Quitting Weed While Pregnant: What You Need to Know
Withdrawal & Recovery
Crosses Placenta
THC crosses the placenta and reaches your baby's developing brain, where cannabinoid receptors guide neuron growth from early in fetal development, which is why ACOG recommends stopping all cannabis use during pregnancy.
ACOG Committee Opinion, 2017
ACOG Committee Opinion, 2017
View as imageIf you only read one thing
THC crosses the placenta — your baby is directly exposed every time you use. Your baby's brain has cannabinoid receptors from early in development, and THC can interfere with the growth those receptors are guiding. Withdrawal is uncomfortable but not dangerous to you or your baby, and it peaks in about a week. Pregnancy-safe nausea treatments exist if morning sickness is why you've been using. Talk to your provider — they can help you stop safely.
If you are pregnant and using cannabis, you are not alone. Between 2 and 5 percent of pregnant people self-report cannabis use (ACOG 2017, the American College of Obstetricians and Gynecologists), and that number is likely higher because of underreporting. Many people use cannabis for nausea, anxiety, sleep, or chronic pain, all of which can get worse during pregnancy. The idea of giving up something that helps you function is genuinely difficult, especially when you are already dealing with the physical and emotional demands of growing a human.
This guide is not here to shame you. It is here to give you clear, research-based information so you can make informed decisions. The science on cannabis and pregnancy is still evolving, but what exists consistently points in one direction: stopping is the safest choice for your baby.
Key Takeaways
- The American College of Obstetricians and Gynecologists (ACOG) recommends stopping cannabis during pregnancy and breastfeeding, and about 2 to 5 percent of pregnant people report still using
- THC crosses the placenta and reaches your developing baby, so your baby is directly exposed to cannabis compounds every time you use
- Cannabis withdrawal is real and hits roughly 47 percent of regular users, but it is temporary and manageable with the right support
- "Natural" does not mean safe during pregnancy — plenty of natural substances, from certain herbs to mercury in fish, are harmful to fetal development
- Quitting while pregnant is one of the most protective things you can do for your baby, and asking for help is nothing to be ashamed of
- Pregnancy-safe options for nausea like vitamin B6, doxylamine, and ondansetron exist and should be part of your quit plan conversation with your provider
What Medical Organizations Actually Recommend
The ACOG issued a formal committee opinion in 2017 recommending that "women who are pregnant or contemplating pregnancy should be encouraged to discontinue marijuana use." This was not a casual suggestion. ACOG also recommended that obstetricians and gynecologists screen pregnant patients for cannabis use and counsel them about the potential risks.
