Cannabis Effects and Experience: The Science Behind Your High
Science
5 mg Gap
A University of Chicago study found that just 5 milligrams of THC separates a calming cannabis experience from one that spikes anxiety, confirming how narrow the therapeutic dose window really is.
Childs et al., Drug and Alcohol Dependence, 2017
Childs et al., Drug and Alcohol Dependence, 2017
View as imageIf you only read one thing
Cannabis doesn't produce one effect — it produces a whole spectrum, and where you land depends on dose, your genetics, your tolerance, your mood, and even what you ate. A University of Chicago study found that just 5 milligrams of THC separates a calming experience from a panic attack. Every effect you feel — hunger, time warping, paranoia, euphoria — maps to a specific brain region with cannabinoid receptors. And if weed 'used to be fun but now just makes me anxious,' that's not random — it's your brain's receptors adapting unevenly.
You take a hit and within minutes your body is doing a dozen things it was not doing before. Your eyes redden. Your mouth goes dry. Food smells extraordinary. A song you have heard five hundred times suddenly has layers you never noticed. Or maybe none of that happens and instead your heart races, your thoughts spiral, and you spend forty minutes convinced your roommate is mad at you for reasons you cannot articulate.
Cannabis does not produce one effect. It produces a spectrum of effects, and where you land on that spectrum depends on a remarkable number of variables, most of which have nothing to do with the strain name on the jar. The neuroscience behind all of it is genuinely fascinating, and understanding it changes how you think about every experience you have ever had with cannabis.
Key Takeaways
- THC works by locking onto CB1 receptors across your brain — mimicking your body's natural bliss molecule anandamide but hitting much harder and lasting far longer
- Cannabis effects and experience follow a two-phase pattern — low doses tend to calm you and lift your mood, while high doses can trigger paranoia, racing thoughts, and panic
- Why the same strain hits differently every time comes down to at least six things — dose, tolerance, genetics, terpene profile, your mental state going in, and your physical environment
- The "weed used to be fun but now it just makes me anxious" experience is real — it reflects long-term changes in receptor density, stress-system sensitivity, and your shifting baseline anxiety
- Cannabinoid hyperemesis syndrome is a condition where chronic heavy use paradoxically causes severe cyclical vomiting — affecting an estimated 2.7 million regular users in the U.S.
- A 2017 University of Chicago study found that the difference between a calming and an anxiety-spiking cannabis experience was just 5 milligrams of THC — confirming how narrow that dose window really is
How THC Works in Your Brain
To understand cannabis effects, you need to understand the system it targets. Your brain runs a signaling network called the endocannabinoid system (ECS), discovered in the early 1990s by researchers who were trying to figure out why THC does what it does. The ECS turned out to be one of the most widespread regulatory systems in the human body, governing mood, appetite, sleep, pain, memory, and stress response.
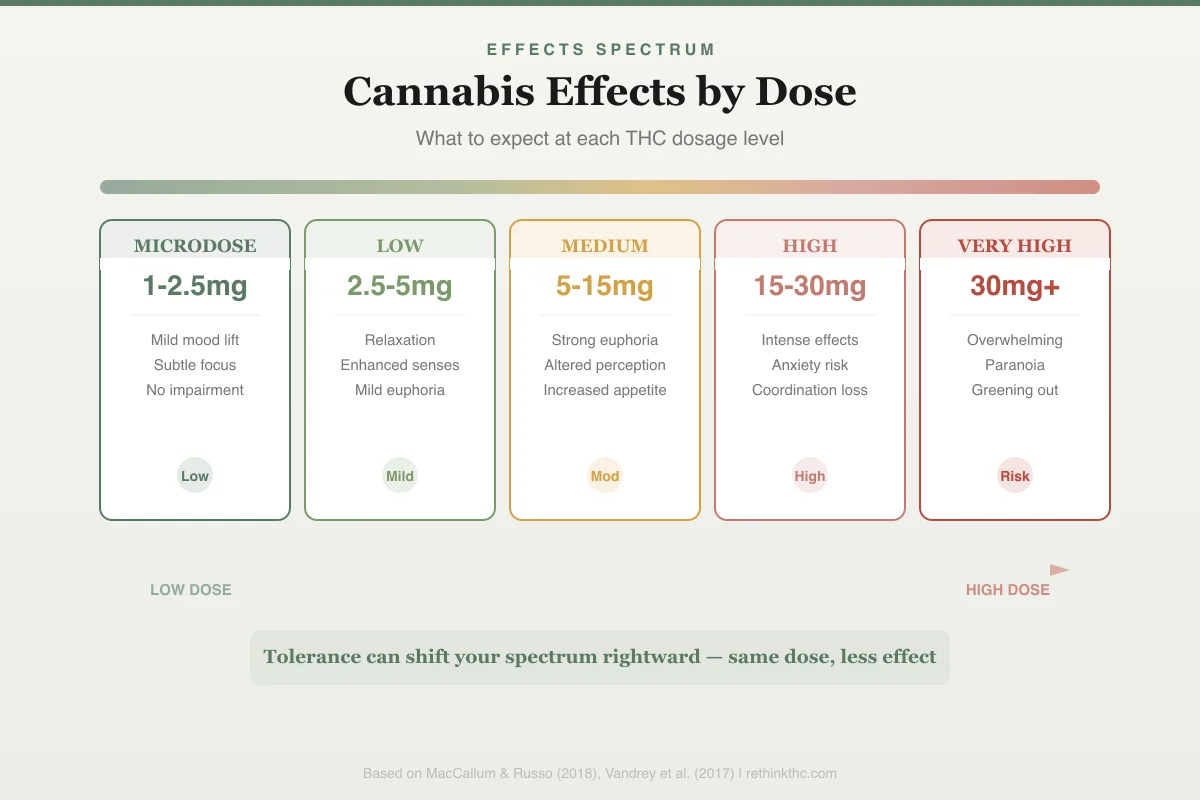
Effects Spectrum
Cannabis Effects by Dose
What to expect at each THC dosage level
Mild mood lift · Subtle focus · No impairment
Relaxation · Enhanced senses · Mild euphoria
Strong euphoria · Altered perception · Increased appetite
Intense effects · Anxiety risk · Coordination loss
Overwhelming · Paranoia · Greening out
Tolerance can shift your spectrum rightward — same dose, less effect
The ECS operates through two main receptors. CB1 receptors are densely concentrated in the brain, particularly in regions that control pleasure (the nucleus accumbens), memory (the hippocampus), coordination (the cerebellum), time perception (the basal ganglia), sensory processing (the cortex), and fear and anxiety (the amygdala). CB2 receptors sit primarily in the immune system and gut.
