THC and Your Prefrontal Cortex: What Cannabis Does to Your Decision-Making Brain
Balanced Cannabis Science
72 Hours
Your prefrontal cortex has one of the brain's highest concentrations of CB1 receptors, but a 2018 meta-analysis found most cannabis-related cognitive deficits begin clearing within just 72 hours of abstinence.
Molecular Psychiatry, 2012
Molecular Psychiatry, 2012
View as imageIf you only read one thing
THC hits the front part of your brain — the part that handles decisions, self-control, and short-term memory — harder than almost anywhere else. If you use daily, your brain turns down the volume on those receptors to cope. The good news: for adults, the damage starts reversing within 2 days of stopping and mostly clears up within a month. The big exception is people who started heavy use as teenagers — one study following over 1,000 people found an 8-point IQ drop that didn't fully come back even after quitting.
There is a reason you cannot find your keys when you are high. Or why a 2 a.m. food order that seemed perfectly reasonable last night looks baffling in the morning. Or why you keep meaning to start that project but somehow never do. The part of your brain responsible for those functions, your prefrontal cortex, is precisely where THC hits hardest.
The prefrontal cortex (PFC) sits right behind your forehead. It is the last brain region to evolve and the last to mature. It handles the things that make you specifically you: planning, decision-making, impulse control, working memory, social behavior, and the ability to weigh future consequences against present desires. It is also loaded with CB1 receptors, the primary docking sites for THC. That combination matters.
Key Takeaways
- Your prefrontal cortex (PFC) — the front part of your brain that handles decisions, impulse control, and planning — has one of the highest concentrations of CB1 receptors, the docking sites where THC binds
- When you are high, THC temporarily scrambles working memory, attention, and impulse control by disrupting normal signaling in the PFC
- Chronic heavy use causes your brain to pull CB1 receptors offline — called downregulation — but brain imaging shows those receptors largely bounce back after about 28 days of abstinence
- Most cognitive deficits from cannabis are reversible — a 2018 meta-analysis found that impairments start clearing up after just 72 hours without using