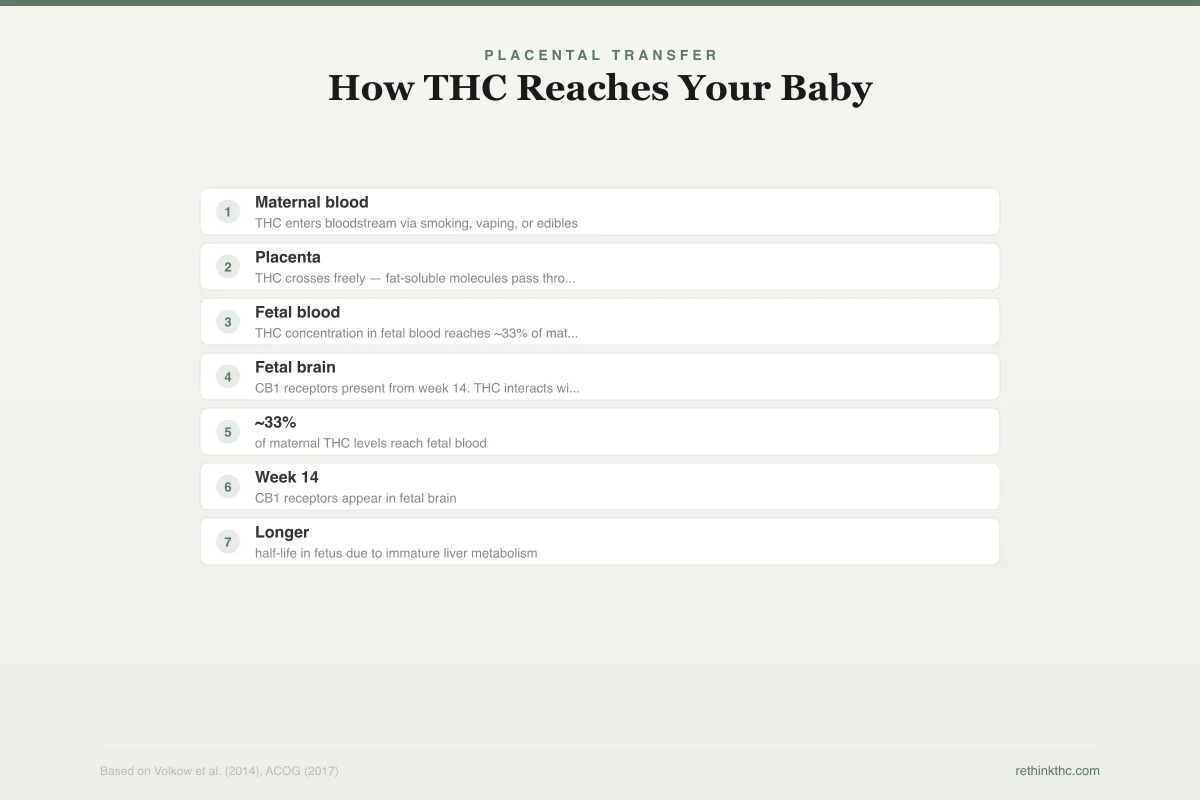
Placental Transfer
How THC Reaches Your Baby
THC is fat-soluble and crosses the placenta freely
Maternal blood
THC enters bloodstream via smoking, vaping, or edibles
Placenta
THC crosses freely — fat-soluble molecules pass through the placental barrier
Fetal blood
THC concentration in fetal blood reaches ~33% of maternal levels
Fetal brain
CB1 receptors present from week 14. THC interacts with developing endocannabinoid system.
~33%
of maternal THC levels reach fetal blood
Week 14
CB1 receptors appear in fetal brain
Longer
half-life in fetus due to immature liver metabolism
Your brain is fully formed. A fetal brain is actively under construction. THC interacts with a system building the architecture of your baby's nervous system.
The reason is straightforward. There is no established safe level of cannabis use during pregnancy. Unlike alcohol, where the research on fetal alcohol spectrum disorders is extensive and dose-response relationships are better understood, cannabis research during pregnancy has significant gaps. But the absence of a known safe threshold is not the same as evidence of safety. It means the safest approach, according to the best available evidence, is to stop.
Volkow's 2014 review in the New England Journal of Medicine highlighted the adverse health effects of cannabis use broadly and flagged prenatal exposure as an area of particular concern. The review noted that THC's ability to cross the placenta makes any level of maternal use a potential exposure for the fetus.
How THC Reaches Your Baby
THC is fat-soluble, meaning it dissolves in fat rather than water. This property allows it to cross biological barriers that water-soluble molecules cannot. The placenta, which filters many substances between your bloodstream and your baby's, does not fully block THC. When you consume cannabis in any form (smoking, vaping, edibles, topicals that enter your bloodstream), THC crosses the placenta and enters fetal circulation.
Your baby's developing brain has cannabinoid receptors (CB1 receptors) from early in fetal development. These receptors are part of the endocannabinoid system, a signaling network that plays a critical role in brain development, including neuron growth, migration, and the formation of connections between brain cells. When THC reaches these receptors in a developing brain, it can potentially interfere with processes that are supposed to be guided by your baby's own endocannabinoids, the natural compounds those receptors were designed to respond to.
This is different from how THC affects an adult brain. Your brain is fully formed. A fetal brain is actively under construction. The same compound that produces a temporary mood shift in you is interacting with a system that is building the architecture of your baby's nervous system.
