Using Weed Under 18: What It Does to Your Developing Brain
Balanced Cannabis Science
8-Point IQ Drop
A landmark study of 1,037 people from birth to age 38 found that persistent cannabis use starting before 18 was linked to an 8-point IQ decline that did not fully reverse even after quitting.
Meier et al., PNAS, 2012
Meier et al., PNAS, 2012
View as imageIf you only read one thing
Your brain isn't finished building until around age 25. THC binds to receptors in exactly the parts still under construction — the ones that handle decisions, memory, and impulse control. A major study tracking 1,037 people from birth to age 38 found that regular teen use was tied to an 8-point IQ drop that didn't fully come back even after quitting. This doesn't mean one joint ruins your brain. It means daily use during the building years carries real risks that adult use doesn't. The earlier you stop, the more time your brain has to finish building properly.
If you are under 18 and using weed, or you know someone who is, the single most important thing to understand is that the teenage brain and the adult brain are not the same organ. They look the same on the outside. They feel the same from the inside. But at the cellular level, the teenage brain is still under construction, and introducing THC during that construction window creates risks that simply do not apply to someone in their 30s. This is not a scare tactic. It is neurobiology.
Key Takeaways
- Your brain keeps building itself until around age 25, and the prefrontal cortex — the part that handles decisions, planning, and impulse control — is the last piece to finish
- A major study that followed 1,037 people from birth to age 38 found that persistent cannabis use starting before 18 was tied to an 8-point IQ drop that did not fully reverse after quitting
- Teen cannabis users still showed problems with memory, attention, planning, and processing speed even after going 3 to 4 weeks without using
- Daily use of high-potency cannabis carries a fivefold jump in psychosis risk, and younger brains appear to be more vulnerable
- Cannabis potency has roughly tripled since 1995, so today's products hit a developing brain much harder than what earlier research studied
- The earlier a teenager stops using, the more developmental time the brain has left to recover — because the prefrontal cortex keeps maturing until about age 25
Your Brain Is Still Being Built
The human brain does not finish developing until approximately age 25. The region that matures last is the prefrontal cortex (PFC), which sits behind your forehead and controls some of the most important functions you will ever need: decision-making, impulse control, planning ahead, and weighing consequences. At 15 or 16, your PFC is still years away from being fully wired.
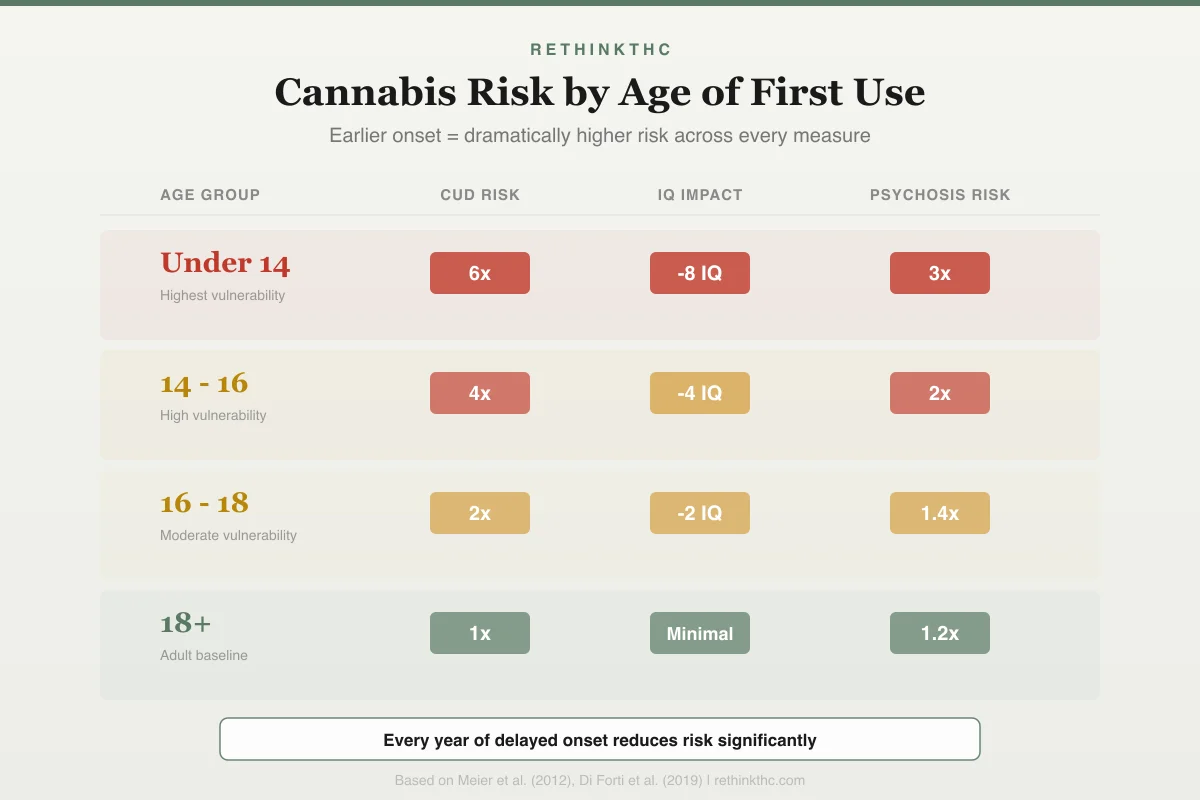
Risk by Age of First Use
Earlier Onset = Dramatically Higher Risk
Risk multipliers across three key measures
Under 14
Highest vulnerability
14 - 16
High vulnerability
16 - 18
Moderate vulnerability
18+
Adult baseline
Every year of delayed onset reduces risk significantly