- The big exception is teen use — the PFC does not finish developing until around age 25, and one long-term study found an 8-point IQ drop in people who started heavy use as teenagers
- There is a catch-22: the PFC is the brain region you need to decide to change your cannabis use, and it is also the region most affected by it, which is why outside structure and support matter so much during quitting
What CB1 Receptors Do in Your Prefrontal Cortex
Your endocannabinoid system runs on two main receptors: CB1 and CB2. CB1 receptors are concentrated throughout the brain, but the prefrontal cortex has one of the highest densities. Under normal conditions, your body produces its own cannabinoids (called endocannabinoids) that bind to these receptors in small, precisely timed bursts. They act as a fine-tuning system, adjusting the strength of signals between neurons.
Prefrontal Cortex
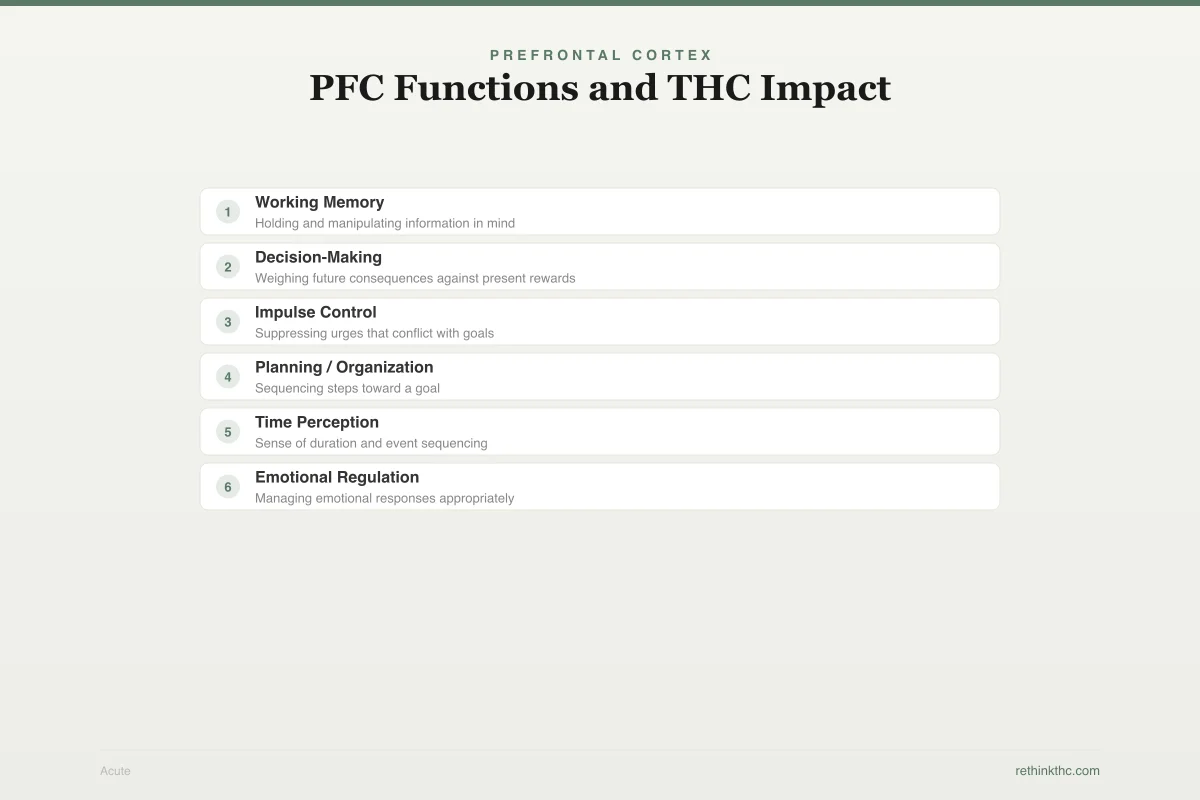
PFC Functions and THC Impact
How THC affects each prefrontal cortex function — acute (while high) vs. chronic (daily use)
Working Memory
Holding and manipulating information in mind
Acute
Chronic
Decision-Making
Weighing future consequences against present rewards
Acute
Chronic
Impulse Control
Suppressing urges that conflict with goals
Acute
Chronic
Planning / Organization
Sequencing steps toward a goal
Acute
Chronic
Time Perception
Sense of duration and event sequencing
Acute
Chronic
Emotional Regulation
Managing emotional responses appropriately
Acute
Chronic
In the PFC, this fine-tuning is critical. Your prefrontal cortex works by maintaining and manipulating information over short periods (working memory), inhibiting impulses that conflict with your goals, and coordinating input from other brain regions to make decisions. Endocannabinoids help regulate the timing and intensity of these processes.
When THC enters your brain, it binds to the same CB1 receptors. But unlike your natural endocannabinoids, which are released in tiny, targeted amounts and broken down quickly, THC floods the system and lingers. Instead of fine-tuning, it is overwhelming the controls.
What Happens to Your PFC When You Get High
The acute effects of THC on the prefrontal cortex are well documented and explain many of the experiences people report while high.
