Withdrawal Anxiety vs Pre-Existing Anxiety: How to Tell the Difference
Withdrawal & Recovery
Days 2-6
Cannabis withdrawal anxiety starts within 1 to 3 days and peaks between days 2 and 6, while pre-existing anxiety persists on a flat trajectory that does not follow the withdrawal timeline.
Journal of Abnormal Psychology, 2003
Journal of Abnormal Psychology, 2003
View as imageIf you only read one thing
The single best way to tell withdrawal anxiety from a pre-existing condition is the trajectory. Withdrawal anxiety peaks in the first week, then drops steadily — rate yourself 1-10 each morning and you'll see the downward trend by week 2-3. Pre-existing anxiety stays flat or barely budges. If your numbers are clearly dropping week over week, it's withdrawal and it's resolving. If they're stuck at the same level by week 4-6, something underneath needs its own treatment. There's also a third pattern — 'unmasking' — where it partially improves then plateaus, meaning withdrawal faded but an underlying condition was revealed.
You quit weed, and now the anxiety is relentless. It follows you from the moment you wake up until you finally fall asleep, if you fall asleep at all. The question that keeps circling is whether this is just withdrawal, something temporary that will fade, or whether this is the real thing, an anxiety disorder that cannabis was keeping in check. The answer changes everything about what you should do next. And right now, in the thick of it, the two feel exactly the same.
This is one of the most common and most confusing experiences people face after quitting cannabis. The reason it is so difficult to sort out is that withdrawal anxiety and pre-existing anxiety use the same brain systems, produce the same physical symptoms, and feel subjectively identical. But they have different causes, different trajectories, and very different treatment needs. Understanding how to distinguish them, even roughly, can save you months of unnecessary suffering or prevent you from dismissing a real condition that needs professional attention.
Key Takeaways
- Withdrawal anxiety and pre-existing anxiety feel identical in the moment — which is why timing and trajectory are the most reliable ways to tell them apart
- Cannabis withdrawal anxiety usually starts within 1 to 3 days of quitting, peaks around days 2 to 6, and gets significantly better by weeks 3 to 4
- Pre-existing anxiety was there before you started using cannabis, does not follow the withdrawal timeline, and often shows recognizable patterns like social anxiety, panic disorder, or generalized worry
- Cannabis may have been suppressing an anxiety disorder for years, so quitting can "unmask" what was always there underneath
- This distinction matters because withdrawal anxiety goes away on its own while a pre-existing anxiety disorder needs targeted treatment
- Tracking your anxiety daily on a simple 1-to-10 scale gives you the data to tell a downward withdrawal trend from a persistent baseline condition
Why They Feel the Same
Both withdrawal anxiety and pre-existing anxiety disorders involve the same neurochemical machinery. Your amygdala (the brain's threat detection center) is overactive. Your GABA system (the brain's primary calming mechanism) is underperforming. Your cortisol, the main stress hormone, is running higher than it should.