Two processes are especially active during adolescence. The first is synaptic pruning, where the brain eliminates connections it does not use regularly and strengthens the ones it does. Think of it as your brain deciding which neural pathways become permanent highways and which get closed down. The second is myelination, where nerve fibers get coated in a fatty insulation called myelin that makes signals travel faster and more efficiently. Both of these processes are critical for building a brain that works well for the rest of your life.
THC works by binding to CB1 receptors, which are part of your endocannabinoid system. These receptors are heavily concentrated in exactly the regions still under construction during adolescence: the prefrontal cortex, the hippocampus (essential for forming memories), and the amygdala (involved in processing emotions and fear). When a substance repeatedly activates receptors in areas that are still being wired and pruned, it has the potential to change the trajectory of that wiring.
A 2014 review by Volkow and colleagues, published in the New England Journal of Medicine, flagged adolescent-onset cannabis use as a distinct risk category. The review found that approximately 17% of people who begin using cannabis as teenagers develop dependence, compared to about 9% of people who have ever tried it in the general population. The developing brain is not just more sensitive to THC. It is more likely to build a pattern of use that becomes difficult to stop.
The Study That Changed the Conversation
The most influential study on teenage cannabis use and long-term brain outcomes is the Meier 2012 study, published in PNAS (Proceedings of the National Academy of Sciences).[1] Researchers followed 1,037 people born in Dunedin, New Zealand, from birth to age 38, with a remarkable 96% retention rate. That means almost no one dropped out over nearly four decades. Participants had their IQ tested before cannabis use began and again at age 38.
The results were striking. People who started using cannabis regularly during adolescence and continued persistent use showed an average 8-point decline in IQ from childhood to midlife. That might not sound dramatic, but 8 IQ points is the difference between the 50th percentile and roughly the 29th percentile. It is a shift you would notice in academic performance, problem-solving, and professional capacity.
Several details make this finding especially significant. The decline was specific to adolescent-onset users. People who started using as adults did not show the same pattern. The decline was dose-dependent, meaning heavier and more persistent use was linked to greater cognitive losses. And most importantly, the IQ decline did not fully reverse even after participants reduced or stopped their use.[1]
The study accounted for education level, childhood socioeconomic status, and other substance use. Researchers also checked whether pre-existing cognitive differences might explain the pattern and found that the decline happened after cannabis use started, not before. This is not absolute proof of causation, but it is the strongest evidence we have from real-world longitudinal data.