Why "Natural" Does Not Mean Safe During Pregnancy
Cannabis is a plant. It grows in the ground. For many people, that association with nature makes it feel fundamentally different from pharmaceuticals or synthetic chemicals. The logic seems reasonable: how could something natural be harmful?
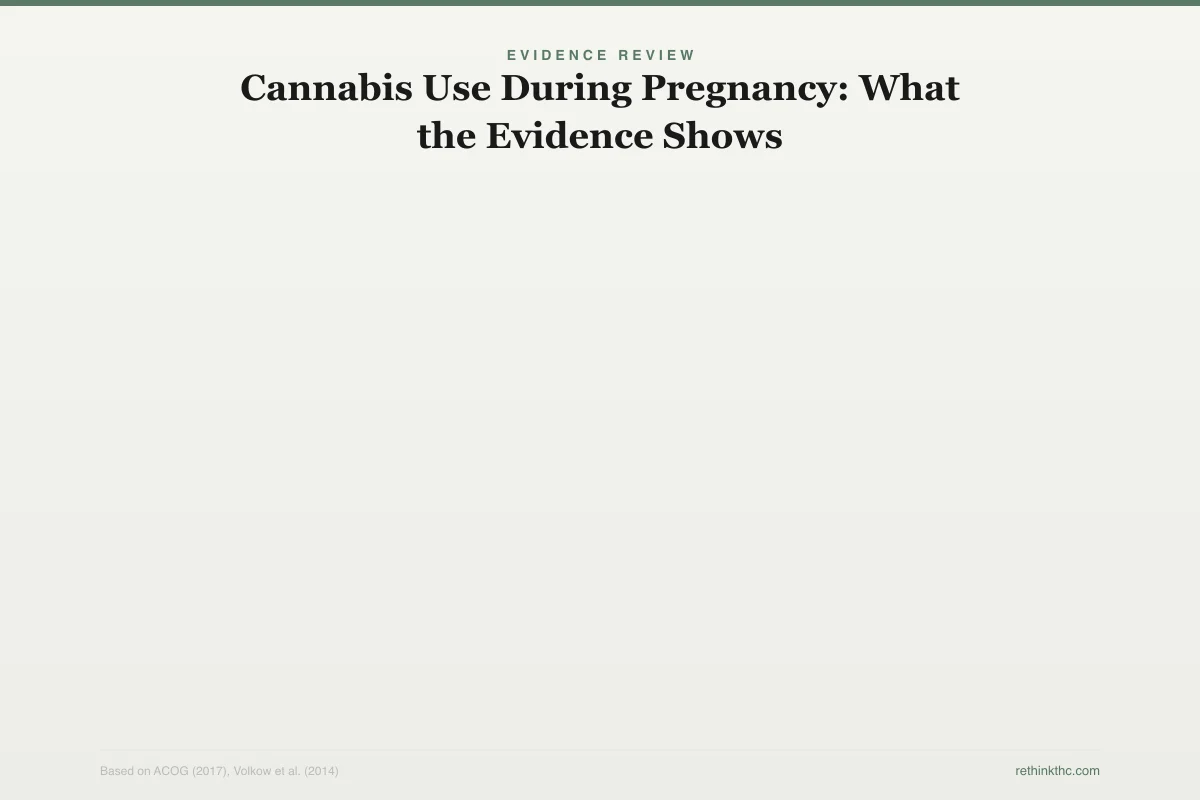
Evidence Review
Cannabis Use During Pregnancy: What the Evidence Shows
Research shows associations, not certainties — but the direction is consistent
Low birth weight
200–300g lower on average
Preterm birth
Mixed results across studies
NICU admission
Slightly increased risk
Developmental effects (age 3–6)
Attention and behavior differences
Cognitive outcomes
Insufficient data to draw conclusions
No established safe level of cannabis use during pregnancy. The absence of a known safe threshold is not the same as evidence of safety.
But pregnancy changes the safety equation for many natural substances. Certain herbal teas, essential oils, and foods that are perfectly safe for adults are not recommended during pregnancy. High levels of mercury in certain fish are natural. Listeria in unpasteurized cheese is natural. Lead in soil is natural. "Natural" describes where something comes from, not how it interacts with a developing fetus.