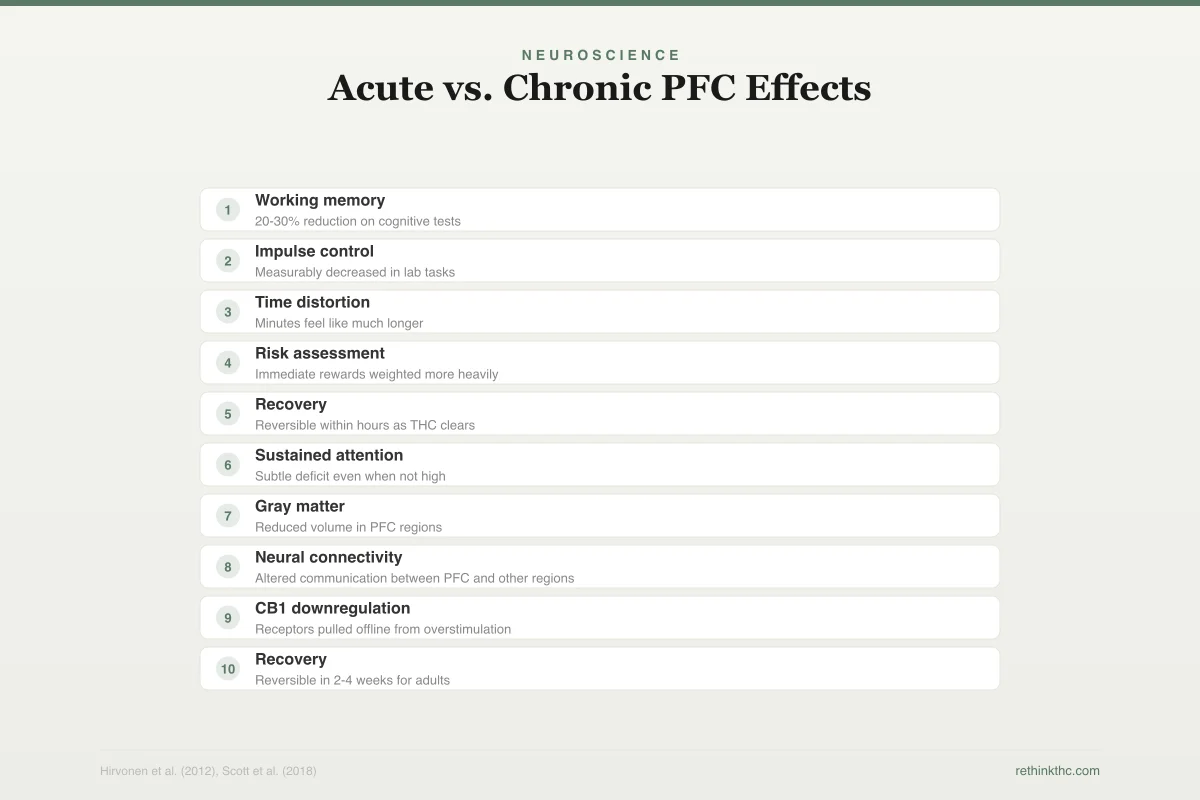
Neuroscience
Acute vs. Chronic PFC Effects
Acute (While High)
20-30% reduction on cognitive tests
Measurably decreased in lab tasks
Minutes feel like much longer
Immediate rewards weighted more heavily
Reversible within hours as THC clears
Chronic (Daily for Months)
Subtle deficit even when not high
Reduced volume in PFC regions
Altered communication between PFC and other regions
Receptors pulled offline from overstimulation
Reversible in 2-4 weeks for adults
Working memory drops. Working memory is your brain's scratchpad. It is what lets you hold a phone number in your head while you walk to grab a pen, or follow a conversation with multiple threads. THC impairs this by disrupting the prefrontal neurons that maintain information in active states. This is why you lose your train of thought mid-sentence, forget what you walked into a room for, or cannot follow a complex plot while watching a movie.
Impulse control weakens. The PFC is your brain's brake system. It evaluates impulses from other brain regions (especially the reward-seeking limbic system) and decides which ones to act on and which to suppress. THC loosens those brakes. This is why you eat the entire bag of chips, send the text you would normally reconsider, or agree to plans you would not normally agree to. It is not that THC creates new desires. It reduces your brain's ability to say "not right now" to desires that were already there.
Time perception shifts. The PFC is involved in temporal processing, your sense of how much time has passed and how to sequence events. THC disrupts this, which is why five minutes can feel like thirty and why high-you is genuinely surprised that an hour has passed.
Decision-making changes. Decisions require weighing present rewards against future costs. That calculation happens in the PFC. THC tips the scale toward the present, making immediate rewards feel larger and future consequences feel more abstract. This is not stupidity. It is a specific, measurable shift in how your brain computes value.
Volkow's 2014 review in the New England Journal of Medicine documented these effects across multiple domains, noting that THC's impact on the PFC explains many of the behavioral changes associated with cannabis use, including impaired decision-making and reduced motivation.