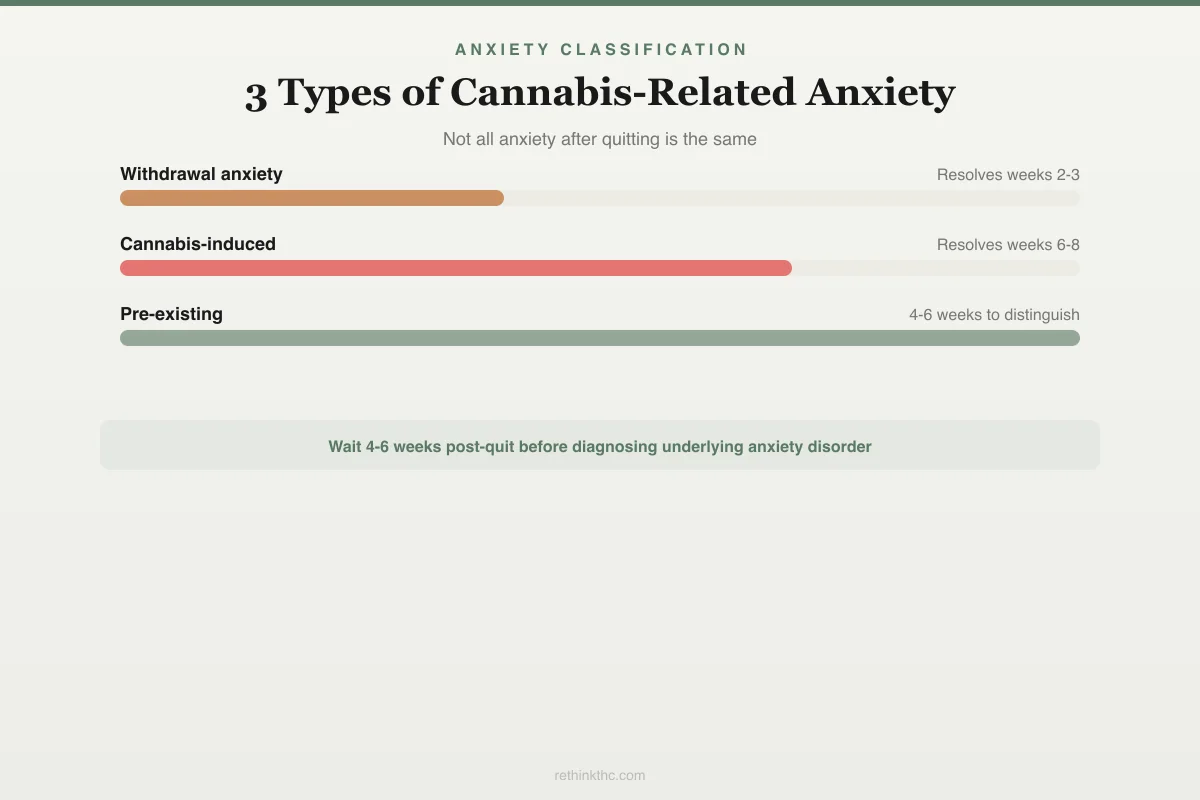
Anxiety Classification
3 Types of Cannabis-Related Anxiety
Not all anxiety after quitting is the same. Knowing which type you have determines the right response.
Onset
Day 1
Peak
Days 3-10
Resolves
Weeks 2-3
Directly caused by THC cessation. Resolves as CB1 receptors recover.
Onset
Gradual over months
Peak
Persists beyond acute
Resolves
Weeks 6-8
Developed from chronic use. Outlasts withdrawal — needs more time.
Onset
Before cannabis use
Peak
Returns when quit
Resolves
4-6 weeks to distinguish
Was masked during use. Requires 4-6 weeks post-quit to properly diagnose.
A 2009 review by Crippa and colleagues, published in Human Psychopharmacology, confirmed that cannabis modulates the very same anxiety circuits that malfunction in anxiety disorders.[1] THC dampens amygdala reactivity, boosts GABA activity, and blunts the stress response. When you remove THC after chronic use, those systems rebound. When you have an anxiety disorder, those systems are dysfunctional at baseline. The subjective experience, racing heart, dread, chest tightness, catastrophic thinking, is indistinguishable in the moment.
This is not a failure of self-awareness. It is a genuine diagnostic challenge that even clinicians find difficult to resolve without the benefit of time.
Withdrawal Anxiety: The Characteristics
Withdrawal anxiety has a specific signature. It arrives within a predictable window, follows a predictable arc, and comes packaged with other withdrawal symptoms that have nothing to do with anxiety disorders.
Research by Budney and colleagues, published in the Journal of Abnormal Psychology in 2003, documented the withdrawal time course in detail.[2] Symptoms typically begin within 1 to 3 days of the last use and peak between days 2 and 6. A 2020 meta-analysis by Bahji and colleagues, published in JAMA Network Open, found that roughly 47% of people who use cannabis regularly experience clinically significant withdrawal symptoms when they stop.[3] Anxiety is among the most commonly reported.
Here is what withdrawal anxiety typically looks like.
