How to Talk to Your Teenager About Weed (Without Losing Them)
Balanced Cannabis Science
Backfire Risk
Scare-based drug prevention approaches show little to no effect on teen behavior and can increase curiosity, while conversations grounded in verifiable evidence keep the door open for honest dialogue.
Meier et al., PNAS, 2012
Meier et al., PNAS, 2012
View as imageIf you only read one thing
Skip the lecture. Ask your teenager what they already know and what their friends think — then share specific studies they can actually look up. The Dunedin study followed 1,037 people for 38 years and found that regular teen users lost 8 IQ points that didn't come back. That's not a scare tactic, it's data. If they're already using, harm reduction beats demanding they stop cold. The real goal isn't controlling their behavior — it's staying the person they come to when things get complicated.
Talking to your teenager about cannabis is one of the more genuinely difficult parenting conversations you will have, and most of the standard advice makes it harder than it needs to be. The lecture model (sit down, here are the facts, here is what I expect) treats your teenager as a passive recipient of your wisdom, and teenagers are not passive recipients of much. What actually works is different, and it starts with understanding why the conventional approach tends to fail.
Key Takeaways
- Scare tactics and lectures usually backfire with teenagers — they either get defensive or nod along while pushing the real conversation underground
- Teens respond better to evidence they can verify than to moral arguments — the Meier IQ study and Di Forti psychosis data are specific, credible, and hard to wave off
- Leading with genuine curiosity about what they already know and believe opens doors that lecturing slams shut
- If your teenager is already using, harm reduction is more practical than demanding instant abstinence
- Keeping the relationship intact matters more than winning any single argument — a teenager who tells you the truth is in a much safer position than one who hides everything
- Practical harm reduction steps — cutting back frequency, avoiding high-potency products, never driving impaired — do more good than demands for abstinence when compliance is uncertain
Why Scare Tactics Backfire
Teenagers are unusually sensitive to what researchers call perceived credibility. When someone oversells a case or makes claims that do not match observable reality, teenagers discount not just that claim but the person making it.
Communication Guide
Talking to Teens About Cannabis
Avoid
- ✕Lecture or monologue
- ✕Use scare tactics or exaggerate risks
- ✕Claim all use equals addiction
- ✕Say "because I said so"
- ✕Bring it up when angry or reactive
Instead
- ✓Ask open-ended questions first
- ✓Share specific studies they can verify
- ✓Acknowledge complexity honestly
- ✓Set clear boundaries with reasons
- ✓Revisit the conversation regularly
Goal: stay a trusted resource, not win an argument. A teen who tells you the truth is safer than one who hides it.
This is the problem with traditional drug education approaches. When teenagers hear dramatic warnings about cannabis that contradict what they see in real life (adults who seem to use it without obvious catastrophe, friends who smoke and are still functioning), they do not update toward caution. They update toward ignoring the source.
A meta-analysis of school-based drug prevention programs found that scare-based approaches often show little to no effect on actual use behavior and can sometimes increase curiosity. The message teenagers take away from overstated danger claims is not "I should be careful." It is "adults will say whatever they think will control me, so I should figure this out myself."
This matters for parents specifically because your credibility is finite and precious. Once you have spent it on claims your teenager perceives as exaggerated, you lose access to the more important conversation.
The alternative is not minimizing the real risks. The real risks are substantial and worth taking seriously. The alternative is presenting those risks accurately and specifically, in terms your teenager can verify and engage with. That is a much harder conversation to dismiss.
Leading With Curiosity
Before you say anything, ask something. This is not a technique. It is a genuine acknowledgment that your teenager already has information, opinions, and experiences around cannabis, and that understanding where they actually are is more useful than delivering a prepared message.
Questions that open conversations:
- "What do your friends actually think about weed? Like, what is their take on it?"
- "Do you think there is a difference between how it affects teenagers versus adults?"
- "What have you heard about why it might or might not be a problem?"
These are not trick questions. They are genuine requests for information. When you ask them and then actually listen without immediately responding with your prepared counter-argument, several things happen. Your teenager experiences you as curious rather than combative. You learn what they actually believe, which is essential for any response to land. And you model the kind of thinking you want them to apply to the topic: taking evidence seriously rather than defaulting to peer consensus.
The instinct to fill silences with your position is strong. Resist it. Ask a follow-up. Reflect back what you heard. "So it sounds like you think most people use it without a real problem? I get why it seems that way. Here is what the research actually shows about that."
Arriving at your information through a door your teenager opened is much more effective than arriving through a door you forced.
The Science Worth Sharing
Here is what makes the cannabis-and-developing-brain conversation genuinely different from most drug prevention messaging: the science is real, specific, and independently verifiable. You are not asking your teenager to trust your authority. You are sharing data they can look up.