Cognitive Effects That Stick Around
One common objection to cannabis-cognition research is that people were tested while they still had THC in their system. A 2009 study by Jacobus and colleagues addressed this directly. They tested adolescent cannabis users after 3 to 4 weeks of monitored abstinence, long enough for THC to clear the body.
Even after nearly a month without using, the teenage cannabis users showed deficits in memory, attention, planning, and psychomotor speed compared to their non-using peers. These are not abstract laboratory measurements. Memory affects how well you learn in school. Attention affects whether you can follow a conversation or finish a task. Planning is what lets you organize your day, manage deadlines, and think ahead. Psychomotor speed affects everything from driving reflexes to sports performance.
For comparison, a 2018 meta-analysis by Scott and colleagues, published in JAMA Psychiatry,[2] reviewed 69 studies on cannabis and cognition. The headline finding was that most cognitive deficits in the general cannabis-using population resolve within about 72 hours of abstinence. That is genuinely encouraging for adult users.
But the adolescent data tells a different story. When the Jacobus study found persistent deficits after 3 to 4 weeks, and the Dunedin study found incomplete IQ recovery after a year or more of reduced use, the pattern is clear: the developing brain does not bounce back the same way an adult brain does. If cannabis disrupts wiring during a critical window, some of that disruption may be structural rather than temporary.
This does not mean every teen who tries weed once is permanently affected. The research points to regular, persistent use as the risk factor. But if you are using daily or near-daily before age 18, the evidence suggests you are taking a gamble with your cognitive capacity that adult users are not taking.
Psychosis Risk Is Real, Especially for Young Users
The connection between cannabis and psychosis has been debated for years, but a 2019 study by Di Forti and colleagues, published in The Lancet Psychiatry,[3] provided unusually clear data. The study examined 11 sites across Europe and found that daily cannabis use was associated with approximately a threefold increased risk of experiencing a first episode of psychosis. Daily use of high-potency cannabis (THC above 10%) pushed that risk to approximately fivefold.
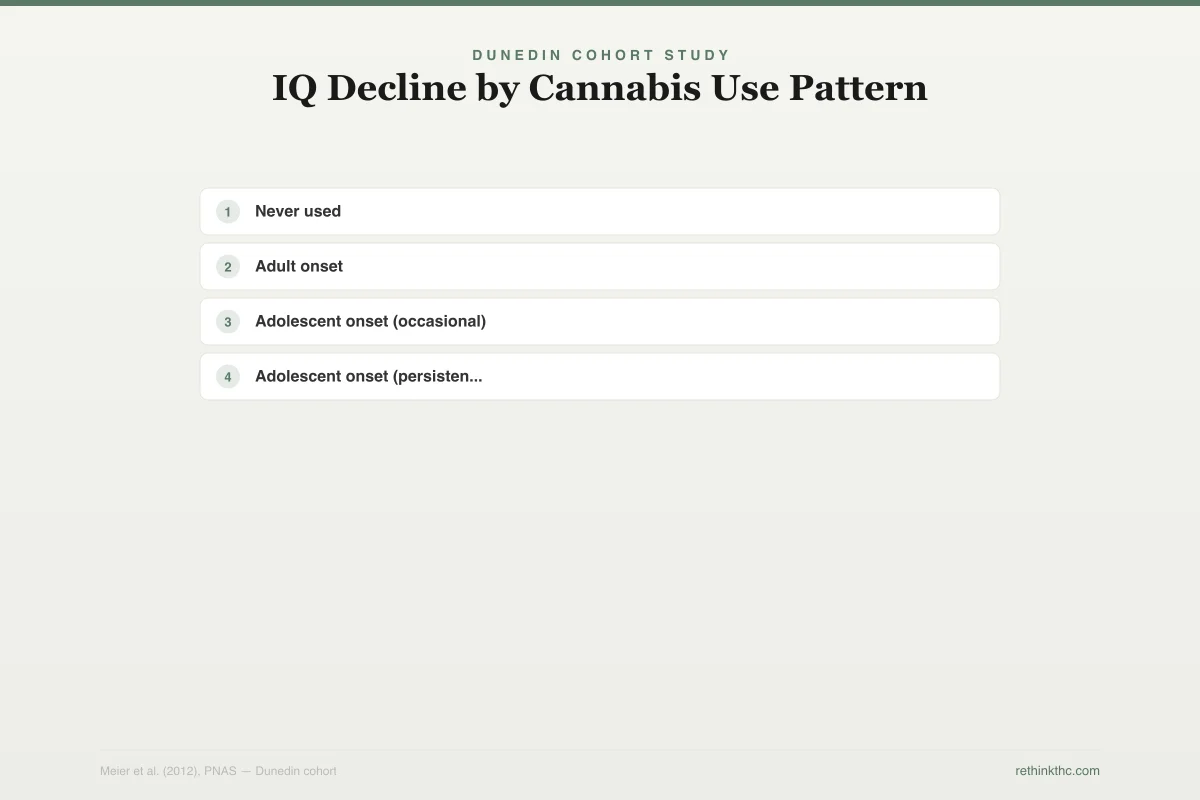
Dunedin Cohort Study
IQ Decline by Cannabis Use Pattern
1,037 people followed from birth to age 38
Never used
0 IQ points
Adult onset
-1.5 IQ points
Adolescent onset (occasional)
-3.5 IQ points
Adolescent onset (persistent, weekly+)
-8 IQ points
50th to 29th percentile