Your body makes its own chemicals to activate these receptors: anandamide and 2-AG. These endocannabinoids are produced on demand in tiny, precise amounts, do their signaling work in seconds, and are immediately broken down by enzymes. The whole system is designed for brief, targeted bursts of activity.
THC disrupts this design completely. Its molecular shape is similar enough to anandamide that it fits into CB1 receptors, but the similarity ends there. THC activates these receptors with significantly greater intensity than anandamide and lingers for hours instead of seconds. When you smoke or ingest cannabis, you are flooding a precision signaling system with a blunt, powerful, long-lasting signal.
Every effect you feel, the euphoria, the hunger, the altered time perception, the paranoia, maps directly to which brain regions have CB1 receptors and what those regions do when they receive this amplified signal. The prefrontal cortex effects alone explain much of what people describe as feeling "high."
The Acute Effects Spectrum
Cannabis does not do one thing to everyone. It produces a range of effects that vary by person, dose, and context. Here is what the neuroscience says about each major effect.
Euphoria and Mood Elevation
The "high" starts in the mesolimbic dopamine pathway, the same reward circuit involved in food, sex, music, and every addictive substance ever studied. THC activates CB1 receptors on GABA neurons in the ventral tegmental area (VTA). GABA is an inhibitory neurotransmitter, meaning these neurons normally act as brakes on dopamine release. When THC suppresses those brakes, dopamine floods the nucleus accumbens. A 2015 PET imaging study in healthy volunteers found that THC increased dopamine release in the striatum by approximately 3 to 8 percent, a modest increase compared to stimulants but enough to produce significant subjective pleasure.
This is why the early part of a high often feels expansive, warm, and vaguely magical. You are experiencing a pharmacologically induced surge in the exact neurotransmitter your brain associates with "this is good, do more of this." This dopamine-driven mood elevation is also why cannabis makes people laugh more readily, lowering the threshold for finding things funny.
Appetite Stimulation
The munchies are not psychological. THC activates CB1 receptors in the hypothalamus, the brain region that regulates hunger. Research published in Nature Neuroscience in 2015 demonstrated something remarkable: THC actually flips the function of POMC neurons. These neurons normally signal satiety (fullness). Under THC's influence, they do the opposite: they start signaling hunger. Your brain's "I am full" circuit literally starts saying "I am starving."
Simultaneously, THC enhances olfactory sensitivity, making food smell more intense, and activates CB1 receptors in the nucleus accumbens, making the taste of food more rewarding. You are hungrier than you should be, food smells better than it should, and eating it feels more pleasurable than it normally would. The munchies are a coordinated neurological event, not a lack of willpower. For a deeper look at the appetite mechanism, see why weed makes you hungry and why food tastes better when you are high.
Time Distortion
Nearly every cannabis user reports that time seems to slow down. A 2012 meta-analysis in Psychopharmacology reviewed studies on cannabinoids and time perception and confirmed that THC consistently impairs interval timing, causing users to overestimate how much time has passed. Five minutes feels like twenty.
The mechanism involves CB1 receptors in the basal ganglia and cerebellum, which are heavily involved in the brain's internal clock. THC disrupts the steady neural oscillations that your brain uses to track time intervals. When those oscillations become irregular, your subjective experience of duration becomes unreliable. This is also why activities feel like they last forever and why music can feel so immersive: you are processing each moment as though it contains more time than it actually does. The full science of why weed makes time feel slow goes deeper into the neural oscillation research.