Chronic Use: When Your Brain Adapts
If you use cannabis occasionally, the effects described above wear off as THC clears your system. But with regular, daily use, your brain starts adapting to the constant presence of THC at CB1 receptors.
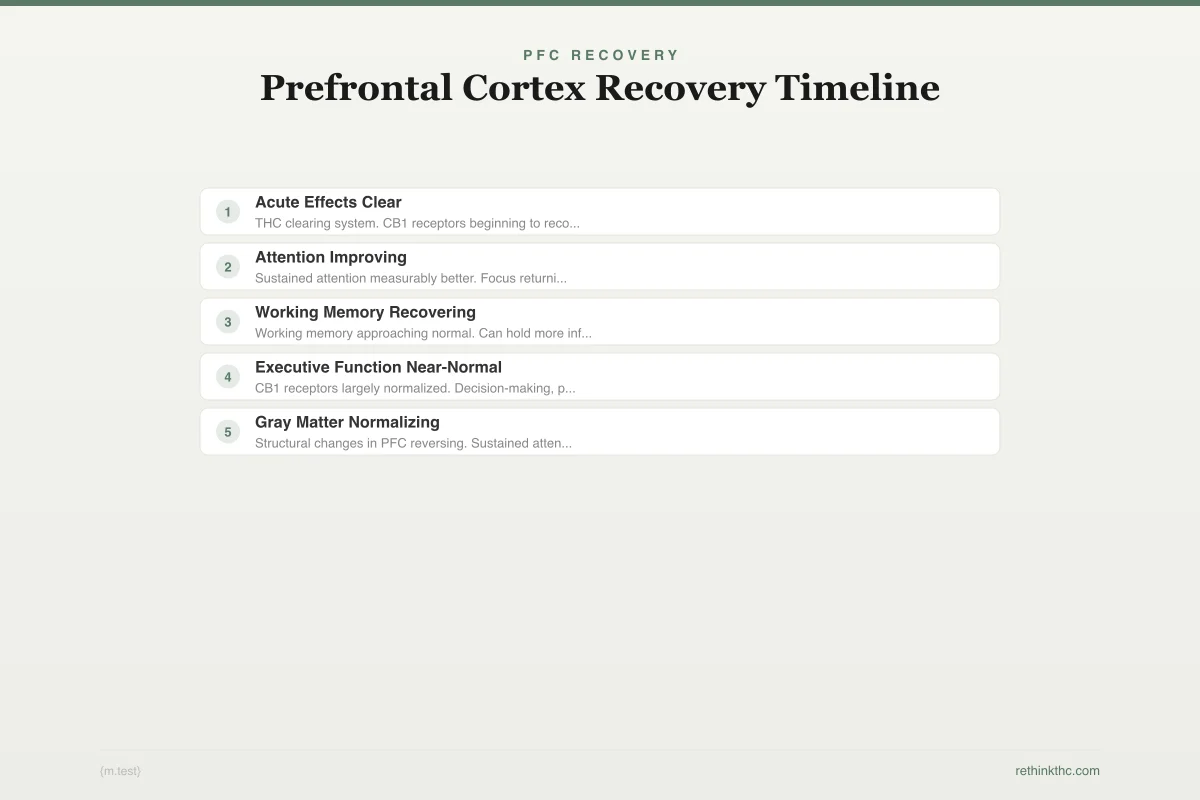
PFC Recovery
Prefrontal Cortex Recovery Timeline
Cognitive function recovery after quitting cannabis (adult users)
THC clearing system. CB1 receptors beginning to recover. Acute cognitive impairment resolving.
D'Souza et al. (2016): receptor recovery begins
Sustained attention measurably better. Focus returning. Less brain fog during conversations.
Noticeable improvement on attention tasks
Working memory approaching normal. Can hold more information in mind. Reading retention improved.
Scott et al. (2018): significant cognitive recovery
CB1 receptors largely normalized. Decision-making, planning, and impulse control near baseline.