THC is a psychoactive compound that alters brain chemistry. The fact that it comes from a plant does not change its pharmacological activity. While cannabis does have proven medical benefits for certain conditions in adults, pregnancy is a context where the risk-benefit equation shifts dramatically. Your body processes it through the same metabolic pathways regardless of whether you think of it as a medicine, a recreational substance, or a plant. And your baby's developing system processes it too.
Cannabis Withdrawal During Pregnancy
One of the biggest concerns about quitting during pregnancy is withdrawal. If you have been using cannabis regularly, your body has adapted to its presence. Stopping can trigger a set of predictable symptoms that, while not dangerous, can feel miserable, especially on top of pregnancy symptoms.
Research by Budney in 2003, published in the Journal of Abnormal Psychology,[1] mapped the withdrawal timeline. Symptoms typically begin within days 1 to 3 of stopping, peak around days 2 to 6, and most resolve within 4 to 14 days. Bahji's 2020 meta-analysis in JAMA Network Open[2] found that roughly 47 percent of regular cannabis users experience withdrawal when they stop.
Common withdrawal symptoms include:
- Irritability and mood swings. These can overlap with normal pregnancy mood changes, making it hard to tell which is which.
- Nausea. Ironically, one of the reasons some pregnant people use cannabis is for nausea, and withdrawal can temporarily make nausea worse before it improves.
- Sleep disruption. Withdrawal-related insomnia can stack on top of pregnancy-related sleep difficulty.
- Anxiety. Heightened withdrawal anxiety is common and usually peaks in the first week.
- Appetite changes. Your appetite may drop temporarily, which can be concerning during pregnancy.
- Sweating and physical discomfort. These are typically mild and resolve quickly.
The important thing to know is that cannabis withdrawal, while uncomfortable, is not medically dangerous to you or your baby. The withdrawal itself does not cause complications. It is temporary, and it is far less risky than continued THC exposure during fetal development.
For a complete overview of what withdrawal looks like, the cannabis withdrawal complete guide covers every symptom in detail.
Managing Withdrawal Safely During Pregnancy
Some of the standard strategies for managing cannabis withdrawal need modification during pregnancy. Here is what works and what to discuss with your provider.
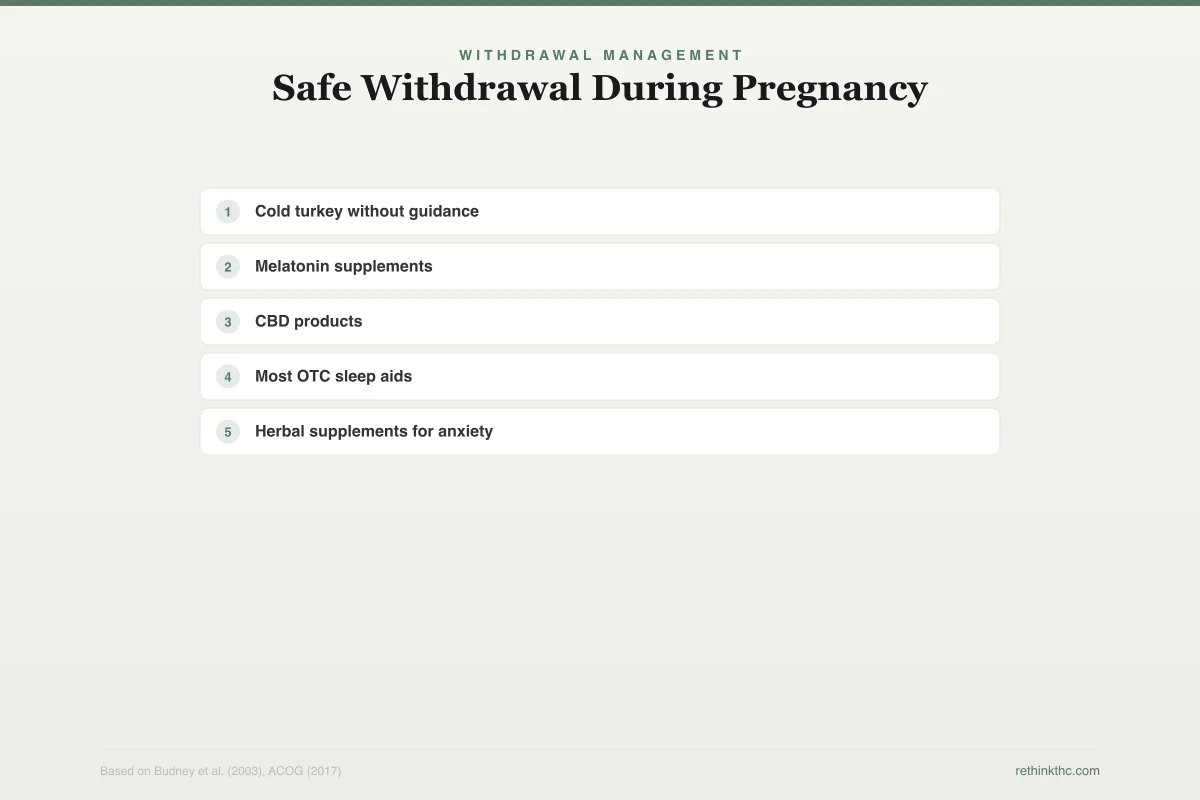
Withdrawal Management
Safe Withdrawal During Pregnancy
Pregnancy-specific strategies — always check with your provider first