Sensory Enhancement
Colors seem brighter. Music sounds richer. Touch feels more electric. This is not imagination. THC increases activity in sensory processing areas of the cortex, and it does so by disinhibiting neural circuits that normally filter sensory input. Normally, your brain aggressively filters incoming sensory data to prevent overwhelm. THC loosens that filter. More raw sensory information reaches conscious awareness, and the nucleus accumbens simultaneously tags that information as more rewarding than usual.
The result is that ordinary sensory experiences feel novel and heightened. This is one of the most reliably reported effects, particularly when it comes to why music sounds better when high, and it maps cleanly to the neuroscience of cortical disinhibition combined with enhanced reward signaling. The same disinhibition of default filtering may also explain why people feel more creative when high, as loosened associative constraints allow more divergent thinking.
Paranoia and Anxiety
Here is where cannabis effects get complicated and where the neuroscience becomes critically important. THC activates CB1 receptors in the amygdala, the brain's threat detection center. At low doses, this appears to dampen amygdala reactivity, which is why small amounts of cannabis can feel calming. But at higher doses, THC can produce the opposite effect, amplifying amygdala signaling and producing intense, sometimes overwhelming anxiety.
A landmark 2017 study by Papagianni and Bhatt published in the Journal of Psychopharmacology demonstrated that THC's effects on anxiety follow a clear biphasic pattern. Low doses reduce anxiety ratings in experimental settings, while high doses significantly increase them. The switch point varies between individuals but is remarkably consistent within them.
The paranoia component involves the prefrontal cortex, which normally provides top-down control over the amygdala, essentially telling it "that threat is not real, calm down." THC impairs prefrontal function, reducing your capacity to reality-check anxious thoughts. So you get amplified threat signaling from the amygdala combined with reduced ability to evaluate whether those signals make sense. That is the recipe for paranoia: your alarm system is ringing louder while your rational brain is less able to reach the off switch. The article on why weed makes you paranoid explores this amygdala-prefrontal dynamic in greater detail.
Short-Term Memory Disruption
The stereotypical stoner memory lapse is a direct consequence of CB1 receptor activation in the hippocampus. The hippocampus is where short-term memories are consolidated into long-term storage. THC disrupts long-term potentiation (LTP), the cellular mechanism by which neurons strengthen their connections to form memories. Research in animal models has consistently shown that THC blocks LTP in hippocampal circuits. You can still form memories while high, but the process is less efficient, which is why people forget what they were saying mid-sentence or cannot recall what happened fifteen minutes ago.
Why Effects Vary Between People
Two people can smoke the same joint at the same time and have wildly different experiences. This is not random. It is driven by identifiable biological and psychological variables.
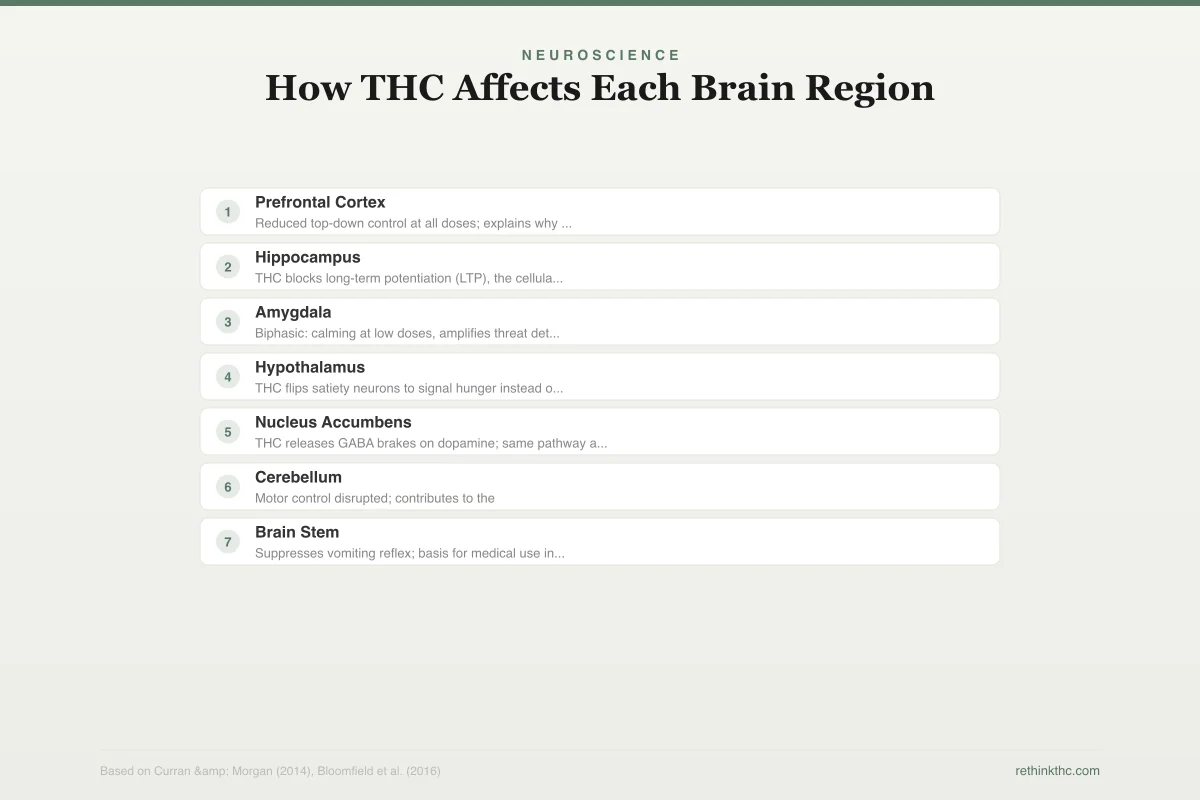
Neuroscience
How THC Affects Each Brain Region
Every cannabis effect maps to a specific brain region with dense CB1 receptors
Altered judgment, time distortion, impaired decision-making
Reduced top-down control at all doses; explains why you cannot "think straight"
Short-term memory disruption, difficulty forming new memories
THC blocks long-term potentiation (LTP), the cellular mechanism for memory consolidation
Reduced fear (low dose) or anxiety and paranoia (high dose)
Biphasic: calming at low doses, amplifies threat detection at high doses
Appetite stimulation ("munchies")
THC flips satiety neurons to signal hunger instead of fullness
Euphoria, dopamine release, reward signaling
THC releases GABA brakes on dopamine; same pathway as food, sex, and all addictive substances
Coordination changes, balance impairment
Motor control disrupted; contributes to the "clumsy high" experience
Anti-nausea effects
Suppresses vomiting reflex; basis for medical use in chemotherapy patients