Hirvonen et al. (2012): receptor normalization
Structural changes in PFC reversing. Sustained attention fully normal on cognitive tests.
Gruber et al.: cortical density changes
Adolescent-onset users may have a longer recovery trajectory. The PFC does not finish developing until ~age 25.
The primary adaptation is called CB1 receptor downregulation. Your brain literally pulls CB1 receptors offline or reduces their sensitivity. Think of it as your brain turning down the volume on a signal that has been blasting too loud for too long.
Hirvonen's 2012 study in Molecular Psychiatry[1] is the landmark research here. Using PET brain imaging (a scan that can visualize receptor density in living brains), the team compared CB1 receptor availability in daily cannabis users versus non-users. Daily users showed significant CB1 downregulation across the brain, with cortical regions, including the prefrontal cortex, among the most affected areas.
This downregulation has consequences. With fewer functional CB1 receptors in your PFC, the fine-tuning system that normally regulates cognition, decision-making, and impulse control is compromised. This may contribute to the subtle cognitive changes that heavy daily users sometimes notice over time: slightly slower thinking, reduced motivation, difficulty with complex planning, a vague sense of mental fog. For a closer look at the motivation side of this, see the article on weed and motivation.
The Good News: Recovery Is Real and Measurable
This is where the science is genuinely encouraging. CB1 receptor downregulation is not permanent.
Receptor Science
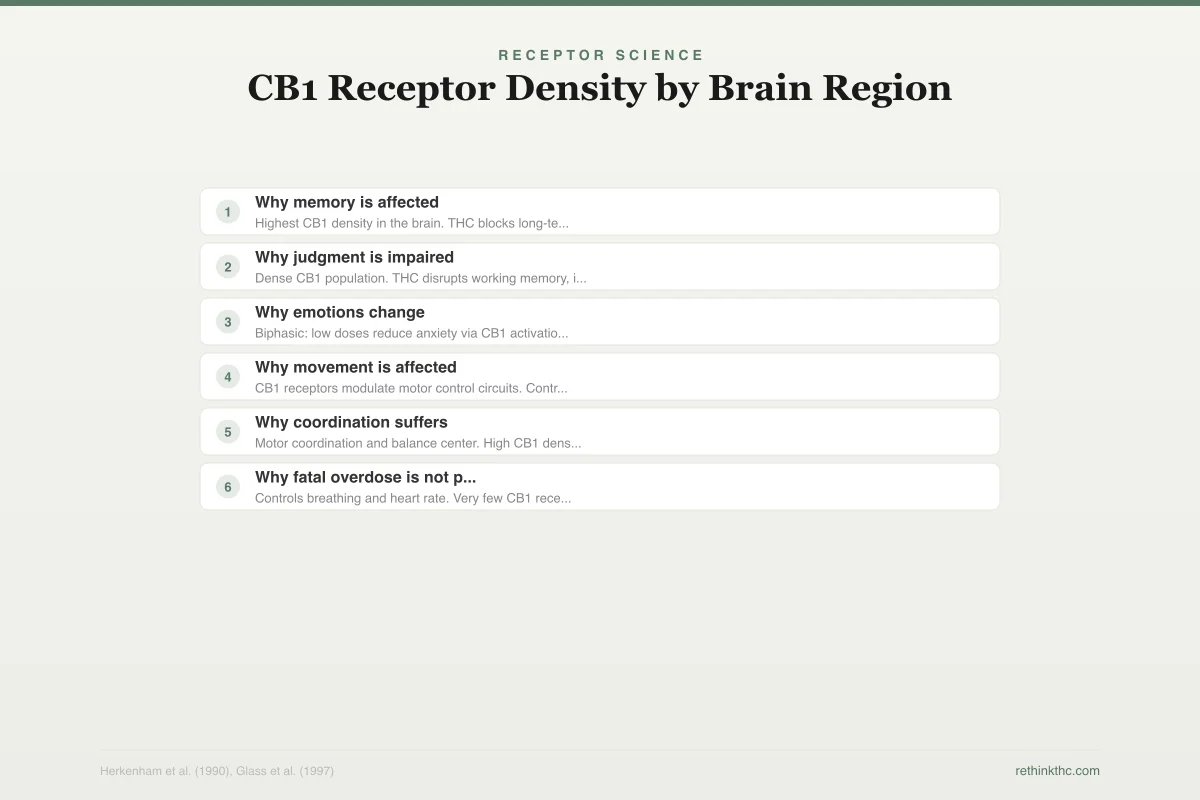
CB1 Receptor Density by Brain Region
Where THC binds determines what it affects. More receptors = greater impact.