8 IQ points did not fully reverse even after a year or more of reduced use
For context, the baseline risk of psychosis in the general population is relatively low, roughly 1 to 3%. A fivefold increase still means most daily high-potency users will not develop psychosis. But for the minority who do, the consequences can be devastating, including hallucinations, delusions, and breaks from reality that require hospitalization.
Why does this matter more for teens? The developing brain is more vulnerable to disruptions in dopamine signaling, which is the neurochemical pathway most closely linked to psychotic experiences. THC increases dopamine release in ways that an immature brain may not be equipped to regulate properly.
If you have a family history of schizophrenia, bipolar disorder, or other psychotic disorders, the risk profile shifts significantly. Genetic predisposition combined with adolescent cannabis use is a combination the research consistently identifies as particularly concerning.
Safety
CriticalPsychosis risk in teens with family history
Concern
Daily use of high-potency cannabis carries a fivefold increase in first-episode psychosis risk. Adolescent brains are more vulnerable because their dopamine signaling systems are still maturing. For teens with a family history of schizophrenia or bipolar disorder, the combination of genetic predisposition and regular cannabis use is a particularly high-risk scenario.
What the research says
The baseline risk of psychosis is low (1-3%), so even a fivefold increase means most users won't develop it. But for the minority who do, consequences include hallucinations, delusions, and hospitalization.
Particularly relevant for: Daily teen users, especially those using high-potency products (>10% THC) or with family history of psychotic disorders
What to do
If you're a teen using daily and have any family history of psychotic disorders — stop or dramatically reduce use and talk to a healthcare provider. This is the highest-risk combination in the research.
Di Forti et al. (2019), The Lancet Psychiatry
Today's Weed Is Not Your Parents' Weed
A 2016 analysis by ElSohly and colleagues, published in Biological Psychiatry,[4] tracked the THC content of confiscated cannabis samples over two decades. Average THC roughly tripled between 1995 and 2014, rising from about 4% to about 12%. And that 12% average is from nearly a decade ago. Current dispensary flower often tests at 20 to 30% THC. Concentrates and dabs can reach 60 to 90%.
Meanwhile, CBD content (which may partially buffer some of THC's harsher effects) decreased. The ratio of THC to CBD shifted dramatically, creating a product that delivers a stronger, less balanced neurochemical impact than what was available when most of the major studies were conducted.