THC mimics anandamide but with far greater intensity and duration — flooding a precision system with a blunt, powerful signal
Genetics. The gene CNR1 encodes the CB1 receptor. Variations in this gene affect receptor density and sensitivity. People with certain CNR1 variants have naturally fewer CB1 receptors and tend to be less sensitive to THC's effects. The gene FAAH determines how quickly your body breaks down anandamide. People with the FAAH C385A variant, found in roughly 38% of people of European descent, break down anandamide more slowly, meaning they walk around with naturally higher endocannabinoid tone. These individuals may respond differently to THC because their baseline system is already more active.
Tolerance state. Regular cannabis use causes CB1 receptor downregulation, meaning your brain literally removes receptors from cell surfaces. A 2012 study in Molecular Psychiatry showed that chronic users have measurably fewer available CB1 receptors than non-users. Fewer receptors means the same dose produces less effect. But tolerance develops unevenly across brain regions, which is why a daily user might barely feel euphoria from a dose that still impairs their memory. The timeline for receptor recovery after stopping use follows a predictable pattern, with most receptors returning to normal within about four weeks.
Set and setting. "Set" is your mindset going in. "Setting" is your physical and social environment. A 2018 study in Psychopharmacology found that pre-existing anxiety levels were the single strongest predictor of whether THC produced relaxation or panic. If you are already anxious, stressed, or in an unfamiliar environment, the amygdala-amplifying effects of THC are more likely to tip into full-blown anxiety. If you are relaxed, safe, and in good company, the same dose is more likely to produce euphoria. This is not placebo. It is neuroscience: your baseline amygdala activity determines how much additional THC-driven activation it takes to cross the anxiety threshold.
Terpenes and the entourage effect. Cannabis contains over 200 terpenes, aromatic compounds that may modulate THC's effects through interactions with neurotransmitter systems independent of CB1. Myrcene, the most common terpene in cannabis, has demonstrated sedative properties in animal studies. Limonene has shown anxiolytic (anti-anxiety) effects. Linalool has analgesic (pain-reducing) properties. The terpene profile of a given cannabis product may meaningfully shift the experience, which helps explain why some cannabis makes you energetic while other strains make you sleepy, though human clinical data on terpene-cannabinoid interactions remains limited.
Biology matters. Body fat percentage affects THC distribution and duration because THC is lipophilic (fat-soluble). Hormonal fluctuations, particularly estrogen levels, can influence CB1 receptor sensitivity. Even your recent meal affects onset and intensity, especially with edibles.
Why Effects Change Over Time
One of the most common questions in cannabis communities is some version of: "Why did weed used to be great but now it just gives me anxiety?" This is not imagined, and the neuroscience behind it involves several converging mechanisms.
CB1 receptor downregulation. Chronic THC exposure reduces CB1 receptor availability, but it does so unevenly. Receptors in reward-related regions (nucleus accumbens) downregulate substantially, which blunts euphoria. Receptors in the amygdala may be less affected or may develop a different pattern of adaptation. The result is that the anxiogenic (anxiety-producing) effects of THC become more prominent relative to the euphoric effects. This shifting emotional landscape is also why cannabis can make people feel unexpectedly emotional. You are not getting more anxious from the same dose. You are getting less euphoria, which shifts the balance.
Stress system sensitization. Long-term cannabis use alters the hypothalamic-pituitary-adrenal (HPA) axis, the body's central stress response system. Research has shown that chronic cannabis users have altered cortisol responses to stress. When you use cannabis to manage stress for months or years, you may be inadvertently sensitizing the very stress circuitry you were trying to quiet. Over time, THC starts triggering stress responses rather than suppressing them because the underlying system has been reorganized.