Highest CB1 density in the brain. THC blocks long-term potentiation, disrupting new memory formation.
Dense CB1 population. THC disrupts working memory, impulse control, and decision-making.
Biphasic: low doses reduce anxiety via CB1 activation, high doses increase it.
CB1 receptors modulate motor control circuits. Contributes to altered coordination.
Motor coordination and balance center. High CB1 density explains clumsiness while high.
Controls breathing and heart rate. Very few CB1 receptors means THC cannot shut down vital functions.
The same Hirvonen 2012 study[1] included a follow-up: after approximately 28 days of monitored abstinence, the daily users showed significant recovery of CB1 receptor availability. The receptors came back online. And D'Souza's 2016 research[2] demonstrated that this recovery process begins within just 2 days of stopping cannabis use. Your brain does not wait a month to start healing. It starts almost immediately.
The cognitive picture is equally encouraging. Scott's 2018 meta-analysis in JAMA Psychiatry[3] (a study that pooled data from multiple previous studies) examined cognitive function in cannabis users after periods of abstinence. The finding was striking: most cognitive deficits associated with cannabis use remediated after just 72 hours of abstinence. Three days. That does not mean full recovery from years of heavy use happens in 72 hours, but it does mean that the most measurable cognitive impairments, the ones that show up on neuropsychological testing, begin resolving very quickly once THC leaves your system.
For a detailed look at the full receptor recovery timeline, that guide breaks it down week by week.
The Adolescent Exception: Why Age Matters So Much
Everything above applies to adults whose prefrontal cortex has finished developing. If you started using cannabis as a teenager, the picture is more complicated, and the stakes are higher.
The prefrontal cortex is the last brain region to fully mature, completing development around age 25. During adolescence and early adulthood, the PFC is actively building and refining its neural connections through a process called synaptic pruning (the brain eliminating weak connections to strengthen the important ones). This construction phase makes the developing PFC uniquely sensitive to disruption.
Meier's 2012 Dunedin study in PNAS (Proceedings of the National Academy of Sciences)[4] is the most important piece of research on this topic. The study followed 1,037 individuals from birth to age 38, tracking cannabis use and cognitive function throughout. The key finding: people who began persistent, heavy cannabis use during adolescence showed an average 8-point decline in IQ from childhood to adulthood. Critically, this decline was not fully recovered after stopping use, and it was not found in people who began heavy use as adults.
Safety
ModerateAdolescent use carries higher risk
Concern
The prefrontal cortex doesn't finish developing until around age 25. Heavy cannabis use during this window appears to cause cognitive changes that don't fully reverse, even years after quitting.
What the research says
The Dunedin study's 8-point IQ decline was specific to persistent heavy use starting in adolescence. Occasional teen use, or heavy use starting in adulthood, showed much smaller or no lasting effects.
Particularly relevant for: Anyone under 25, especially those under 18
What to do
If you're under 25 and using regularly, reducing or stopping gives your still-developing brain the best chance. If you started as a teen and have already quit, know that many people still report significant subjective improvements in thinking and clarity.
Meier et al. (2012), Volkow et al. (2014)
Eight IQ points may not sound dramatic, but at a population level it is significant. It is the difference between average and low-average cognitive functioning. And the fact that it persisted even after quitting suggests that THC exposure during the PFC's critical development window can cause lasting structural changes.
Jacobus's 2009 research on adolescent cannabis users found that cognitive deficits were still measurable after 3 to 4 weeks of abstinence, a period long enough for CB1 receptors to recover in adults. This suggests that the adolescent brain's vulnerability is not just about receptor disruption. It is about THC interfering with the developmental process itself.
