnia
A 2016 systematic review by Gates and colleagues examined 36 human studies on cannabis withdrawal and sleep.[4] The review confirmed that sleep disruption is a consistent feature of cannabis withdrawal and one of the primary drivers of relapse. People who quit cannabis for other reasons often resume use specifically because they cannot sleep.
The dream component is called REM rebound. After weeks or months of REM suppression from THC, your brain compensates when THC is removed by producing an excess of REM sleep. Dreams become more frequent, more vivid, more emotionally intense, and often more disturbing. For some people, the nightmares after quitting weed are so vivid and distressing that they wake repeatedly through the night, which worsens the insomnia.
This REM rebound is covered in detail in THC and REM sleep rebound, and the broader insomnia pattern is addressed in weed withdrawal insomnia.
The Sleep Recovery Timeline
The withdrawal insomnia follows a predictable pattern, and knowing the timeline prevents the most common mistake: quitting on day 4 because you conclude cannabis was medically necessary for sleep.
Days 1 to 3. Sleep onset delay returns. You lie awake longer than you have in months. The first signs of REM rebound appear. Many people mistake this for the insomnia they were "treating" with cannabis, when it is actually withdrawal from it.[6]
Days 2 to 5. The worst insomnia. Near-total sleeplessness for some. This is the relapse danger zone. The logic feels airtight: "I cannot sleep without cannabis, therefore I need cannabis to sleep." But this is the bottom of the withdrawal curve, not the new normal. Approximately 47 percent of regular users experience clinically significant withdrawal symptoms during this window.[7]
Weeks 1 to 2. REM rebound in full force. Vivid, emotionally intense, sometimes disturbing dreams every night. Night sweats after quitting weed compound the disruption — caused by thermoregulatory dysfunction as the endocannabinoid system recalibrates.[9] The combination of insomnia, vivid nightmares, and drenched sheets makes this the hardest stretch.
Weeks 2 to 3. Dream intensity drops. Total sleep time gradually increases. Still not great, but the trajectory is clearly improving. Most people can feel the difference between this week and week one.
Week 4. CB1 receptor density normalizes.[3] Sleep architecture begins returning to baseline. The biological foundation for natural sleep regulation is back online.
Weeks 4 to 6. Most people report that sleep has normalized or, for some, improved beyond their pre-cannabis baseline. The full sleep recovery timeline after quitting weed maps this progression week by week. The vivid dreams during withdrawal may persist for several weeks beyond that, gradually fading.
The key insight: the worst night is usually night 3 or 4. That is the exact night most people decide to use again. The timeline shows that night 4 is the bottom, not the new normal. Everything after it gets better. For a comprehensive guide to managing this entire process, see the complete cannabis withdrawal guide.
Safety
ModerateWithdrawal insomnia drives relapse
Concern
About 47% of regular cannabis users experience clinically significant withdrawal symptoms. Sleep disruption is among the most distressing and is one of the strongest predictors of relapse — people quit on day 3 or 4 believing they cannot sleep without cannabis, when they are actually at the worst point of withdrawal.
What the research says
The insomnia peaks around days 2 to 5, then steadily improves. CB1 receptors normalize by about week 4 of abstinence. Most people report normal or even improved sleep by weeks 4 to 6. The worst night is the bottom of the curve, not the new normal.
Particularly relevant for: Anyone who uses cannabis nightly and is considering stopping or reducing
What to do
If you are planning to quit, expect 3 to 5 rough nights and do not make the decision to restart during that window. Taper gradually if possible. Consider CBT-I or a short-term sleep aid to bridge the gap. Talk to a healthcare provider if withdrawal insomnia lasts beyond 6 weeks.
Bahji et al. (2020), JAMA Network Open; Gates et al. (2016), Substance Abuse; Hirvonen et al. (2012), Molecular Psychiatry
The Difference Between Falling Asleep and Sleeping Well
This distinction is the core of the cannabis and sleep question, and it is worth stating explicitly.
Falling asleep is about sleep latency, the time between getting into bed and losing consciousness. THC reliably reduces this number, at least initially. If your primary problem is lying in bed for hours unable to drift off, THC addresses that specific symptom.
Sleeping well is about sleep architecture, the progression through light sleep, deep sleep, and REM sleep in appropriate proportions. It is about sleep efficiency, total sleep time, overnight awakenings, and how you feel the next day. By these measures, chronic THC use is consistently associated with worse outcomes.