Baseline anxiety accumulation. Life does not stand still while cannabis use continues. Many people begin using cannabis in a period of relative low-stress (late teens, early twenties) and continue into phases with more responsibility, financial stress, health concerns, or relationship complexity. The same drug interacting with a fundamentally different anxiety baseline produces a fundamentally different experience.
Tolerance to positive effects outpacing tolerance to negative effects. This is one of the cruelest tricks of pharmacology. Tolerance to THC's euphoric and relaxing effects develops faster than tolerance to its anxiety-producing and memory-impairing effects. The enjoyable aspects fade first. What remains is a drug that makes you anxious and forgetful but no longer makes you feel particularly good.
The Dose-Response Curve: Biphasic Effects
Perhaps the single most important concept for understanding cannabis effects is that THC has a biphasic dose-response curve. This means low doses and high doses produce opposite effects, and the relationship is not linear.
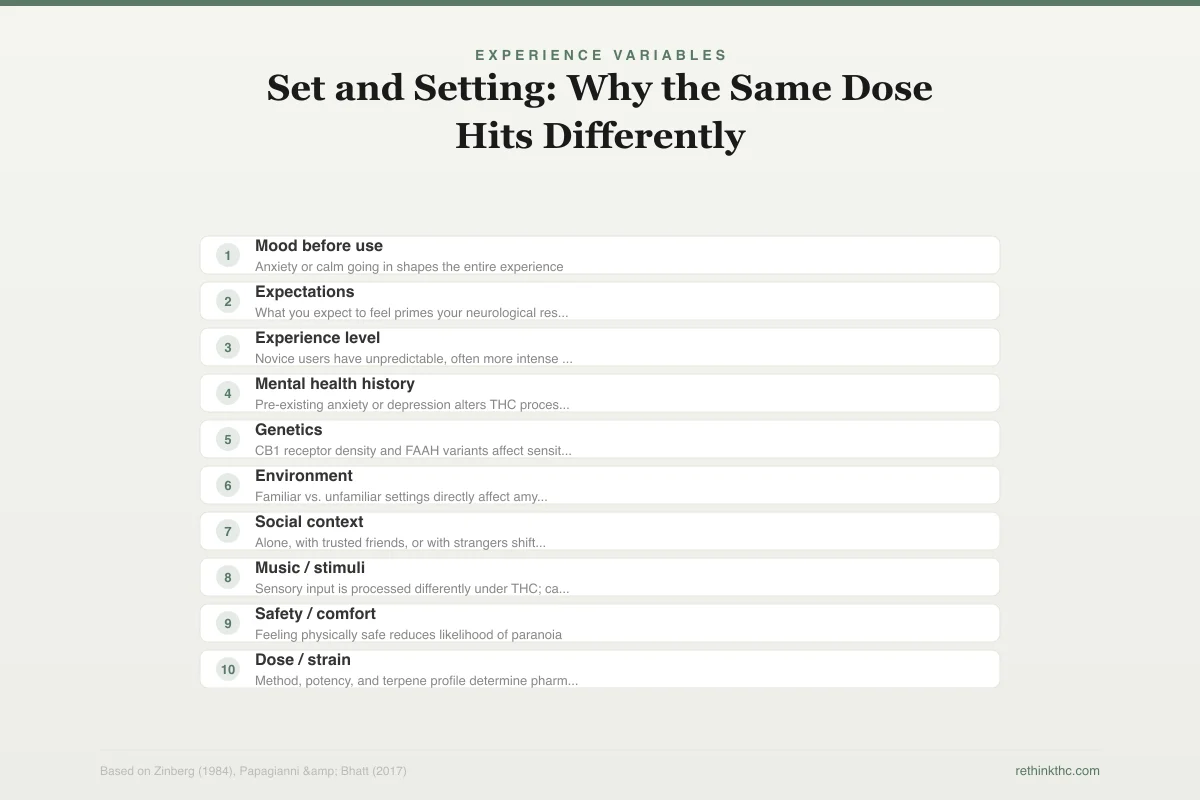
Experience Variables
Set and Setting: Why the Same Dose Hits Differently
Non-pharmacological factors that shape your cannabis experience
Set (Internal)
Your mindset, biology, and psychological state going in
Mood before use
Anxiety or calm going in shapes the entire experience
Expectations
What you expect to feel primes your neurological response
Experience level
Novice users have unpredictable, often more intense reactions
Mental health history
Pre-existing anxiety or depression alters THC processing
Genetics
CB1 receptor density and FAAH variants affect sensitivity
Setting (External)
Your physical environment, social context, and substance variables
Environment
Familiar vs. unfamiliar settings directly affect amygdala reactivity
Social context
Alone, with trusted friends, or with strangers shifts anxiety threshold
Music / stimuli
Sensory input is processed differently under THC; can amplify or calm
Safety / comfort
Feeling physically safe reduces likelihood of paranoia
Dose / strain
Method, potency, and terpene profile determine pharmacological input
The same 10mg edible can produce euphoria or panic depending on these variables — cannabis is not just pharmacology, it is context
At low doses (roughly 2.5 to 5 mg of THC for a non-tolerant individual), THC tends to reduce anxiety, enhance mood, improve sociability, and produce mild euphoria. The amygdala is gently modulated downward. The reward system gets a modest boost. Sensory processing is slightly enhanced without becoming overwhelming.