Safe Approaches
- ✓Gradual taper over 1–2 weeks (talk to your OB about pacing)
- ✓Ginger or ginger tea for nausea (generally safe in moderate amounts)
- ✓Light exercise: walking, prenatal yoga, swimming
- ✓Consistent sleep hygiene: same bedtime, cool room, no screens before bed
- ✓Hydration and small frequent meals for appetite changes
- ✓Deep breathing and progressive muscle relaxation for anxiety
- ✓Let your support system know what you are going through
Discuss With Provider First
- ✕Cold turkey without guidance
May increase stress hormones — discuss approach with OB
- ✕Melatonin supplements
Limited safety data during pregnancy
- ✕CBD products
Limited pregnancy data, often contains undisclosed THC
- ✕Most OTC sleep aids
Check with your provider before taking anything
- ✕Herbal supplements for anxiety
Many herbs are not tested for pregnancy safety
Cannabis withdrawal is uncomfortable but not medically dangerous to you or your baby. The withdrawal itself does not cause pregnancy complications.
Talk to Your OB or Midwife
This is the most important step. Many people avoid telling their healthcare provider about cannabis use because they fear judgment or, in some states, legal consequences. But your provider needs accurate information to give you the best care. Most providers are far more supportive than you might expect, and they can help you create a plan that accounts for both withdrawal and pregnancy needs.
If you are worried about your provider's reaction, you can frame it directly: "I have been using cannabis and I want to stop. I need help managing the transition safely during my pregnancy."
Gradual Reduction vs. Stopping Immediately
For most people, stopping cannabis is medically appropriate at any point during pregnancy. However, if you are a heavy daily user and concerned about severe withdrawal symptoms, talk to your provider about whether a brief taper (gradually reducing over a few days) might be appropriate for your situation. The goal is to reach zero use as quickly as safely possible. For more on this decision, see the guide on cold turkey vs. tapering approaches.
Non-Pharmacological Symptom Management
Many of the supplements and over-the-counter remedies used for withdrawal are not tested for pregnancy safety. Stick to approaches that are safe during pregnancy:
- Ginger or ginger tea for nausea (generally considered safe in pregnancy in moderate amounts).
- Consistent sleep hygiene. Same bedtime, cool room, no screens before bed. This matters more than usual because both withdrawal and pregnancy disrupt sleep.
- Gentle exercise. Walking, prenatal yoga, or swimming can help with anxiety, mood, and sleep.