Cannabis optimizes one metric (falling asleep) at the expense of the others. This is why many daily users report that they "sleep fine" but also feel chronically tired, mentally foggy, and emotionally flat. The sleep they are getting looks like sleep from the outside, but it is not delivering the restorative benefits that healthy sleep architecture provides.
Medical Use vs. Self-Medication for Sleep
There is an important distinction between using cannabis for sleep under medical guidance and self-medicating with whatever is available at the dispensary.
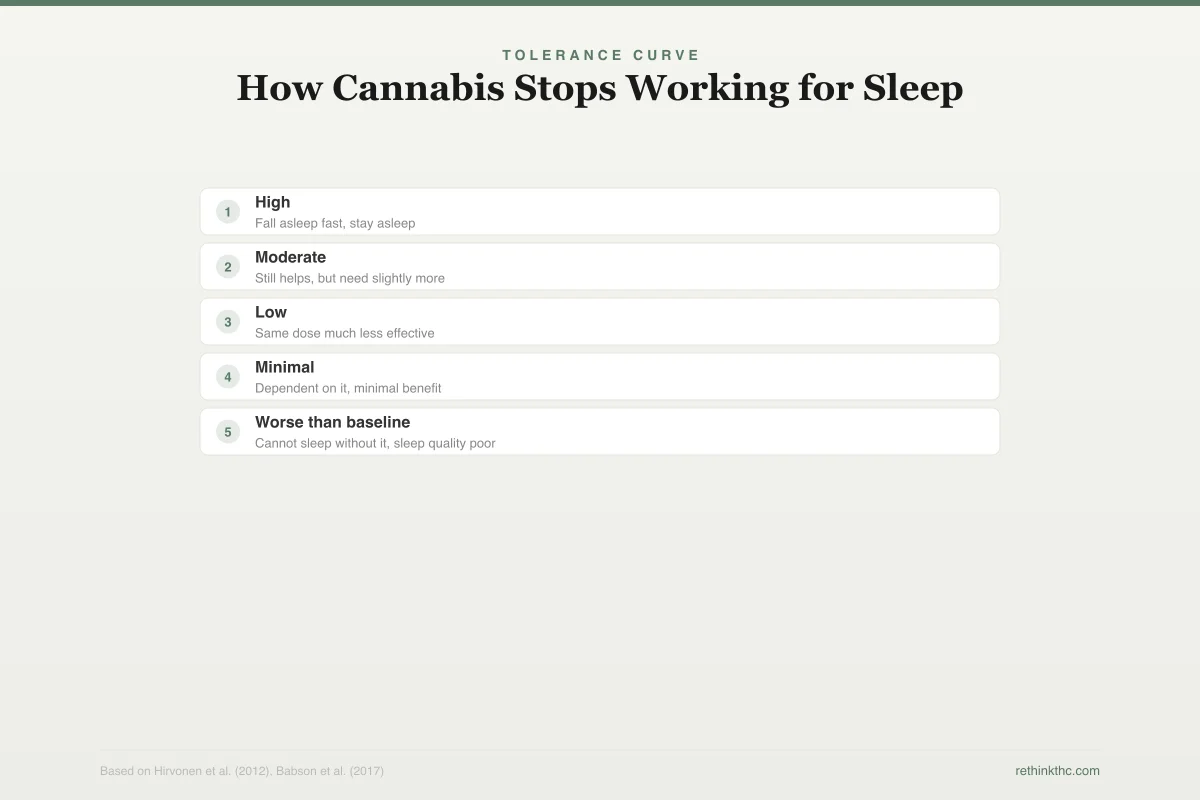
The chart below shows how tolerance erodes the initial sleep benefit, often within weeks of regular use.
Tolerance Curve
How Cannabis Stops Working for Sleep
CB1 receptor downregulation erodes effectiveness over time
Fall asleep fast, stay asleep
Still helps, but need slightly more
Same dose much less effective
Dependent on it, minimal benefit
Cannot sleep without it, sleep quality poor
As CB1 receptors downregulate, you need more cannabis for less effect -- eventually sleep is worse than before you started, but you cannot sleep without it
Medical cannabis programs in some jurisdictions include insomnia or sleep disorders as qualifying conditions. When cannabis is prescribed for sleep by a knowledgeable provider, it typically involves specific product recommendations, dosing guidance, monitoring for tolerance and side effects, and integration with other sleep interventions (sleep hygiene, cognitive behavioral therapy for insomnia, and management of underlying conditions).