At high doses (above 10 to 15 mg for a non-tolerant individual, or proportionally higher for regular users), the picture inverts. The amygdala goes into overdrive. The prefrontal cortex loses its ability to regulate. Working memory degrades significantly. Time distortion becomes disorienting rather than interesting. Paranoia can set in. Heart rate increases. For some individuals, very high doses can produce depersonalization, derealization, or frank panic attacks.
A 2017 study at the University of Chicago gave participants either 7.5 mg or 12.5 mg of THC before a simulated job interview. The low-dose group reported reduced stress and more positive emotion compared to placebo. The high-dose group reported significantly more negative emotion and self-rated their performance lower, even though objective measures of performance did not differ. The difference between a good experience and a bad one was 5 milligrams.
This biphasic pattern explains why the experienced cannabis user who switches from flower to concentrates often has a terrible time. The leap in effective dose can push them from one side of the curve to the other in a single session. It also explains why many people find that "less is more" after a tolerance break: with recovered CB1 receptors, a small dose sits comfortably in the low-dose zone that chronic use had pushed them past.
Cannabinoid Hyperemesis Syndrome
At the far end of the chronic-use effects spectrum sits cannabinoid hyperemesis syndrome (CHS), a condition that would seem almost paradoxical if it were not so well-documented. Cannabis is known for reducing nausea. CHS is a condition caused by cannabis that produces severe, cyclical vomiting.
CHS typically develops after years of heavy, daily use. The mechanism is not fully established, but the leading theory involves dysregulation of TRPV1 receptors in the gut and brainstem. These are the same receptors activated by capsaicin (the chemical that makes chili peppers hot), which may explain the hallmark symptom of CHS: compulsive hot water bathing provides temporary relief, likely through competing TRPV1 activation that overrides the nausea signal.
A 2018 epidemiological study estimated that CHS may affect up to one-third of heavy daily cannabis users to some degree, with emergency department visits for cyclical vomiting syndrome increasing significantly in states following cannabis legalization. Many cases go undiagnosed for months or years because neither patients nor clinicians initially suspect cannabis as the cause of vomiting.
The only reliable treatment for CHS is complete cessation of cannabis use. Symptoms typically resolve within one to two weeks of stopping but return rapidly upon resumption. CHS is important because it demonstrates that the body's relationship to cannabinoids has hard limits. The endocannabinoid system is built for intermittent, low-level activation. Sustained, high-intensity activation can produce outcomes that are the exact opposite of what cannabis nominally does.
Safety
ModerateCannabinoid hyperemesis syndrome (CHS)
Concern
Heavy daily cannabis use can cause severe cyclical vomiting — the exact opposite of cannabis's anti-nausea reputation. CHS often goes undiagnosed for months because neither patients nor doctors suspect cannabis as the cause of vomiting.
What the research says
Symptoms typically resolve within 1-2 weeks of completely stopping cannabis. However, they return rapidly if use resumes. Hot showers provide temporary relief during episodes by activating competing receptors (TRPV1).
Particularly relevant for: Daily or near-daily cannabis users, especially those using high-potency products for months to years
What to do
If you use cannabis daily and experience unexplained cyclical nausea or vomiting — especially if hot showers help — talk to a doctor about CHS. The only effective treatment is stopping cannabis entirely.
Williams et al. (2025); epidemiological data showing increased ER visits in legal cannabis states
The "Hit Different" Variables
Beyond the big factors of genetics, tolerance, and dose, there are smaller variables that explain why the same weed hits different sometimes — why the same person using the same product can have different experiences on different days.