It appears shortly after quitting. If you were not particularly anxious during your last period of daily use and the anxiety arrived within days of stopping, the timing points toward withdrawal. Anxiety disorders do not suddenly develop because you stopped smoking. They were either there before or they were not.
It peaks and then gradually improves. Withdrawal anxiety is worst in the first one to two weeks. By weeks 3 to 4, most people report significant improvement. If you track your anxiety on a simple 1 to 10 scale each day, you should see a downward trend starting sometime in the second or third week. The improvement may not be linear, with some bad days mixed in, but the overall direction should be toward less anxiety over time.
It comes with other withdrawal symptoms. Cannabis withdrawal is not just anxiety. It includes insomnia, irritability, loss of appetite, vivid dreams, sweating, and difficulty concentrating. If you are experiencing a cluster of these symptoms alongside anxiety, that is a withdrawal pattern, not an anxiety disorder pattern. A thorough look at the full symptom picture is covered in weed withdrawal anxiety.
It responds to time, not just intervention. Withdrawal anxiety improves because your brain is recalibrating. Hirvonen and colleagues, in a 2012 study published in Molecular Psychiatry, demonstrated that CB1 receptors, the primary targets of THC in the brain, return to normal density after approximately 28 days of abstinence.[4] As your endocannabinoid system normalizes, the anxiety systems it regulates come back into balance. You do not necessarily need medication or therapy for withdrawal anxiety to resolve, though both can help you get through the acute phase.
Pre-Existing Anxiety: The Characteristics
Pre-existing anxiety looks different when you know what to examine. The key distinguishing features relate to history, pattern, and trajectory.
It was present before cannabis use began. Think back to your life before you started using cannabis regularly. Were you an anxious person? Did you avoid social situations? Did you have panic attacks? Did you worry excessively about things others seemed to handle easily? If anxiety was a significant part of your life before cannabis entered the picture, it is very likely still there underneath.
It has a specific shape. Anxiety disorders tend to present in recognizable patterns. Generalized anxiety disorder involves persistent, excessive worry about multiple areas of life. Social anxiety disorder centers on fear of judgment or embarrassment in social situations. Panic disorder involves recurring, unexpected panic attacks. Specific phobias involve intense fear of particular situations or objects. If your anxiety consistently clusters around one of these patterns, that points toward a diagnosable condition rather than generalized withdrawal distress.
It does not improve on the withdrawal timeline. This is the most important differentiator. If you are at week 5 or 6 after quitting and your anxiety has not improved at all, or has only marginally decreased, the withdrawal phase has largely passed. What remains is more likely to be an underlying condition. The complete guide to cannabis withdrawal covers the full timeline in detail.
There is often a family history. Anxiety disorders have a strong genetic component. If close family members have struggled with anxiety, panic attacks, or related conditions, the probability that your anxiety is more than withdrawal increases.
The Unmasking Phenomenon
There is a third possibility that is neither pure withdrawal nor a brand-new condition. It is the idea that cannabis was suppressing (or "masking") a pre-existing anxiety disorder that you may or may not have known about.
Many people start using cannabis in their late teens or early twenties, which is also the age when anxiety disorders most commonly emerge. If cannabis use began around the same time the anxiety disorder was developing, you may have never experienced the full, unmedicated version of your anxiety. Cannabis suppressed it before you had a chance to recognize it as a disorder.
When you quit, the mask comes off. The anxiety that surfaces is not caused by withdrawal and is not new. It is the original condition, finally expressing itself without THC dampening it. This is the "unmasking" phenomenon, and it is one of the most common reasons people who quit cannabis after long-term use feel like their anxiety is uniquely severe.
The unmasking pattern tends to look like this: withdrawal anxiety peaks in weeks 1 to 2 and partially improves, but then plateaus at a level that is still significantly elevated. The withdrawal component resolved, but the underlying condition remains. People in this situation often describe feeling "better than week one, but nowhere near okay." That plateau is the signal that something else is going on.