- Hydration and small frequent meals. These help with both withdrawal appetite changes and pregnancy nausea.
- Deep breathing and relaxation techniques. Progressive muscle relaxation and diaphragmatic breathing are safe, free, and effective for withdrawal anxiety.
Let Your Support System Know
If you have a partner, close friend, or family member you trust, let them know what you are going through. Withdrawal irritability combined with pregnancy hormones can strain relationships. Giving the people around you context ("I am quitting cannabis and the first two weeks might be rough") helps them support you instead of taking your mood shifts personally.
What About Using CBD Instead
CBD (cannabidiol) is the non-psychoactive compound in cannabis, and some people consider switching to CBD products during pregnancy as a compromise. However, ACOG's recommendation covers all cannabis products, not just THC. The research on CBD during pregnancy is extremely limited, and CBD products are not well regulated, meaning they may contain undisclosed THC or contaminants.
Until more research establishes a safety profile for CBD during pregnancy, most providers recommend avoiding it. For more on the differences between these compounds, see the CBD vs. THC guide.
What About Breastfeeding
ACOG's 2017 recommendation also covers lactation. THC is secreted into breast milk, and because THC is fat-soluble and breast milk is high in fat, concentrations can be significant. Your baby's brain continues developing rapidly after birth, and the same concerns about CB1 receptor interference apply during breastfeeding. If you have older children and are wondering how to navigate these conversations as a family, the guide on how to talk to your teenager about weed offers a research-based framework.
Medical Consensus
What Major Medical Organizations Recommend
Every major health organization advises against cannabis during pregnancy
American College of Obstetricians and Gynecologists
2017Recommends stopping. Screen and counsel all pregnant patients.
American Academy of Pediatrics
2018Recommends against all use during pregnancy and lactation.
World Health Organization
2016Advises against cannabis use during pregnancy.
U.S. Food and Drug Administration
2019Warns against use during pregnancy and breastfeeding.
Centers for Disease Control and Prevention
2020Recommends abstinence from cannabis during pregnancy.
Unanimous recommendation: discontinue cannabis use during pregnancy and breastfeeding
The research here is still limited, but the precautionary approach recommended by ACOG and the American Academy of Pediatrics is to avoid cannabis use during breastfeeding. For a detailed look at what the research shows about THC concentrations in breast milk and how long they persist, see weed and breastfeeding: THC in breast milk.
The Guilt Factor
If you used cannabis during part of your pregnancy before deciding to quit, you may be dealing with guilt or anxiety about potential harm. This is an understandable reaction, but it is worth putting into perspective.
The research on cannabis and pregnancy outcomes shows associations, not certainties. Using cannabis for part of a pregnancy does not mean your baby will have problems. Stopping when you can is the proactive, protective thing to do. The fact that you are reading this and considering your options means you are already making decisions in your baby's interest.
Guilt is not useful if it paralyzes you or makes you avoid getting help. Channel that energy into the next step: talking to your provider, making a quit plan, and lining up support.
The Nausea Problem
This deserves its own section because it is the most common reason pregnant people give for using cannabis. Pregnancy nausea (often called morning sickness, though it can last all day) ranges from mildly annoying to completely debilitating. For people with hyperemesis gravidarum, a severe form of pregnancy nausea, the desperation for relief is real.
Cannabis does suppress nausea in many people. But there are pregnancy-safe alternatives that your provider can prescribe, including vitamin B6, doxylamine (Unisom), ondansetron (Zofran) in certain cases, and other antiemetics. If nausea is the reason you have been using cannabis, replacing it with a pregnancy-safe treatment, rather than just white-knuckling through, makes quitting significantly more achievable.
Tell your provider specifically that nausea management is part of your quit plan. They have tools for this.
Timeline: What to Expect When You Stop
Based on Budney's 2003 research and the broader withdrawal literature:
Days 1 to 3. Withdrawal symptoms begin. Irritability, anxiety, and sleep disruption are usually the first to appear. Nausea may temporarily increase.
Days 2 to 6. Peak symptom severity. This is the hardest stretch. Remind yourself it is temporary.