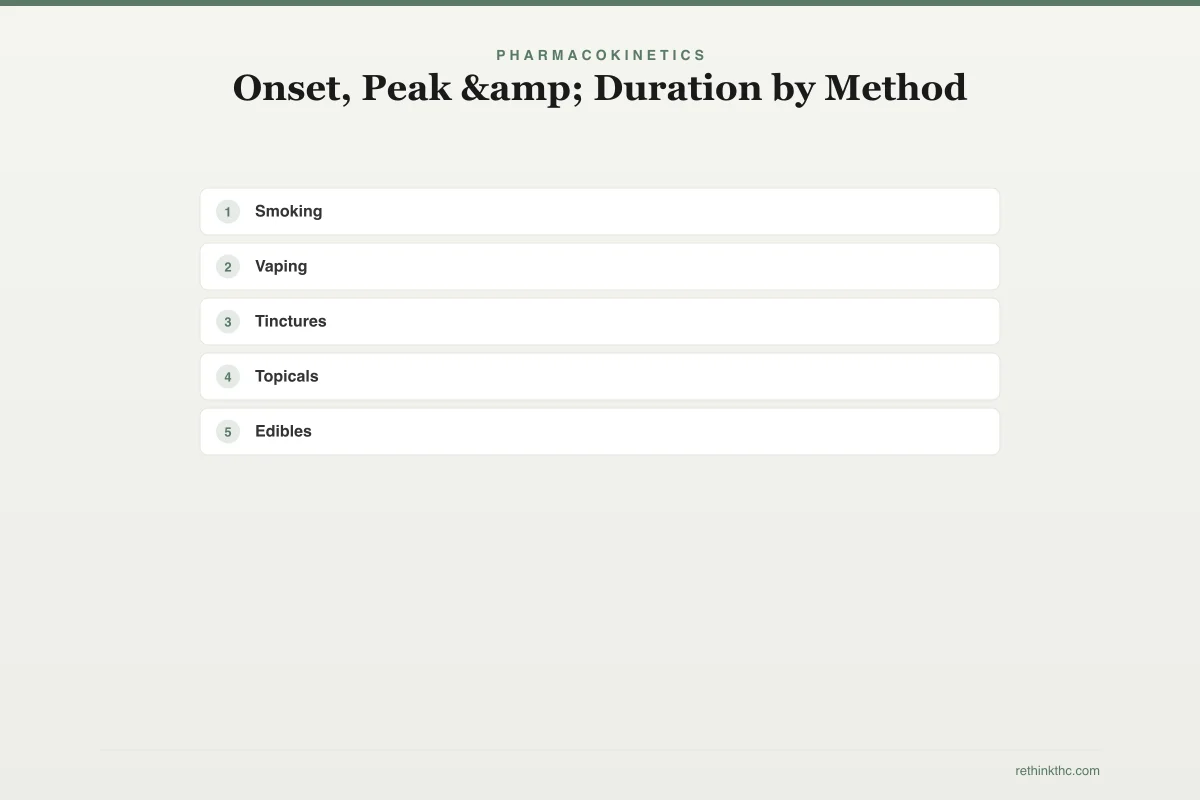
Pharmacokinetics
Onset, Peak & Duration by Method
Timeline comparison of cannabis consumption methods
Smoking
2–3 hr
onset: 1–5 min
Vaping
2–3 hr
onset: 1–5 min
Tinctures
3–6 hr
onset: 15–45 min
Topicals
2–4 hr
onset: 15–45 min
Edibles
4–8 hr
onset: 30–90 min
Sleep deprivation. Being sleep-deprived alters endocannabinoid levels, particularly 2-AG, which shows circadian variation. Using cannabis when sleep-deprived means THC is interacting with a system already running at abnormal levels, producing unpredictable results. For more on the sleep connection specifically, see why weed makes you sleepy.
Alcohol and other substances. Alcohol increases THC absorption and potentiates its effects, which is why mixing weed and alcohol can cause "the spins". Combining the two produces significantly greater impairment than either alone. Caffeine can counteract some of THC's sedating effects but may amplify anxiety.
Blood sugar. Hypoglycemia (low blood sugar) intensifies THC's cognitive and mood effects. Eating before using cannabis provides a more stable experience, and this is doubly true for edibles, where fat content in a recent meal can increase THC bioavailability by 2.5 to 3 times.
Menstrual cycle. Estrogen levels modulate CB1 receptor sensitivity. Research in animal models has shown that females are more sensitive to THC during high-estrogen phases of their cycle. Human data is limited, but many women report that cannabis effects fluctuate with their cycle, and the animal literature provides a plausible mechanism.
Route of administration. Inhaled THC reaches peak blood concentration in 3 to 10 minutes and effects last 2 to 4 hours. Oral THC is converted to 11-hydroxy-THC in the liver, a metabolite that crosses the blood-brain barrier more efficiently and produces a subjectively different, often more intense and longer-lasting high. This is why edibles "hit different" in the most literal pharmacological sense. You are experiencing a different active compound.
What This All Means
The science of cannabis effects is not a simple story of "THC gets you high." It is a complex interaction between a powerful exogenous compound, an intricate endogenous signaling system, individual genetic variation, dynamic tolerance processes, and moment-to-moment physiological state. Understanding this complexity does not make the experience less enjoyable for those who choose to use cannabis. It makes the experience more predictable and safer.
If cannabis has started producing anxiety instead of relaxation, that is not random: it is a predictable consequence of shifting receptor availability and dose-response dynamics. If the same edible hits like a freight train one day and barely registers the next, that is not the product being inconsistent: it is your body's state being different. If you have been vomiting cyclically and no one can figure out why, and you use cannabis daily, CHS belongs on the differential.
Every cannabis experience you have ever had was your neuroscience, not just the plant. The more you understand about the system THC targets, the better equipped you are to make informed decisions about if, how, and how much you choose to use it.