Self-medication, which describes how most people use cannabis for sleep, involves no dosing guidance, no monitoring, no attention to product composition, and no plan for managing tolerance. The person decides they sleep better with cannabis, buys whatever is available, and uses it nightly in increasing amounts. This pattern almost always leads to tolerance, dependence, and worse sleep outcomes over time.
Neither approach is guaranteed to work. But the difference between medical oversight and unguided self-medication is the difference between a strategy and a habit. For a broader perspective on what the research supports across all medical cannabis applications, see medical benefits of cannabis.
What the Research Cannot Tell You (Yet)
The Babson 2017 review was careful to note the limitations of the existing evidence. Most cannabis and sleep studies are small. Many rely on self-reported sleep quality rather than objective polysomnography. The products used in studies often do not match what consumers are actually using. And long-term studies (following users for years rather than weeks) are rare.
The review also noted a significant gap in research on the sleep effects of different cannabinoid ratios, terpene profiles, and consumption methods. It is plausible that a low-dose, CBD-dominant product taken sublingually has very different sleep effects than a high-THC concentrate that is smoked. But the research to confirm or deny this is largely absent.
What the science can say with reasonable confidence is that acute THC use reduces sleep latency, chronic THC use disrupts sleep architecture, tolerance erodes the benefit over weeks, and withdrawal produces rebound insomnia and vivid dreams. Beyond that, the field needs better data.
Practical Considerations
If you are currently using cannabis for sleep and are evaluating your options, here are some evidence-informed considerations.
If cannabis is the only thing that gets you to sleep, consider that the underlying reason may have shifted. You may have started using cannabis because of difficulty sleeping, but after months of daily use, the difficulty sleeping when you try to stop may be withdrawal-driven rather than reflecting your original sleep problem. The only way to find out is to go through the withdrawal period, which typically peaks in week 1 and substantially improves by weeks 3 to 4. Strategies for navigating this period are covered in how to sleep without weed.
If tolerance is building, that is a signal that the approach is not sustainable. Needing more cannabis to achieve the same sleep effect is the definition of tolerance, and the trajectory points toward increasing dose, increasing dependence, and decreasing actual sleep quality. If nightly use has become your default, the research on using weed to sleep every night long-term outlines exactly where that trajectory leads.
If you want to try reducing rather than stopping, a gradual taper is generally easier to tolerate than abrupt cessation. Reducing by roughly 10 to 25% per week allows some adaptation and produces milder withdrawal symptoms. Switching to CBD-only products during the taper may preserve some sleep benefit without the REM suppression and tolerance issues associated with THC. Some people also find that melatonin during weed withdrawal can bridge the gap while their natural sleep regulation recovers.
Cognitive behavioral therapy for insomnia (CBT-I) is the gold standard treatment for chronic insomnia and has consistently outperformed medications in long-term studies. It addresses the behavioral and cognitive patterns that maintain insomnia without any substance at all. If you have never tried CBT-I, it should be on your list before or alongside any substance-based approach.
Sleep hygiene tailored for cannabis users goes beyond the standard advice. Because THC may suppress melatonin, disrupts thermoregulation, and alters adenosine signaling, cannabis users need adapted strategies — including a 2 to 3 hour pre-bed cannabis cutoff, specific temperature management, and building non-cannabis wind-down routines. Standard recommendations like consistent wake time, dark and cool bedroom, no screens for 30 to 60 minutes before bed, and limiting caffeine after noon represent the foundation. But sleep hygiene for cannabis users covers the specific adaptations that account for THC's interference with these systems. Building this foundation before attempting to quit dramatically reduces withdrawal insomnia severity.
Cannabis versus other sleep aids. If you are considering alternatives to cannabis for sleep, understanding the tradeoffs is essential. Melatonin is not a sedative but a circadian clock shifter — useful for timing problems but not for hyperarousal-based insomnia. Diphenhydramine (Benadryl) builds tolerance faster than cannabis and carries long-term dementia risk. Trazodone has a more favorable profile for chronic use. Magnesium is the lowest-risk option but also the mildest. The detailed comparison is covered in cannabis vs sleep aids.