The Dunedin Study
The most important study to know is the Meier 2012 research published in PNAS.[1] Researchers followed 1,037 people born in Dunedin, New Zealand, from birth to age 38, measuring their IQ before cannabis use began and again at midlife.
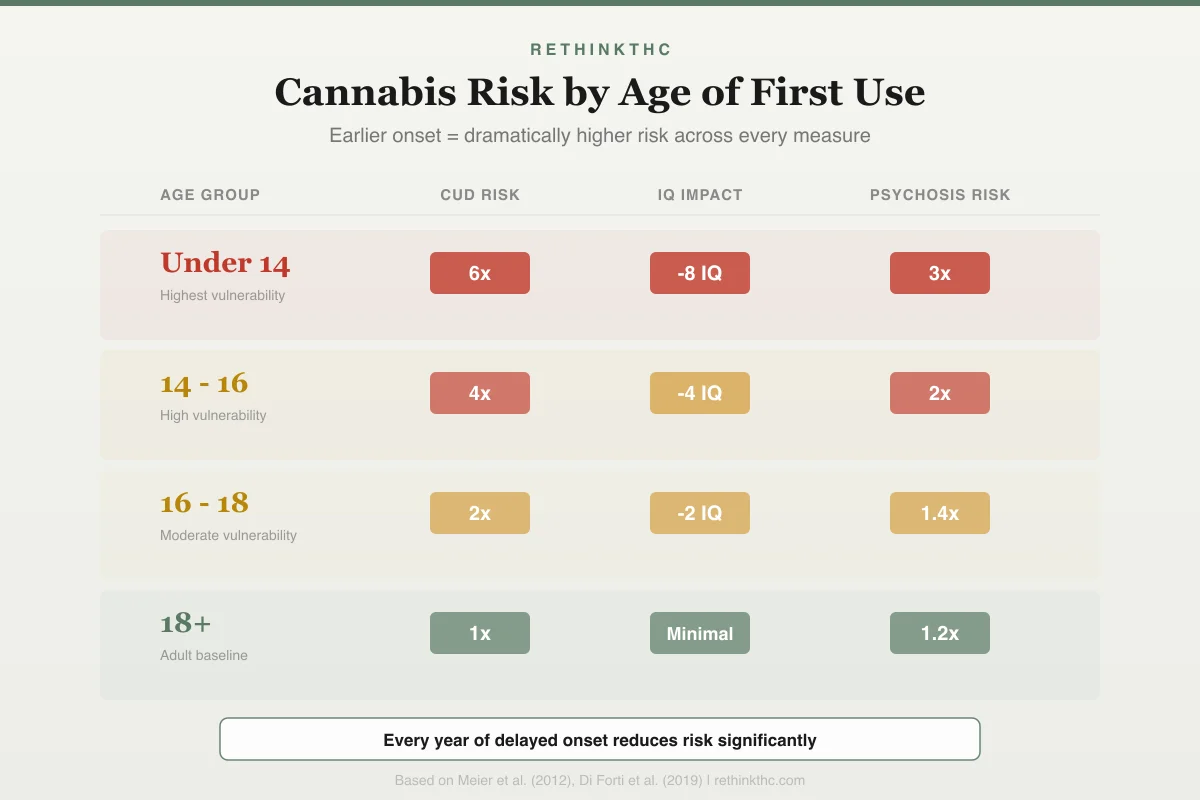
People who began using cannabis regularly during adolescence and continued persistent use showed an average 8-point IQ decline from childhood to midlife. People who began using as adults did not show the same pattern. The decline did not fully reverse even after a year or more of reduced use.
Eight IQ points is the difference between being at the 50th percentile and roughly the 29th percentile. That is a shift you would notice in academic performance, problem-solving speed, and the ease with which you process complex information.
When you share this with your teenager, be specific: 1,037 people, followed for 38 years, with IQ tested before any cannabis use began. This is not a laboratory study using theoretical exposure. It is 38 years of real life. It is very hard to dismiss.
The key detail that makes it relevant to their age and not yours: the decline was specific to adolescent-onset users. Adults who started using cannabis did not show the same pattern. This is not a universal cannabis risk. It is a developing-brain risk.
The Psychosis Data
The Di Forti 2019 study in The Lancet Psychiatry[2] examined 11 sites across Europe. The finding: daily cannabis use was associated with approximately a threefold increased risk of experiencing a first episode of psychosis. Daily use of high-potency cannabis, defined as THC above 10%, pushed that risk to approximately fivefold.