The Bottom Line
Pillar covering neuroscience of every common cannabis effect. THC mimics anandamide at CB1 receptors but with far greater intensity/duration, flooding a precision signaling system. Euphoria: THC suppresses GABA brakes on dopamine in VTA → dopamine floods nucleus accumbens (2015 PET: ~3-8% increase). Appetite: CB1 in hypothalamus flips POMC neurons from satiety→hunger (2015 Nature Neuroscience) + enhanced olfactory sensitivity + increased food reward. Time distortion: CB1 disrupts basal ganglia/cerebellum oscillations used for interval timing (2012 Psychopharmacology meta-analysis). Sensory enhancement: cortical disinhibition loosens sensory filtering + reward tagging. Paranoia: biphasic amygdala effect — low dose dampens, high dose amplifies; impaired prefrontal cortex reduces reality-checking (Papagianni 2017, Journal of Psychopharmacology). Memory: CB1 blocks hippocampal LTP. Variability factors: CNR1 gene (receptor density), FAAH C385A variant (anandamide breakdown), tolerance (uneven CB1 downregulation across regions — Hirvonen 2012), set/setting (pre-existing anxiety = strongest predictor), terpenes, biology. Why effects change over time: reward receptor downregulation outpaces amygdala adaptation → anxiety ↑ relative to euphoria; HPA axis sensitization; tolerance to positives develops faster than to negatives. Biphasic dose-response: U of Chicago study — 7.5mg reduced stress vs 12.5mg increased it (5mg difference). CHS: TRPV1 dysregulation from chronic heavy use → cyclical vomiting; only treatment = cessation.
Sources & References
- 1RTHC-00771·Bhattacharyya, S et al. (2014). “A specific gene variant determined who lost motor control after THC.” Psychological medicine.Study breakdown →PubMed →↩
- 2RTHC-01951·Bloomfield, Michael A P et al. (2019). “A comprehensive review of human brain imaging reveals how cannabis affects executive function, emotion, memory, and reward.” Pharmacology & therapeutics.Study breakdown →PubMed →↩
- 3RTHC-01542·van de Giessen, E et al. (2017). “Cannabis-Dependent People Had Significantly Blunted Dopamine Release in the Brain's Reward System.” Molecular psychiatry.Study breakdown →PubMed →↩
- 4RTHC-01958·Bossong, Matthijs G et al. (2019). “THC boosted brain activity in attention networks, and a common gene variant influenced the effect.” European neuropsychopharmacology : the journal of the European College of Neuropsychopharmacology.Study breakdown →PubMed →↩
- 5RTHC-02165·Mason, Natasha L et al. (2019). “THC disrupted brain connectivity by boosting striatal glutamate and dopamine in occasional users.” European neuropsychopharmacology : the journal of the European College of Neuropsychopharmacology.Study breakdown →PubMed →↩
- 6RTHC-02250·Ranganathan, Mohini et al. (2019). “Your COMT gene variant determines how much THC impairs your working memory.” Psychopharmacology.Study breakdown →PubMed →↩
- 7RTHC-01245·Ramaekers, J G et al. (2016). “Cannabis and Cocaine Reduced Impulse Control and Brain Connectivity, But Only in People With Certain Genetics.” Brain imaging and behavior.Study breakdown →PubMed →↩
- 8RTHC-07953·Williams, Mollie V et al. (2025). “How Emergency Departments Handle Cannabis-Related Emergencies.” Emergency medicine practice.Study breakdown →PubMed →↩
What the Research Shows
This section synthesizes 328 peer-reviewed studies on Cannabis Effects and Pharmacology. Stronger evidence means more consistency across study types.
Mega-analysis of 400 IV THC infusions found psychosis-like symptoms in 45% of healthy volunteers, with effects increasing with dose and decreasing with regular cannabis use history
Strong EvidenceMeta-analysis of 372 participants found THC's brain effects are dose-dependent and track with CB1 receptor density across regions
Strong EvidenceMeta-analysis of 28 studies found blood and saliva THC levels are poor predictors of driving impairment, with negligible to weak correlations that disappear entirely in regular cannabis users
Strong EvidenceWhere Scientists Disagree
Areas where research shows conflicting results or ongoing scientific debate.
Data from 120 subjects showed cannabis tolerance develops and fades quickly, while withdrawal symptoms including insomnia, irritability, and tremor appeared after as few as 7 days of use
Moderate EvidenceReview finding cannabis increases heart rate with rapid tolerance development, poses minimal risk for young healthy users but significant risks for people with existing cardiovascular disease
Moderate EvidenceReview of animal studies found cannabinoid tolerance develops through receptor down-regulation, withdrawal symptoms are generally milder than with other drugs, and tolerant animals showed no increased vulnerability to morphine
Moderate EvidenceControlled study of 23 marijuana users found varying CBC and CBD concentrations did not change the effects of smoked marijuana, confirming THC as the primary active ingredient
Moderate EvidenceWhat We Still Don't Know
- Long-term prospective studies tracking outcomes over 5+ years are largely absent from the literature.
- Research on diverse populations (different ages, ethnicities, and medical backgrounds) remains limited.
Evidence Breakdown
Distribution of study types in this research area. Higher-tier evidence (meta-analyses, RCTs) provides stronger conclusions.
Research Timeline
How our understanding of this topic has evolved.
Pre-2000
3 studies published. Includes 1 RCTs.
2000–2009
12 studies published. Includes 3 RCTs, 3 strong-evidence studies.
2010–2014
22 studies published. Includes 7 RCTs.
2015–2019
52 studies published. Includes 12 RCTs, 5 strong-evidence studies.
2020–present
239 studies published. Includes 5 meta-analyses, 18 RCTs, 36 strong-evidence studies.