This is a critical point. The Dunedin study, the Jacobus study, and much of the foundational research was conducted with cannabis well under 10% THC. If developing brains showed vulnerability at those potency levels, the implications for today's products are concerning. The research has not yet caught up with the modern potency landscape, which means current findings may actually underestimate the risks for teenagers using today's cannabis.
The rise of vape pens makes this even more relevant. Vaping delivers THC more efficiently, hits faster, and is easier for teens to use discreetly. The combination of higher potency and more efficient delivery is a genuine concern from a neurodevelopmental perspective.
What Recovery Looks Like for Teens
The news is not all bleak. The brain retains significant neuroplasticity well into the mid-twenties, which means the construction project is still underway even if it has been disrupted. Stopping earlier gives the brain more runway to course-correct.
Research on CB1 receptor recovery shows that these receptors begin returning to normal within about 2 days of abstinence and largely normalize by approximately 28 days. This receptor-level recovery is the foundation for cognitive and emotional improvement after quitting.
For adults, the Scott 2018 meta-analysis[2] offers clear encouragement: most cognitive effects resolve within 72 hours. For adolescents, the picture is less certain. The Jacobus data showing persistent deficits after 3 to 4 weeks and the Dunedin data showing incomplete IQ recovery[1] suggest that adolescent recovery may be slower and less complete, particularly for persistent heavy users.
But slower does not mean impossible. The earlier you stop, the more developmental time your brain has left. If you are 16 and you stop now, your prefrontal cortex still has roughly nine years of development ahead of it. That is a meaningful window for recovery and adaptation. Resources like a tolerance break guide can help you structure the process, and understanding what to expect in the first week can make the transition less intimidating.
When to Seek Professional Help
If you or a teenager you know is using cannabis daily, having trouble stopping despite wanting to, experiencing memory problems or declining grades, or noticing paranoia, detachment from reality, or significant mood changes, it is worth connecting with a healthcare provider. These are not signs of moral failure. They are signals that a developing brain is responding to a chemical exposure in ways that could benefit from professional guidance.
A provider experienced with adolescent substance use can assess the situation without judgment and offer strategies that account for the unique challenges of the developing brain. Family involvement, when supportive rather than punitive, consistently improves outcomes.
SAMHSA's National Helpline is available at 1-800-662-4357. It is free, confidential, and available 24 hours a day, 7 days a week. You can also text "HELLO" to 741741 to reach the Crisis Text Line.
The Bottom Line
The adolescent brain is still under construction until approximately age 25, with the prefrontal cortex finishing last. Two critical processes, synaptic pruning and myelination, are actively reshaping neural architecture during this period. THC binds to CB1 receptors concentrated in the same regions undergoing development, potentially altering the brain's final wiring. The landmark Dunedin study (Meier 2012) found that persistent cannabis use starting before age 18 was linked to an 8-point IQ decline that did not fully reverse after quitting. Adolescent users showed persistent deficits in memory, attention, and planning even after 3 to 4 weeks of abstinence, while most adult cognitive deficits resolve within 72 hours. Daily high-potency cannabis use carries a fivefold increase in psychosis risk, with younger brains appearing more vulnerable. Cannabis potency has roughly tripled since 1995, and modern vape pens deliver THC more efficiently, compounding the concern. Recovery is possible but slower for adolescents, and stopping earlier gives the brain more developmental runway to course-correct.
Sources & References
- 1RTHC-00591·Meier, Madeline H. et al. (2012). “From Teen Years to 38: Heavy, Long-Term Cannabis Use Tracked With Lower Cognitive Scores.” Proceedings of the National Academy of Sciences (PNAS).Study breakdown →PubMed →↩
- 3RTHC-02010·Di Forti, Marta et al. (2019). “Daily High-Potency Cannabis Use and Psychosis Risk: The Largest European Study Drew a Direct Line.” The Lancet Psychiatry.Study breakdown →PubMed →↩
- 4RTHC-01144·ElSohly, Mahmoud A. et al. (2016). “U.S. Cannabis Potency Tripled Over Two Decades While CBD Nearly Vanished.” Biological Psychiatry.Study breakdown →PubMed →↩