This matters for the potency conversation. A 2016 analysis by ElSohly and colleagues in Biological Psychiatry[3] found that average THC content roughly tripled between 1995 and 2014, from about 4% to about 12%. Current dispensary products often test at 20 to 30% THC. This means most teenagers are accessing cannabis that exceeds the "high-potency" threshold in the Di Forti study.
Presenting this to your teenager: "The study that found a fivefold increase in psychosis risk defined high-potency as THC above 10%. Most of the stuff people are actually using today is 20 to 30% THC. The research on what that level of exposure does to a developing brain has not caught up yet, because the products are too new. But the direction of the data is not encouraging."
The Dependence Rate
A 2014 review by Volkow and colleagues in the New England Journal of Medicine noted that approximately 17% of people who begin using cannabis as teenagers develop dependence. The rate for adult-onset users is about 9%. The developing brain is roughly twice as likely to develop a problematic relationship with cannabis as the fully developed brain.
This is useful for the "it is not addictive" conversation that will almost certainly come up. Cannabis can produce dependence in a meaningful proportion of users, and that proportion is significantly higher for adolescent-onset users.
Engaging With What Their Friends Are Saying
Your teenager's social environment has its own information ecosystem, and it is worth knowing what arguments they are likely to have already absorbed.
Even if your teenager is not using, they may be navigating a social environment where their friends are. The my kid's friends smoke weed guide covers how to help your teenager handle peer pressure without isolating them from their social circle.
"Everyone uses it and they are fine." This is individual observation being used to dismiss population-level data. Some people smoke cigarettes their whole lives and never get cancer. The population-level data is still worth paying attention to. Ask: "If the same percentage of people who used it got hurt as we see in the research, and those injuries just were not immediately visible, how would you know from looking at your friends right now?"
"It is natural, so it is safe." Many things that are natural are also dangerous. The "natural" argument does not track. What matters is the specific neurochemical effects on a developing brain, which the research documents clearly regardless of where the compound comes from.
"Alcohol is worse and that is legal." This is a legitimate observation about policy inconsistency, and engaging with it honestly rather than dismissing it will earn you credibility. Alcohol is genuinely harmful, and the policy treatment of alcohol versus cannabis is not strictly rational. That acknowledged: "The fact that alcohol causes harm does not make cannabis safe. Both carry real risks for developing brains. The research on adolescent alcohol use is also concerning. I would rather you waited on both."
"You can not overdose on it." True in the sense of fatal toxicity, but the absence of lethal overdose does not mean the absence of harm. The IQ data, the dependence data, and the psychosis data are all real harms that do not require an overdose to occur.
"What if my teenager says I used to smoke weed?" This is one of the hardest conversations, especially if you still use. If you are a parent who uses cannabis and is trying to figure out how to have this conversation authentically, the I smoke but don't want my kids to guide addresses that tension directly. And if this conversation has prompted you to reconsider your own use, quitting weed as a parent covers the unique challenges and motivations that come with that decision.
"Studies can say anything." When a teenager says this, they are often repeating a general cultural skepticism about research rather than engaging with specific methodological concerns. Ask them what would make a study credible. The Dunedin study followed 1,037 people for 38 years. What would they need to see to take that seriously?
If They Are Already Using
If your teenager is already using cannabis, a different approach is needed than for a teenager who has not yet started.
First, resist the impulse to immediately escalate to consequences. If you have just discovered or they have just disclosed that they have used cannabis, your response to that moment determines every future disclosure. Staying regulated and curious rather than reactive keeps the relationship intact.
Ask what has been happening. Not in an interrogation mode, but genuinely: how often, what kind of product, in what context. You need this information to respond proportionately, and they need to see that telling you the truth does not immediately trigger punishment.
If use is occasional and your teenager is otherwise functioning well (grades, relationships, sleep, affect), the most important thing is maintaining honest communication and setting clear expectations about what you want. "I want you to stop, and here is why, and here is what I need you to understand" is a reasonable response to occasional experimentation.
If you have discovered that your teenager is actively smoking weed and you need guidance on next steps, the my kid is smoking weed parent guide covers the specific interventions and conversations that situation calls for.
If use is frequent, daily, or appears to be affecting your teenager's functioning (declining grades, mood changes, withdrawal from activities, disrupted sleep), that warrants more direct intervention. A conversation with their pediatrician or a therapist who specializes in adolescent substance use is worth having. The quitting weed as a teenager or young adult guide covers what the process looks like for developing brains specifically. This is not a crisis that requires emergency response, but it is a situation that benefits from professional guidance. The signs of cannabis use disorder are worth reviewing. If your child has autism and you are navigating questions about cannabis use in that context, the cannabis and autism families research guide covers what the evidence shows and does not show.