Undiagnosed sleep apnea may be hiding behind your cannabis use. Cannabis-induced sedation can mask the symptoms of obstructive sleep apnea by reducing the arousals that would otherwise alert you to breathing problems. If you snore loudly, experience morning headaches, or feel excessively sleepy despite adequate sleep hours, a sleep study should be on your list. See weed and sleep apnea for the full analysis of how cannabis interacts with sleep-disordered breathing.
The Honest Answer
Does cannabis help sleep? It helps you fall asleep faster, at least for a while. But it does not help you sleep well. It suppresses REM sleep, it may reduce deep sleep over time, it builds tolerance, and it creates a withdrawal pattern that makes sleep worse when you try to stop.
For someone with an occasional sleepless night, using cannabis once or twice is unlikely to cause significant harm. For someone using cannabis nightly as their primary sleep strategy, the evidence suggests that short-term relief is being purchased at the cost of long-term sleep quality, and the price increases over time as tolerance grows and dependence sets in.
The most honest framing is that cannabis masks sleep problems rather than solving them. It creates the experience of falling asleep while undermining the quality of the sleep that follows. If your goal is genuinely better sleep rather than faster sleep onset, the research points away from chronic cannabis use and toward approaches that improve sleep architecture rather than bypassing it.
When to Seek Professional Help
If you are experiencing chronic insomnia, whether related to cannabis use or not, professional help is available and effective. Sleep medicine specialists can assess for underlying sleep disorders (such as sleep apnea) that cannabis use may be masking. Cognitive behavioral therapy for insomnia is highly effective and produces durable improvements without medication.
If you are struggling with cannabis dependence, withdrawal insomnia, or sleep problems that are significantly affecting your daily functioning, reach out for support. SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
The Bottom Line
Cannabis helps you fall asleep faster. That part is real, and it is probably why so many people swear by it as a sleep aid. But falling asleep faster is not the same as sleeping well. THC suppresses REM sleep, the stage your brain needs for memory, emotional processing, and restoration. Over weeks of regular use, tolerance builds and you need more for less benefit while the underlying disruption continues. When you stop, withdrawal often produces the very insomnia you were trying to avoid, along with vivid dreams that can last two to six weeks before your sleep normalizes. If you are using cannabis for sleep, the honest question is whether you are solving a problem or postponing it. CBT-I, the gold standard treatment for chronic insomnia, works without tolerance or dependence, and the improvements last after treatment ends. Cannabis does not offer that.
Sources & References
- 1RTHC-01329·Babson, Kimberly A et al. (2017). “Why Quitting Cannabis Wrecks Your Sleep — and Why It Gets Better.” Current psychiatry reports.Study breakdown →PubMed →↩
- 2RTHC-00301·Bolla, Karen I. et al. (2008). “Stopping Heavy Cannabis Use Was Linked to Poorer Sleep. The Second Night Looked Worse..” Sleep.Study breakdown →PubMed →↩
- 3RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩
- 4RTHC-01161·Gates, Peter et al. (2016). “Systematic Review Confirms Cannabis Withdrawal Disrupts Sleep, but Specific Mechanisms Remain Unclear.” Substance abuse.Study breakdown →PubMed →↩
- 5RTHC-00138·Grotenhermen, Franjo (2003). “The Complete Guide to How Cannabis Moves Through Your Body.” Clinical pharmacokinetics.Study breakdown →PubMed →↩
- 6RTHC-00134·Budney, Alan J. et al. (2003). “When Heavy Users Quit Cannabis, Symptoms Show Up Fast and Ease Within Two Weeks.” Journal of Abnormal Psychology.Study breakdown →PubMed →↩
- 7RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩
- 8RTHC-07046·Mao, Fangxiang et al. (2025). “Recreational Cannabis Use Was Linked to Worse Sleep Across 120 Studies.” Sleep medicine reviews.Study breakdown →PubMed →↩
- 9RTHC-01338·Bonnet, Udo et al. (2017). “Comprehensive review of cannabis withdrawal: symptoms, brain mechanisms, gender differences, and treatment options.” Substance abuse and rehabilitation.Study breakdown →PubMed →↩