Understanding whether cannabis was self-medicating an existing anxiety condition is a critical part of figuring out your next steps.
| Feature | Withdrawal Anxiety | Pre-Existing Anxiety | Unmasking |
|---|---|---|---|
| Onset | Within 1–3 days of quitting | Present before cannabis use | Appears after quitting but does not fully resolve |
| Trajectory | Peaks days 2–6, improves by weeks 3–4 | Steady intensity, no withdrawal arc | Partially improves, then plateaus |
| Pattern | Generalized dread, not trigger-specific | Specific patterns (social, panic, GAD) | May have specific patterns that emerge as withdrawal fades |
| Accompanying symptoms | Full withdrawal cluster (insomnia, irritability, appetite loss) | Anxiety is dominant or only symptom | Withdrawal cluster fades but anxiety remains |
| Family history | Not necessarily relevant | Often present | Often present |
| Resolution | Resolves with time (4–6 weeks) | Requires targeted treatment | Withdrawal layer resolves; underlying condition needs treatment |
Diagnostic Tool
Three Anxiety Patterns — Which One Matches Yours?
Track your anxiety 1–10 daily. The trajectory tells you what you're dealing with.
Withdrawal anxiety
Peaks days 2–6, then steadily drops
What to do: Resolves by weeks 3–4 on its own
Pre-existing anxiety
Stays at a steady level — no withdrawal arc
What to do: Needs targeted treatment (therapy, possibly medication)
Unmasking (both)
Partially improves, then plateaus above normal
What to do: Withdrawal layer fades; underlying condition remains
How to use this: Rate your anxiety 1–10 each morning. After 3 weeks, look at the trend. Dropping steadily? Withdrawal. Flat line? Pre-existing. Dropped then stuck? Unmasking.
Timeline: Budney et al. (2003); CB1 recovery: Hirvonen et al. (2012)
A Framework for Sorting It Out
This is not a diagnostic tool. It is a set of questions that can help you and a healthcare provider work through the layers.
When did anxiety first appear in your life? If it predates cannabis use by years, the odds favor a pre-existing condition. If it only appeared after you quit, withdrawal is the more likely explanation.
What does the trajectory look like? Track your anxiety daily on a simple scale. Withdrawal anxiety shows a clear, if bumpy, downward trend over 3 to 4 weeks. Pre-existing anxiety holds steady or fluctuates without an overall downward direction.
What other withdrawal symptoms are present? If your anxiety is accompanied by insomnia, irritability, appetite loss, and sweating, the full withdrawal picture is present. If anxiety is the dominant or only symptom and others have faded, the withdrawal explanation becomes less sufficient.
Does the anxiety have a specific pattern? Pure withdrawal anxiety is usually generalized, a vague sense of dread or unease that does not attach to specific triggers. Anxiety disorders often have triggers, situations, or patterns. Social anxiety spikes around people. Panic disorder involves discrete attacks with specific physical symptoms. Phobias attach to identifiable objects or situations.
Is there a family history? Genetics load the gun. If anxiety disorders run in your family, your baseline risk is higher regardless of cannabis use.
Why This Distinction Matters
The practical reason to figure this out is that the two conditions require different responses.
Withdrawal anxiety requires patience. It will improve on its own as your brain recalibrates. Supporting yourself through it with exercise, breathing techniques, sleep hygiene, and social connection helps, but time is the primary treatment. The broader landscape of weed and anxiety explains these neurochemical patterns in more depth.
Pre-existing anxiety requires treatment. Cognitive behavioral therapy has strong evidence for most anxiety disorders. Medication may be appropriate in some cases. Lifestyle interventions matter too, but they are typically not sufficient on their own for a diagnosable anxiety disorder. Waiting and hoping it will pass, the way you would with withdrawal, can mean months or years of unnecessary suffering.
If it is the unmasking scenario, both are happening at once. You need patience for the withdrawal component and active treatment for the underlying condition. A provider who understands cannabis withdrawal can help you navigate both simultaneously.