For harm reduction if they are going to continue using despite your preferences:
- Frequency matters significantly. Occasional use carries different risk than daily use.
- Potency matters. Lower-potency products carry meaningfully less risk than high-potency concentrates.
- Vape cartridges purchased informally carry contamination risks beyond the THC exposure. Laced products are a documented real-world risk, not a hypothetical.
Safety
ModerateUnregulated vape cartridges carry real contamination risk
Concern
Vape cartridges purchased outside regulated dispensaries may contain vitamin E acetate, heavy metals, pesticides, or synthetic cannabinoids. The 2019 EVALI outbreak hospitalized over 2,800 people and killed 68, mostly from black-market THC cartridges.
What the research says
If a teenager is going to vape despite your preferences, cartridges from licensed dispensaries are meaningfully safer than street-purchased ones. This is not an endorsement — it is a contamination risk that is worth naming directly.
Particularly relevant for: Any teenager using vape cartridges from informal sources
What to do
If your teenager is vaping, have a separate conversation specifically about where their cartridges come from. This is a distinct safety issue from the THC exposure itself.
CDC EVALI investigation (2019-2020); state contamination testing data
- Using never means driving, operating equipment, or being in situations where impaired judgment creates physical danger.
Harm reduction is not endorsement. It is an acknowledgment that your influence over your teenager's behavior is real but limited, and that keeping them safer within their actual choices is better than only engaging with the theoretical choice where they do exactly what you want.
Maintaining the Relationship
The most important thing this conversation is protecting is not your teenager's immediate behavior. It is your position as someone they come to when things get complicated.
A teenager who hides their cannabis use from you is not safer than one who tells you the truth. They are more isolated from adult guidance at exactly the moments when they might need it most. The goal of these conversations is not to achieve compliance. It is to remain a trusted resource.
That means saying things like:
- "I would rather you come to me with the truth, even if it is not what I want to hear, than have you hide it because you are worried about my reaction."
- "You are not going to lose my trust by being honest with me. You might lose it by lying to me."
- "I do not expect to control everything you do. I do expect you to know where I stand and to think seriously about why."
It also means being willing to revisit the conversation, to update your view when new information comes in, and to acknowledge uncertainty where it genuinely exists. The research on adolescent cannabis use is real and concerning. It is also not complete, and modern potency levels have outpaced the research. You do not have to pretend more certainty than the evidence warrants. Honest uncertainty is more credible than false confidence.
The developing brain article goes into the neuroscience in more detail if your teenager wants to look at the underlying biology, and the endocannabinoid system piece explains how THC actually works in terms they can engage with.
When to Seek Professional Help
If your teenager is using daily, showing signs that cannabis use is affecting their daily functioning, expressing that they have tried to stop and cannot, or showing mood changes, paranoia, or detachment from their usual life, it is worth bringing in professional support. A pediatrician or adolescent health specialist can assess the situation without judgment and provide guidance tailored to the developing brain.
Family therapy can also help when the communication around this topic has become a source of significant conflict in your household.
SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day, 7 days a week. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
The Bottom Line
Scare tactics and lectures typically backfire with teenagers, producing defensiveness or surface compliance while pushing real conversation underground. Teenagers respond better to verifiable evidence than moral arguments. The Meier Dunedin study (1,037 people followed for 38 years) found that persistent adolescent-onset cannabis use was linked to an 8-point IQ decline that did not fully reverse. The Di Forti study found daily high-potency cannabis use carries a fivefold increase in psychosis risk. Cannabis potency has tripled since 1995, meaning most current products exceed the "high-potency" threshold used in research. Effective parent-teen conversations lead with curiosity rather than interrogation, share specific verifiable science rather than vague warnings, and engage honestly with the arguments teenagers have already absorbed from their social environment. If a teenager is already using, harm reduction strategies are more practical than demanding immediate abstinence.
Sources & References
- 1RTHC-00591·Meier, Madeline H. et al. (2012). “From Teen Years to 38: Heavy, Long-Term Cannabis Use Tracked With Lower Cognitive Scores.” Proceedings of the National Academy of Sciences (PNAS).Study breakdown →PubMed →↩
- 2RTHC-02010·Di Forti, Marta et al. (2019). “Daily High-Potency Cannabis Use and Psychosis Risk: The Largest European Study Drew a Direct Line.” The Lancet Psychiatry.Study breakdown →PubMed →↩
- 3RTHC-01144·ElSohly, Mahmoud A. et al. (2016). “U.S. Cannabis Potency Tripled Over Two Decades While CBD Nearly Vanished.” Biological Psychiatry.Study breakdown →PubMed →↩