Days 7 to 14. Gradual improvement. Most physical symptoms are fading. Mood is stabilizing. Sleep is still disrupted but improving.
Weeks 3 to 4. Most people feel significantly better. Cravings may persist but are less intense. Your CB1 receptors are actively recovering and normalizing.
By day 28. Research by Hirvonen in 2012, published in Molecular Psychiatry,[3] showed that CB1 receptors return to normal density after approximately 28 days of abstinence. Your brain's cannabinoid system is resetting.
The full withdrawal process is covered in the withdrawal timeline guide.
When to Seek Professional Help
Talk to your healthcare provider if:
- You are unable to stop using cannabis on your own despite wanting to
- Withdrawal symptoms are severe enough to interfere with eating, sleeping, or daily functioning
- You are experiencing significant anxiety or depression during the quitting process
- You have a history of mental health conditions that cannabis was managing
- You are using cannabis alongside other substances
Your OB, midwife, or a maternal mental health specialist can provide support tailored to pregnancy. Many areas also have substance use counselors who specialize in working with pregnant people.
Safety
ModerateWhen to involve your provider immediately
Concern
If you can't stop using despite wanting to, if withdrawal symptoms are severe enough to prevent eating or sleeping, if you're experiencing significant anxiety or depression, or if you're using cannabis alongside other substances — these situations need provider involvement, not just willpower.
What the research says
Your OB or midwife can help manage withdrawal symptoms safely during pregnancy, prescribe pregnancy-safe nausea and anxiety treatments, and connect you with substance use counselors who specialize in working with pregnant people. You will not be judged for asking.
Particularly relevant for: Any pregnant person struggling to quit cannabis on their own
What to do
Tell your provider. Frame it as: 'I want to stop and I need help doing it safely.' SAMHSA helpline: 1-800-662-4357 (free, confidential, 24/7).
ACOG Committee Opinion No. 722 (2017)
SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day, 7 days a week. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
You Are Making the Right Call
Quitting cannabis during pregnancy is not easy, especially if it has been helping you manage real symptoms. But the research consistently supports one conclusion: stopping is the safest choice for your developing baby. If you are still in the planning stages, the broader guide on quitting weed and pregnancy covers what to consider before and during conception. Withdrawal is temporary. The discomfort of the first two weeks is a finite cost for a significant benefit.
You do not have to do this alone. Talk to your provider, lean on your support system, and give yourself credit for making a hard decision. The fact that you are researching this topic means you are already taking it seriously. That matters.
The Bottom Line
ACOG recommends discontinuing all cannabis use during pregnancy and breastfeeding. THC is fat-soluble and crosses the placenta, reaching the fetal brain where CB1 receptors are present from early development and play a critical role in neuron growth and connectivity. Self-reported cannabis use during pregnancy is 2 to 5%, likely higher due to underreporting. Cannabis withdrawal is uncomfortable but not medically dangerous during pregnancy, with symptoms peaking around days 2 to 6 and resolving within 2 to 4 weeks. About 47% of regular users experience withdrawal. Pregnancy-safe nausea alternatives (vitamin B6, doxylamine, ondansetron) can replace cannabis for morning sickness management. CBD products are also not recommended during pregnancy due to insufficient safety data and poor regulation. The safest approach is to stop use as quickly as possible with provider guidance.
Sources & References
- 1RTHC-00134·Budney, Alan J. et al. (2003). “When Heavy Users Quit Cannabis, Symptoms Show Up Fast and Ease Within Two Weeks.” Journal of Abnormal Psychology.Study breakdown →PubMed →↩
- 2RTHC-02407·Bahji, Anees et al. (2020). “About Half of Heavy Cannabis Users Experience Withdrawal. This Meta-Analysis Measured It..” JAMA Network Open.Study breakdown →PubMed →↩
- 3RTHC-00573·Hirvonen, Jussi et al. (2012). “Daily Cannabis Use Was Linked to Fewer CB1 Receptors. A Month Without Brought Them Back..” Molecular Psychiatry.Study breakdown →PubMed →↩