Safety
ModerateDon't wait 6 weeks if it's already severe
Concern
The guidance to 'wait and see if it's withdrawal' assumes manageable anxiety. If anxiety is severe enough to prevent you from working, eating, sleeping, or maintaining basic daily life — regardless of the cause — you need support now.
What the research says
A good clinician won't rush to a diagnosis during early withdrawal. They'll help you cope now and refine the assessment as the neurochemical picture clears. Getting help early doesn't lock you into a label.
Particularly relevant for: Anyone whose anxiety is functionally impairing during any stage of withdrawal
What to do
If anxiety is preventing normal functioning at any point — even day 3 — see a healthcare provider or call SAMHSA at 1-800-662-4357. You don't have to wait for the withdrawal window to close before getting help.
Clinical guidance for anxiety assessment during cannabis withdrawal
When to Get Evaluated
There is no perfect moment, but there are clear signals that professional evaluation is warranted.
If anxiety is severe enough to impair daily functioning, regardless of the cause, you deserve support now. You do not have to wait until week 6 to seek help.
If you have a history of anxiety that predates cannabis use, a clinician can begin building a treatment plan even during the withdrawal window, adjusting it as the picture clarifies.
If anxiety has not improved meaningfully by week 4 to 6, the withdrawal explanation is running out of time. This is the point where evaluation becomes especially important.
If you experience panic attacks, persistent dread, or avoidance behaviors that are limiting your life, these suggest a condition that needs its own treatment rather than simply time.
A good clinician will not rush a diagnosis. They will work with you through the withdrawal period, monitor the trajectory, and refine their assessment as the neurochemical noise clears. The goal is not to slap a label on what you are feeling. It is to get you the right kind of help.
When to Seek Professional Help
If anxiety is significantly affecting your ability to work, sleep, maintain relationships, or function day to day, professional support can make the process much more manageable, whether the cause is withdrawal, a pre-existing condition, or both.
Seek help immediately if you experience severe panic, persistent depersonalization, or thoughts of self-harm at any point. SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
The Bottom Line
The question "is this withdrawal or is this real anxiety" is one of the most common things people ask after quitting cannabis. The honest answer is that you probably cannot tell for certain in the first few weeks, and that is okay. What you can do is track the trajectory, pay attention to the pattern, be honest about your history, and seek professional support if the anxiety does not improve on the expected timeline.
The worst thing you can do is assume it must be permanent and go back to using as the only way to cope. The second worst thing is to assume it is all just withdrawal and ignore signs that something deeper needs attention. The path between those two mistakes is patience combined with self-awareness, and a willingness to get professional help when the data points in that direction.
The Bottom Line
Withdrawal anxiety and pre-existing anxiety feel identical because they use the same brain systems — an overactive amygdala, underperforming GABA, and elevated cortisol. The most reliable way to distinguish them is timing and trajectory. Withdrawal anxiety begins within 1 to 3 days of quitting, peaks between days 2 and 6, and improves significantly by weeks 3 to 4 as CB1 receptors normalize. Pre-existing anxiety was present before cannabis use, does not follow the withdrawal timeline, and often has recognizable patterns like social anxiety, panic disorder, or generalized worry. A third possibility is the "unmasking" phenomenon, where cannabis suppressed a developing anxiety disorder for years and quitting reveals what was always there. Tracking anxiety daily on a 1-to-10 scale provides the objective data needed to identify the pattern. If anxiety has not improved meaningfully by weeks 4 to 6, professional evaluation for an underlying condition is warranted.
Sources & References
- 1RTHC-00349·Crippa, Jose Alexandre S. et al. (2009). “Cannabis both calms and panics — the biphasic dose-response explains why the same drug produces opposite anxiety effects.” Human Psychopharmacology: Clinical and Experimental.Study breakdown →PubMed →↩
- 2RTHC-00134·Budney, Alan J. et al. (2003). “When Heavy Users Quit Cannabis, Symptoms Show Up Fast and Ease Within Two Weeks.” Journal of Abnormal Psychology.Study breakdown →PubMed →↩
- 3RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩
- 4RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