Volkow's 2014 review in the New England Journal of Medicine quantified the risk: approximately 17% of people who begin using cannabis in adolescence develop dependence, compared to 9% of those who start as adults. The developing PFC may be part of the reason. An immature impulse-control system is less equipped to regulate use, and the neurological effects of use during that period further compromise the system that would otherwise help moderate future behavior.
What This Means for Your Decisions Right Now
If you are an adult who uses cannabis regularly, the evidence suggests that your prefrontal cortex is affected but recoverable. CB1 receptors normalize. Cognitive function returns. The mental fog lifts. The 28-day mark appears to be a meaningful milestone for receptor recovery, and measurable cognitive improvement begins within 72 hours of your last use.
If you are weighing whether to quit, cut back, or take a tolerance break, the PFC research supports all three. Any reduction in use gives your prefrontal cortex a chance to recalibrate. Even a planned tolerance break of a few weeks can produce noticeable improvements in clarity, motivation, and decision-making.
If you started using as a teenager and are now wondering whether the damage is done, the answer is nuanced. Meier's research does show lasting effects from adolescent-onset persistent use, but "lasting" does not mean "nothing improves." Many former heavy teen users report significant subjective improvements in cognition and executive function after quitting, even if standardized testing shows some residual effects. The brain has more plasticity than any single study can fully capture.
The Irony of PFC Impairment
There is a catch-22 worth naming. The prefrontal cortex is the brain region you need to decide to change your cannabis use. It is also the region most affected by cannabis use. If your PFC is compromised by chronic THC exposure, the very cognitive functions you need to plan a break, resist impulses, and follow through on decisions are running at reduced capacity.
This is not an excuse. It is an explanation. If you have tried to quit or cut back and found it harder than expected, part of the difficulty may be neurological. Your brake system is impaired, and you are asking it to stop the car. This is one reason why external structure, whether it is a quit plan, an accountability partner, or professional support, can be so valuable. You are outsourcing some PFC function to your environment until your brain recovers enough to handle it internally.
When to Seek Professional Help
If you are experiencing persistent cognitive difficulties that interfere with work, school, or daily life, whether or not you are currently using cannabis, a neuropsychological evaluation can clarify what is going on. If you have been using heavily since adolescence and are concerned about long-term effects, a healthcare provider can help you understand your specific situation and develop a plan.
If you are finding it difficult to quit or cut back despite wanting to, that is also worth discussing with a professional. Cannabis use disorder is a recognized medical condition with effective treatments, and difficulty quitting does not mean you lack willpower. It means your brain's regulatory system needs support.
SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day, 7 days a week. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
The Bottom Line
The prefrontal cortex (PFC), responsible for decision-making, impulse control, and planning, has one of the highest densities of CB1 receptors in the brain. THC acutely impairs working memory, impulse control, time perception, and decision-making by overwhelming the PFC's fine-tuning system. Chronic use causes CB1 receptor downregulation, but brain imaging shows receptors largely normalize after 28 days of abstinence. A 2018 meta-analysis found most cognitive deficits remediate after just 72 hours. The major exception is adolescent use: the Dunedin study following 1,037 people found an 8-point IQ decline in those who began persistent heavy use as teenagers, an effect not seen in adult-onset users and not fully reversed after quitting. About 17% of adolescent-onset users develop dependence versus 9% of adult-onset users.
Sources & References
- 1RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩
- 2RTHC-01134·D'Souza, Deepak Cyril et al. (2016). “Brain Cannabinoid Receptors Drop With Heavy Use, Then Rebound Within Days of Stopping.” Biological Psychiatry: Cognitive Neuroscience and Neuroimaging.Study breakdown →PubMed →↩
- 4RTHC-00591·Meier, Madeline H. et al. (2012). “From Teen Years to 38: Heavy, Long-Term Cannabis Use Tracked With Lower Cognitive Scores.” Proceedings of the National Academy of Sciences (PNAS).Study breakdown →PubMed →↩